Many patients of orthopedic dentists after prosthetics talk about how difficult it was for them to get used to dentures. High-quality permanent artificial teeth and crowns are compact in size and do not cause any discomfort. But with removable ones, problems arise: from unpleasant sensations in the palate and irritating pressure on the gums to constant nausea and even a gag reflex. Each patient experiences the adaptation process in his own way, so it can last only a couple of days, one or two weeks, or several months.
Why does discomfort occur?
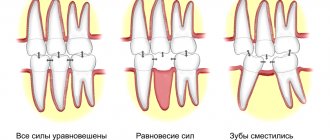
A person with missing teeth gets used to living without them. His dental system begins to distribute the chewing load differently, and the muscles, cheeks, nerves, tongue and jaw bones involved in the process gradually get used to the restructuring that has occurred.
If missing teeth can be restored with permanent dentures, the parameters of which are almost identical to natural teeth, the load when chewing food turns out to be natural. And the absence of foreign elements - fixing hooks and staples - guarantees the absence of irritation of the mucous membranes of the cheeks and tongue.
In removable structures, the chewing load is distributed differently. For example, popular clasp dentures distribute it to the palate and the remaining adjacent teeth. It is clear that the sensations when chewing food will be unusual at first and will almost certainly cause irritation.
Myths about crowns, or why are patients afraid of having crowns installed?
I often see fear and disappointment on the faces of patients when the word “crown” is mentioned. And I am sure that this is not unfounded. Almost every patient of mine has either a personal bad experience, indirectly or directly related to “crowns,” or his friends or relatives have such an experience. Let's try to understand the reasons for this unsuccessful experience using the example of questions and arguments that patients use to operate.
Myth one: “Teeth decay and rot under crowns”
Yes, this happens, and patients come to me with similar problems. The reasons may be different, but they are all quite understandable.
Reason one. Teeth that were severely damaged even before prosthetics. Unfortunately, crowns are sometimes offered to a patient in cases where, according to modern treatment protocols, it is time to remove a decayed tooth. Hence the problems - if a tooth is critically damaged by life, then the crown is only the final chord, which often does not last long. If a tooth is destroyed to the level of the gum (or under the gum), and there is no way to improve this situation, it is better to replace such a tooth with an implant while there is enough bone tissue around.
Reason two. Poor hygiene. If this is the cause of the destruction of healthy teeth, then no crown will save a weakened tooth from the effects of microorganisms.
Reason three. Neglect by the doctor of such an important clinical stage as the manufacture of intermediate crowns. People also call them “temporary”. For modern doctors, the stage of making “temporary” crowns is inextricably linked with the making of permanent ones. If you neglect it, problems may arise.
Reason four. Poor quality crowns that do not fit well to the tooth. When there is a large gap between the tooth and the crown, this will not lead to anything good. Plaque accumulates in the cracks, an unpleasant odor appears in these areas, and the gums begin to become inflamed.
Here is one example of a tooth being removed due to a huge gap formed by the edge of an old metal crown.
If desired, one could stick a finger into this gap. Now compare the fit of the old metal crown with this photo:
The crown-tooth boundary, even with high magnification, is visible only by the color transition. The microscopic gap is securely closed with fixing cement, like a sealant. This is the kind of fit that any modern crown should strive for.
Myth two: “The tooth needs to be ground down heavily for a crown.”
This is not entirely true. Currently, in modern dentistry it is customary to preserve tooth tissue as much as possible, as this improves the prognosis of restoration. Using magnification - an operating microscope and binoculars - the doctor has very good control over how much tooth tissue he removed during treatment. As a rule, for a modern design it is enough to remove 0.6-0.9 millimeters of tissue, depending on the clinical situation, and an adequate doctor always strives for these values.
In this photo there were 2 teeth side by side with different approaches to treatment for crowns. On the right is a tooth cut down excessively (the thickness of the removed tissue is about 2 mm), on the left is a tooth processed using magnification (the thickness of the removed tissue is 0.4-0.6 mm). Modern materials (metal-free ceramics) and magnification tools allow dentists to treat teeth 3-4 times more carefully. And this significantly affects their service life.
Myth three: “If anything happens, after the crown the only thing is removal.”
Let's look at the previous paragraph. If the boundary between the edge of the crown and the tooth is above the gum, if the grinding was done carefully under magnification, then re-prosthetizing such a tooth even after a long time is not a problem. If the tooth is destroyed even before prosthetics, then there is really nothing to hope for.
Myth four: “Teeth under crowns must be depulped (the nerve removed) and pins placed.”
This is an inveterate myth, which, unfortunately, is still reinforced by many dentists. I can only say that with the use of modern equipment, cooling, adequate temporary prosthetics and careful hands, it is possible to work on vital - “living” - teeth without any problems. But often it is not necessary to cover such teeth with a full crown - it is enough to make an inlay.
These four myths are often the most important arguments of patients “against” dental restoration with crowns. What happens when patients choose a “filling” instead of a crown, arguing that “if it falls out, I’ll put a new one”? A few photos will answer best:
And the reason for such fractures is that the load on the tooth is very serious, and many, including some dentists, do not take this into account. The crown allows you to distribute the chewing load more evenly and safely over the remaining part of the tooth, without leading to chipping of the walls. Whether it is worth risking a tooth and preferring a large composite filling to a durable, properly made ceramic crown, everyone decides for themselves.
And now I would like to give an example of work according to modern indications. The patient underwent endodontic treatment of the root canals of tooth 4.6 due to irreversible pulpitis, then a decision was made to make an indirect all-ceramic restoration (crown).
The “core” of the tooth was restored and it was prepared for a full crown:
View of the finished restoration in the oral cavity after a few weeks:
PS So, is the word “crown” really a death sentence for a tooth? In my opinion - no! And with my article I tried to prove this with examples. The procedure for making a crown in modern dentistry is a high-tech event aimed at preserving the tooth and its further long-term functioning. The use of water cooling during preparation and a rubber dam make the procedure quite comfortable for the patient. The doctor's use of magnification allows maximum control over the preparation process. And such a novelty as digital impressions saves the patient from what is perhaps the most unpleasant procedure in prosthetics. In the right hands, an indirect restoration (crown or inlay) can help protect the tooth from fracture. If they are wrong, they lead to problems and disappointments, which give rise to many myths. So, dear patients, choose your doctor carefully! Good luck to everyone!
Author of the article: Pavel Pola
Authors of photos of clinical cases: Pavel Pola and Kirill Kostin
What inconveniences can you encounter after prosthetics?
Dentists installing dentures in Moscow warn in advance about possible discomfort that may manifest itself:
- noticeably irritating sensation of a foreign body in the oral cavity;
- pain caused by the pressure of the structure on the supporting teeth and especially the gums;
- rubbing of mucous membranes, redness and swelling, formation of bedsores on the gums;
- a feeling of poor closure of the jaws and teeth;
- increased salivation caused by the perception of the prosthesis as food that needs to be easier to move from the mouth to the throat;
- the appearance of gagging as a reaction to the presence of a foreign body in the mouth;
- impaired diction, which can be caused by even the best removable dentures (the tongue needs time to get used to changing position when pronouncing sounds);
- partial loss of taste of products caused by the closure of certain areas of the oral mucosa by the prosthesis.
Treatment
If the prosthesis is mobile, the doctor must determine the degree of displacement and instability of the artificial tooth. If the reason is weakening of the fixation, the prosthesis or abutment is removed, after which the structure is reinstalled. If dismantling the coronal part is not possible, which could lead to serious damage, fixation is carried out using a drilled hole. The cavity is then closed with filling material.
If none of the above options is suitable, the crown must be removed altogether. It is cut, after which the fastening is checked, and the connecting part is repaired. To restore the row, a new prosthesis is made and installed in place.
In some cases, the cause of the problem is peri-implantitis. In such a situation, the doctor must preserve the bone tissue to eliminate complications and avoid the need to remove the implant. Treatment methods depend on the stage of the disease, bone condition and other factors. The following actions are usually taken to eliminate inflammatory processes:
- office cleaning, removal of plaque and stone;
- ultrasonic treatment, elimination of affected areas;
- bone grafting, for which barrier membranes and bone substitutes (natural or synthetic) are used;
- therapy aimed at protecting against pathogenic bacteria (general and local with treatment of the affected surface);
- hygiene using antiseptics;
- control using radiography.
After treatment is completed, re-prosthetics are performed. Extraction of the artificial root is required only in situations where implant failure occurs. You can insert a new pin after removing it, treating the hole, removing necrotic tissue and plastic surgery. In some cases, a new rod is placed in the old socket after completion of therapy. But there is no clear opinion among experts; it all depends on the condition of the tissues and other factors.
Prevention
To avoid complications, the patient after implantation must follow a number of rules regarding oral hygiene. Poor condition and poor care are the main reason for the development of complications, any diseases of soft tissues and bones.
After completing the treatment procedure, the Patient at home must do the following:
- brushing your teeth twice a day with soft brushes that are changed every two months;
- removing food debris using irrigators or electric brushes, rinsing with antibacterial solutions;
- using dental floss to remove plaque from the cervical area;
- the use of multi-beam, cylindrical, conical brushes;
- refusal of bleaching, soda-containing or fluoridated toothpastes.
If these measures are followed and regular preventive visits to the dentist, the development of complications is reduced to a minimum. In addition, it is recommended to protect the row from excessive loads and injuries, and to exclude situations in which the prosthesis or jaw could be damaged.
Do you really have to put up with this?
Making dentures is quite a complex job, in some ways even comparable to art. Working in tandem, the orthopedic surgeon and the dental technician put a lot of effort into making an accurate and as comfortable prosthesis as possible. But in most cases, after putting it on and wearing it, it turns out that it needs some adjustment to the patient’s gums.
To regain lost comfort, you need to walk with the installed structure for 3–4 weeks. During this time, you can get used to the initially interfering prosthesis and get rid of the unpleasant sensations. If you simply remove it when discomfort appears, then you will have to describe all the inconveniences experienced in words, and the doctor will not be able to understand what exactly caused them. Do you want the correction to be effective? Be sure to come to your appointment wearing a prosthesis that causes discomfort.
Correction of dentures is carried out within 15–20 minutes. As a rule, it is possible to restore the patient’s comfort in one or two visits to the dental clinic.
Do I need to see a dentist?
If an inflammatory process occurs, then professional therapeutic treatment is necessary. To do this, the crown is removed without the possibility of reusing it. After sanitation, it is necessary to monitor the dynamics for some time, and it will be possible to resume orthopedic treatment only when the absence of inflammation is confirmed.
If you feel that the crowns are interfering with your bite, you do not need to fix the problem yourself. Seek help from a specialist as soon as possible. Without the intervention of a specialist, restoration of the bite is impossible. If the teeth meet in a certain place, and not evenly, then many problems can arise. Among them: increased tooth wear, gaps in teeth and other complications.
Important!
If for some reason your doctor does not want to redo his work, then you need to contact another specialist, but you should not delay the solution to this problem.
What is a dental crown
A crown is a type of dental prosthesis, non-removable, completely or partially covering the visible part of the tooth. Sometimes it is part of a larger prosthesis, such as a bridge. Crowns are distinguished:
- orthopedic. Replenish the missing part of the tooth crown. These include equatorial, three-quarter (for premolars), half-crowns (protect part of the vertical surface and the cutting edge);
- full clinical. Like a cap, they cover the entire stump of the tooth.
- stump, fenestrated, crowns with a pin are placed when more than 80% of tooth decay occurs, so they are often classified as pin structures.
To ensure that the crown does not interfere with the closure and active movement of the jaw, it is made according to the shape of the tooth, with a tight coverage of the neck without immersing more than 0.2 mm in the gum pocket. “Parts” for this type of fixed prosthetics are cast from metals, alloys, porcelain, and plastic. There are combined dentures, when a material different from the base is used for lining.
An inlay is first installed under the crown. Happens:
- straight (direct), made in the mouth, used when the tooth has 3 out of 4 walls left. Externally, it is a screw or pin that is inserted into the canal with a filling;
- indirect (indirect), an impression is made, and the inlay is cast from it in the laboratory.
The pin cult inlay is considered more reliable (and expensive); a ceramic inlay is placed under ceramic dentures.
Dental crown