What is tonsillectomy?
Removal of palatine tonsils is one of the most common operations in the practice of an ENT doctor.
Many people think that it is performed only for children, but this is not so. Adults may also need it if chronic tonsillitis has become severe and is accompanied by purulent complications, and enlarged tonsils interfere with swallowing and even breathing, causing sleep apnea syndrome - a short-term cessation of breathing during sleep. The palatine tonsils sometimes become inflamed. Inflammation of the tonsils (tonsils) is referred to as tonsillitis. It, in turn, can be acute and chronic.
Inflammation of the tonsils. Photo: James Heilman, MD / (Creative Commons Attribution-Share Alike 3.0 Unported license)
Acute tonsillitis is called tonsillitis. With chronic tonsillitis, the inflammatory process lasts for years, with periodic exacerbations. An exacerbation is usually accompanied by fever, sore throat and sore throat, including when swallowing.
The tonsils become coated, bad breath appears, and the cervical lymph nodes become enlarged. If exacerbations recur one after another, and conservative treatment does not help, you have to resort to surgical treatment - removal of the tonsils (tonsillectomy).
Relief of pain symptoms in children after tonsillotomy
One of the most common diseases of the ENT organs in childhood, diagnosed according to some data in more than 50% of preschool children [1], is hypertrophy of the palatine tonsils. The high prevalence of this condition in children is associated with a high frequency of surgical interventions on the tonsils, in our country this is mainly tonsillotomy. In Russia, tonsillotomy accounts for 25–30% of planned surgical interventions in a children's hospital [2]. According to foreign authors, the share of tonsillotomy (adenotonsillotomy) in those countries where this intervention is practiced in the structure of surgical interventions in otorhinolaryngological departments is more than 55% (for the age group of patients from 1 to 3 years). The main indication for tonsillotomy is obstructive sleep apnea syndrome [3].
Among the most common complications in the early postoperative period during tonsillotomy and other surgical interventions on the tonsils are bleeding and severe pain, which should not be underestimated in pediatric practice. Thus, according to recent studies, complications in the early postoperative period in patients after surgical interventions on the organs of the lymphopharyngeal ring in 48.1% were severe sore throat, and bleeding was noted only in 3.9% of cases. In 29.0% of patients, severe sore throat was the cause of severe dysphagia, and in 4.6% it was clinically manifested by dehydration [4]. In children under 6 years of age, pain in the throat in the early postoperative period is mainly accompanied by nausea and vomiting [5].
Thus, one of the pressing problems of all modern clinical medicine and otorhinolaryngology in particular is postoperative pain relief. When analyzing previously published materials, one cannot fail to note the particularly great importance of non-steroidal anti-inflammatory drugs in minimizing pain after surgery on the tonsils [6].
The drug lysine salt of ketoprofen, which has anti-inflammatory, analgesic and antipyretic properties, with a rapid onset and duration of action of up to 8 hours, combined with very good tolerability, is of certain interest in terms of pain relief [7]. According to comparative randomized clinical studies of ketoprofen, lysine salt in a dose of 50–100 mg has a stronger analgesic effect than paracetamol/codeine combinations [8].
Taking into account the above problem, a clinical study was conducted at the clinical sites of the Department of Pediatric Otorhinolaryngology of the Federal State Educational Institution of Further Professional Education of the Russian Medical Academy of Postgraduate Education, the purpose of which was to increase the effectiveness of pain relief after tonsillotomy in children.
The study included 140 children aged 6 to 18 years (mean age 9.49 years) after radiowave tonsillotomy under endotracheal anesthesia. As a premedication before surgery, patients received only atropine solution (sublingually). In all patients, tonsillotomy (in 121 patients in combination with adenotomy using the Kozlov-Karpov method) was performed using a radio wave surgery device. A direct incision through the tissue of the palatine tonsil was made using a monopolar needle electrode in the “cut and coagulation” mode. Non-steroidal anti-inflammatory drugs were prescribed to relieve pain in the early postoperative period. All children, according to the sequential number randomization method, were divided into four groups.
Patients of the 1st group (35 people) received the drug ketoprofen lysine salt in the form of an oral solution (OKI drug, produced by Dompe, Italy) 40 mg (children aged 6 to 14 years) or 80 mg (children over 14 years old) and older) if there are complaints of severe, unbearable sore throat with an interval between doses of the drug of at least 8 hours.
Patients of the 2nd group (35 people) received the drug ketoprofen lysine salt in the form of an oral solution (OKI drug, produced by Dompe, Italy) 40 mg (children aged 6 to 14 years) or 80 mg (children from 14 years old and older) 3 times a day (at least 8 hours between doses) for 3 days after surgery.
Patients of the 3rd group (35 people) received ibuprofen orally (Nurofen, syrup 100 mg/5 ml, manufactured by Reckitt Benckiser Healthcare International Ltd., UK) 100-300 mg (child weight 17-20 kg - 150 mg each ; child weight 21-30 kg - 200 mg; child weight 31-40 kg - 300 mg) up to 3 times a day if there are complaints of severe, unbearable sore throat.
Patients of the 4th group (35 people) received the drug ketoprofen lysine salt in the form of a solution for topical use (OKI drug, produced by Dompe, Italy) 4 ml (children aged 6 to 12 years) or 6 ml (children over 12 years old) and older) 2 times a day (morning and evening) for 3 days after surgery. A single dose of rinsing solution was diluted in 100 ml of drinking water immediately before use. The patient performed the first gargling with this solution 3 hours after surgery, regardless of the severity of the pain syndrome.
Control examinations of patients were carried out 3, 6 hours after surgery, on the 1st, 2nd and 3rd days after surgery.
The study did not include children with diseases and conditions that are a contraindication for the prescription of the drug ketoprofen lysine salt in the form of granules for the preparation of an oral solution (for patients of the main groups) and ibuprofen (for patients of the control group), as well as patients with concomitant diseases, changing, in the opinion of the researcher, the natural course of the disease, affecting the result of therapy and/or violating the possibility of subjective assessment of the symptoms of the disease (psychoneurological pathology, diabetes mellitus, blood diseases, oncological diseases, immunodeficiency states, infectious diseases, etc.).
The evaluation of the effectiveness of treatment was carried out by the curator personally, noting the patient’s condition at the agreed time, entering into the primary documentation (inpatient card) the frequency of vomiting, the presence of nausea and the presence of bleeding from the surgical field. If bleeding occurred in the early postoperative period, the doctor carried out a set of measures to achieve stable hemostasis. If a patient vomits more than 2 times and severe nausea, the patient was given a single intravenous injection of metoclopramide solution (based on the patient’s body weight); if vomiting occurs more than 3 times, infusion therapy with glucose-saline solutions was performed.
Starting from the first day after surgical treatment (3 hours after surgery), the patient independently subjectively assessed the severity of pain in the throat and nausea on the basis of a 10-point visual analogue scale, where “0” points were the absence of a symptom, “10” points - maximum severity of the symptom. Patients of the 1st and 2nd groups, when taking the drug ketoprofen lysine salt in the form of an oral solution for the first and second time, assessed the ability to swallow the medicine (they could or not) and the organoleptic properties of the drug (whether they liked the taste or not). Patients of the 4th group, during the first and second gargling with a solution of ketoprofen lysine salt, assessed the possibility of using this form of medication and the organoleptic properties of the drug (whether they liked the taste or not).
The assessment of the safety of therapy was carried out by assessing the patient’s condition in a timely manner, noting in the primary documentation (inpatient card) the corresponding changes in the patient’s condition (the appearance of pathological elements on the skin, diarrhea, nausea, shortness of breath, etc.). On the 2nd day after surgery, all patients underwent capillary blood sampling for a general clinical blood test.
Statistical processing of the results was carried out using the Statistica v.6.0 program. To compare quantitative characteristics, Student's t-test was used, and to compare qualitative characteristics, Pearson's c2 test was used. The difference was considered statistically significant at p < 0.05.
Results and discussion
According to the visual analogue scale (VAS), at the first examination after surgery, patients of all groups had the same severity of sore throat (p > 0.05). This indicator was 6.4 ± 0.3 points in patients of the 1st group, 6.8 ± 0.5 points in the 2nd group, 6.2 ± 0.4 points in the 3rd group, 4th groups - 6.5 ± 0.5 points. Nausea and vomiting were noted in the 1st group in 7 (20%) people, in the 2nd group - in 8 (22.9%), in the 3rd - in 6 (17.1%) and in the 4th group - in 8 (22.9%) people. There was no bleeding in any patient. In the 1st group, 17 (48.6%) patients asked for an anesthetic drug, in the 3rd group - 14 (40%) patients.
During the control examination 6 hours after surgery, the severity of sore throat was 4.2 ± 1.2 points in patients of the 1st group, 1.6 ± 0.8 points in the 2nd group, 1.6 ± 0.8 points in the 3rd group - 4.8 ± 1.4 points, in group 4 - 3.4 ± 1.2 points. There was no statistically significant difference in indicators (p > 0.05). At the second examination (6 hours after surgery), 9 patients of the 1st group and 13 patients of the 3rd group asked for an anesthetic drug. However, none of the patients in groups 2 and 4 asked the doctor for an anesthetic during the follow-up examination.
During a control examination 6 hours after surgery, complaints of nausea and vomiting were reported by 9 (25.7%) patients of group 1 (all did not receive painkillers after the first examination), 1 (2.9%) patient of group 2, 11 (31.4%) patients (8 of them did not receive pain medication at the initial examination) of the 3rd group and 4 (11.4%) patients of the 4th group. 2 out of 3 patients of the 3rd group, who continued to have nausea after taking ibuprofen syrup, noted that a feeling of nausea arose after taking the drug. None of the patients had bleeding.
When examining patients 24 hours after surgery, according to VAS data, the severity of sore throat in patients of the 1st group was 3.5 ± 0.8 points, in the 2nd group - 1.2 ± 0.4 points, in 3 in group 4.5 ± 0.8 points, in group 4 — 3.2 ± 0.6 points. The severity of pain in patients of group 2 was significantly less than in patients of groups 1, 3 and 4 (p < 0.05). The difference between VAS scores for the severity of sore throat between patients of groups 1, 3 and 4 was not statistically significant (p > 0.05). One day after the operation, 1 (2.9%) child from the 1st observation group and 2 (5.7%) patients from the 3rd group complained of nausea. None of the patients had bleeding.
When examining patients 48 hours after surgery, according to VAS data, the severity of sore throat in patients of group 1 was 2.7 ± 0.6 points, in group 2 - 0.8 ± 0.2 points, in group 3 in group 3.6 ± 0.5 points, in group 4 — 2.5 ± 0.6 points. The severity of pain in patients of group 2, as at the previous examination, was significantly less than in patients of groups 1, 3 and 4 (p < 0.05). The difference between VAS scores for the severity of sore throat between patients of groups 1, 3 and 4 was not statistically significant (p > 0.05). No child complained of nausea. None of the patients had bleeding. According to the results of a clinical blood test taken on the second day after surgery, no pathological changes were detected in any patient under our supervision.
When examining patients 72 hours after surgery, according to VAS data, the severity of sore throat in patients of group 1 was 1.4 ± 0.5 points, in group 2 - 0.4 ± 0.05 points, in group 3 in group 1.8 ± 0.5 points, in group 4 — 1.4 ± 0.4 points. The severity of pain in patients of group 2, as at the previous examination, was significantly less than that in patients of groups 1, 3 and 4 (p < 0.05). The difference between VAS scores for the severity of sore throat between patients of the 1st, 3rd and 4th groups is not statistically significant (p > 0.05). No child complained of nausea. None of the patients had signs of bleeding.
According to the results of a follow-up examination of patients 10 days after surgery, not a single patient had complaints of bleeding from the oropharynx. None of the patients complained of discomfort in the throat. A retrospective assessment by patients (or their official representatives) of the ease of use of the drug ketoprofen lysine salt in the form of granules for the preparation of an oral solution (patients of the 1st and 2nd groups) showed that all patients noted the ease of use of this dosage form and only 3 ( 8.6%) patient of the 1st group and 1 (2.9%) patient of the 2nd group described the taste of the drug as “unpleasant”. However, this did not affect the possibility of further use of the drug. A similar survey of patients of the 4th group who used gargling with a solution of ketoprofen lysine salt for pain relief showed that 28 patients (80%) found this form of use convenient, while the remaining 7 patients were also able to use this form of the drug as prescribed by the doctor. Moreover, all 7 patients who noted some inconvenience in using this form of the drug were under the age of 10 years. The organoleptic properties of the rinse solution were rated as “pleasant” by 30 (85.7%) patients.
conclusions
Based on the above, we can conclude that in patients who have undergone radio wave tonsillotomy, a course of ketoprofen lysine salt solution for oral administration in the early postoperative period has an advantage over a single use (in the presence of severe sore throat) of this form of the drug or ibuprofen syrup according to effectiveness in relieving pain in the throat. A course of oral administration of a solution of ketoprofen lysine salt can reduce the frequency of complaints of nausea on the first day of surgery.
The form of the drug solution of ketoprofen lysine salt for gargling with a course of use in the early postoperative period in this category of patients gives an effect in reducing sore throat, comparable to a single oral administration of painkillers used during observation, but is inferior to the analgesic effect of a course of use of a ketoprofen solution lysine salt for oral administration. Also, this form of the drug is not always convenient for use in children under 10 years of age.
None of the patients under observation showed signs of serious adverse drug reactions from the use of the above-mentioned drugs, requiring the patient to be excluded from the study and provided with appropriate medical care. Complaints of a number of patients about nausea and vomiting are probably related to the anesthesia treatment the child underwent, since they were noted in patients of the 1st and 3rd groups, regardless of the fact that an anesthetic was used. However, in some cases, nausea cannot be ruled out as a consequence of taking an anesthetic drug.
The results of our observation in comparison with the available literature data allow us to conclude that a course of use in the early postoperative period of a solution of ketoprofen lysine salt for oral administration in patients who have undergone radio wave tonsillotomy has an advantage over a one-time use (due to severe sore throat) of a similar drug, ibuprofen syrup and ketoprofen lysine salt solution for gargling. At the same time, the subjectivity of a number of criteria for assessing the effectiveness of these drugs determines the relevance of further study of the issue of the peculiarities of the use of non-steroidal anti-inflammatory drugs in the early postoperative period in children after surgical interventions on the organs of the lymphopharyngeal ring.
Literature
- Dashevskaya N. D. Health status of preschool children before entering school. Materials of the IX Congress of Pediatricians of Russia. 2001: 176–177.
- Karpova E. P., Tulupov D. A., Zyabkin I. V., Naumov O. G., Kerchev B. I. On the issue of indications for adenotomy in children // Russian Rhinology. 2010;3:48–49.
- Borgström A., Nerfeldt P., Friberg D., Sunnergren O., Stalfors J. Trends and changes in pediatric tonsil surgery in Sweden 1987–2013: a population-based cohort study // BMJ Open. 2017; 7(1):e013346. DOI: 10.1136/bmjopen-2016–013346.
- Muninnobpamasa T., Khamproh K., Moungthong G. Prevalence of tonsillectomy and adenoidectomy complication at Phramongkutklao Hospital // J Med Assoc Thai. 2012; Suppl 5:S69–74.
- Sidorov V. A., Agavelyan E. G., Mikhelson V. A., Leshkevich A. I., Grabovskaya V. A., Zyabkin I. V., Shcheglov A. O., Korotkova P. V. Modern approaches to conducting anesthesia in pediatric ENT surgery // Anesthesiology and Reanimatology. 2005; 1:4–9.
- Nosulya E.V., Kim I.A. Tonsillectomy: modern possibilities of postoperative pain relief // Medical Council. 2014; 15:36–40. DOI: https://dx.doi.org/10.21518/2079–701X-2014–15–36–41
- Borsa M., Tonon GC, Ronchi C., Zanolo G., Canali S. Pharmacokinetics of a slow-release preparation of ketoprofen lysine in man. // Arzneimittelforschung. 1983; 33(10):1497–1500.
- Messeri A., Busoni P., Noccioli B., Murolo S., Ivani G., Grossetti R., Gallini C., Maestri L., Fedele G., Novellini R. Analgesic efficacy and tolerability of ketoprofen lysine salt vs paracetamol in common pediatric surgery. A randomized, single-blind, parallel, multicentre trial // Paediatr Anaesth. 2003; 13(7):574–578.
E. P. Karpova, Doctor of Medical Sciences, Professor D. A. Tulupov1, Candidate of Medical Sciences V. A. Grabovskaya F. A. Fedotov
Federal State Budgetary Educational Institution of Further Professional Education RMANPO Ministry of Health of the Russian Federation, Moscow
1 Contact information
Relief of pain symptoms in children after tonsillotomy / E. P. Karpova, D. A. Tulupov, V. A. Grabovskaya, F. A. Fedotov
For citation: Attending physician No. 1/2018; Page numbers in the issue: 22-25
Tags: children, tonsils, postoperative period
Difference from tonsillotomy
Along with tonsillectomy, there is another operation with a similar name - tonsillotomy, in which enlarged tonsils are removed not entirely, but partially (usually in children). The indication for such an operation is the hypertrophy of these tonsils, when they occupy the entire space from the anterior palatine arch to the midline of the pharynx. With tonsillotomy, only the “excess” of enlarged tonsils is removed, returning them to normal size. Tonsillotomy is less traumatic than radical removal of the tonsils, and allows you to preserve their protective functions.
Why doesn't conservative treatment help?
Due to immunodeficiency (congenital or acquired) or concomitant diseases that contribute to prolonged inflammatory processes (diabetes mellitus, chronic infection), conservative treatment of tonsillitis may be ineffective.
Important! Group A beta-hemolytic streptococcus can settle in the tonsils, which causes rheumatic damage to the heart, joints and kidneys. Removing the tonsils avoids these complications.
Other factors that complicate conservative treatment include smoking and alcohol abuse. For teachers, singers and actors, the risk factor is the need to talk long, loudly and a lot.
Indications for laser tonsil removal
The reason for removing affected tonsils is the presence of a serious threat to other organs. As a rule, removal of the tonsils is indicated for patients who suffer from tonsillitis more than four times a year, patients for whom non-surgical treatment has not given the desired results, patients with complications such as diseases of the heart, joints, and nervous system. Removal of the tonsils is necessary for patients who have suffered an acute rheumatic attack, as well as for people whose excessive enlargement of the tonsils due to the spread of lymphoid tissue causes breathing or swallowing problems.
At what age is surgery performed?
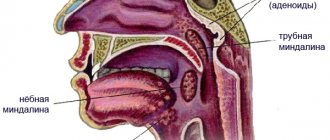
Surgical treatment may be recommended for adults and children over 8 years of age. By this time, the tonsils are fully formed. The palatine tonsils are an integral part of the pharyngeal ring - a group of tonsils (paired palatine and tubal, unpaired nasopharyngeal and lingual) - an important organ of local immunity of the nasopharynx and respiratory tract. Early removal of tonsils can contribute to the development of atopic diseases - allergic rhinitis or bronchial asthma. Such operations are usually not performed on children under three years of age, since they rarely have tonsillitis - the tonsils are too small.
Important! Tonsils can be removed no earlier than six months after polio vaccination.
Recovery period
The quality of the operation depends on the professionalism of the doctor. The laser is a sterile instrument that resists septic inflammation of tissues. Regeneration of the pharyngeal mucosa is restored within two to three weeks, in the absence of burns and extensive wounds. Typically, on the 7th day after laser tonsil removal, a postoperative examination is scheduled with the attending physician. To speed up healing, the patient is prescribed rinsing with a special composition. After tonsil removal, treatment with antibacterial drugs is usually not required. During the first 24 hours after laser treatment, the patient is allowed to drink only cool water. It is recommended to turn to a gentle diet of cool, smooth, soft dishes. It is not advisable to eat hard, spicy, fatty or hot foods. Smoking and drinking alcohol is strictly prohibited. After surgery, the patient should not freeze or be physically overloaded. It is advisable to undergo a course of immunity-strengthening treatment.
Contraindications
They can be absolute (excluding the possibility of tonsillectomy) and relative, when everything is postponed until the reasons preventing the operation are eliminated.
Absolute contraindications:
- diseases with increased bleeding: hemophilia, hemorrhagic diathesis, Werlhof's disease, agranulocytosis, leukemia;
- heart failure grade 2–3;
- acute infectious diseases and exacerbation of chronic ones;
- active form of tuberculosis;
- cirrhosis of the liver.
Relative contraindications:
- caries (before sanitation - dental prophylaxis of the oral cavity);
- inflammation of the gums;
- pustular diseases of the mouth and skin;
- ARVI and influenza;
- exacerbation (decompensation) of chronic diseases;
- menstruation;
- pregnancy after the 26th week due to the risk of premature birth.
Contraindications to laser intervention
Removal of tonsils with a laser is contraindicated for patients with cancer, diseases of the hematopoietic organs, blood clotting disorders, mental and nervous system disorders, and serious heart, liver and kidney diseases.
Manipulations to remove hypertrophied tonsils should be postponed during periods of exacerbation of acute infectious, viral and rheumatoid diseases, the active stage of tuberculosis, diabetes mellitus, hypertension and during female menstruation. In addition, tonsil removal is not performed on pregnant and lactating women and children under 10 years of age.
Types of tonsil removal surgeries
Classical
The surgeon installs a mouth retractor and separates the tonsil tissue along with the capsule from the surrounding tissues in a “blunt” way using a raspator. The bleeding is stopped, the vessels are cauterized with an electrocoagulator or laser. The whole process takes from 15 to 40 minutes.
Electrocoagulation
Figure 1. Incision at the base of the tonsil during electrocoagulation.
Source: Maxillofacial Plastic and Reconstructive Surgery / Open-i (Attribution 4.0 International) Instead of a scalpel, a high-frequency current electrode is used. The vessels are “sealed”, so blood loss is minimal. Recovery may take longer due to associated injuries to surrounding tissues.
Removed tonsils. Maxillofacial Plastic and Reconstructive Surgery / Open-i (Attribution 4.0 International)
Cryodestruction
Tonsils are frozen with liquid nitrogen. As a result, they become pale, flat and hard, and after a day they die and are gradually rejected. The method is recommended for patients with an increased risk of bleeding (thrombocytopenic purpura, hemophilia, etc.), severe heart failure and endocrine pathology.
Important! The cryosurgical method is used in a series of procedures lasting up to 1.5 months. During this time, a relapse of the disease is possible if not all of the tonsil tissue has been destroyed. Cryosurgery is used when classical surgery is not possible.
Ultrasonic destruction
High-frequency sound vibrations warm up the tissues to prevent bleeding. Unlike exposure to liquid nitrogen or electricity, surrounding tissue is almost not damaged. Ultrasound method is one of the least traumatic.
Radio wave destruction
A probe is installed inside the tonsils, which generates radio waves. They evaporate the water from here and cause scarring. Ablation can be repeated several times. Anesthesia is not needed here - only local anesthesia or light sedation. Recovery is quick, but radical tonsil removal is almost impossible. Therefore, radio wave therapy is used for their hypertrophy, but not for chronic tonsillitis, when radical intervention is required.
Cold plasma destruction
A relatively new method of removing tonsils. It is based on the property of cold plasma (radio frequency energy converted into ionic dissociation) to separate molecular bonds in tissues without releasing thermal energy. Plasma is called cold because it causes minimal heating of the tissue, which means that pain after surgery will be insignificant, recovery will be easy and quick. The method is low-traumatic and can be used for partial or complete removal of tonsils.
Laser removal
Laser tonsillectomy can be complete or partial (with cutting of the upper layers of the tonsils). Different types of laser are used - carbon, infrared, etc. Only pathological tissues are removed, and healthy ones are not affected. Other advantages include immediate separation of the tonsil from the underlying tissues with coagulation of blood vessels, which reduces the risk of bleeding and infection.
Operation options
Most often, a bilateral tonsillectomy is performed, that is, complete bilateral removal of the tonsils. How is tonsil removal done? There are several variations in how the operation is performed.
The classic type of operation is mechanical removal using a scalpel, a special loop and surgical scissors. This is a radical way to get rid of chronic tonsillitis. Recovery after surgery is long and quite painful. Another disadvantage of this operation is the high likelihood of bleeding.
Currently, classical surgery is being replaced by microinvasive tonsillectomy, which is much easier to tolerate by patients, avoids heavy blood loss and makes it easier to recover from surgery. There are several modern methods for removing tonsils.
- Laser tonsillectomy. How is laser tonsillectomy performed? Under the influence of laser radiation on the lymphoid tissue of the tonsil, liquid evaporates from it, and the vessels are coagulated (cauterized), which avoids bleeding. The patient does not experience pain. The wound at the site of the removed tonsil heals quickly enough, so the patient’s recovery is quick and easy. The downside of this operation is the heating of healthy tissue, which can lead to burns.
- Radio wave method. How is tonsillectomy performed using the radio wave method? Under the influence of a radio wave created by the Surgitron or Fotek surgical apparatus, the liquid from the tonsil tissue is evaporated. The operation is bloodless and does not damage healthy tissue. Swelling after surgery disappears quickly enough, and the patient recovers easily.
- Ultrasonic removal is carried out using an ultrasonic scalpel, which heats and destroys the affected tissue. This is a low-traumatic, safe method of removal. Thanks to the effects of ultrasound, tissue regeneration proceeds faster.
- Cryodestruction. During this procedure, the tonsils are exposed to low temperature, the source of which is liquid nitrogen. After this, the inflamed tissue is rejected. This is the most non-traumatic, bloodless method of removal. It does not require special postoperative care, is carried out quickly and is very easily tolerated by patients.
- Coblation is the effect of cold plasma on the tonsils. The operation is performed using a special device that converts electricity into plasma. The plasma flow does not burn healthy tissue. The recovery period after coblation is the shortest and most painless of all removal methods. The disadvantage of the operation is its price and low prevalence. Few medical institutions offer this service.
When deciding on an operation, the ENT doctor will definitely explain all the pros and cons of each type of surgical intervention and give recommendations on what is best to choose in a particular case.
Many patients before tonsillectomy ask the question: “What is the danger of removing tonsils?” Possible complications after surgery include the likelihood of relapse if tonsil tissue is not completely removed; the likelihood of bleeding in the first hours after surgery and infection of the wound (more often in patients with weak immunity).
Postoperative period
Figure 2. Appearance of the throat after tonsillectomy. Source: James Heilman MD, CC BY-SA 3.0.
Recovery usually takes 3–4 weeks, the first of which takes place in the hospital. This is necessary in order to respond in time to the most common complication of tonsillectomy – pharyngeal bleeding. To prevent it, hemostatic drugs are prescribed.
From the operating room the patient is transferred to a ward under the supervision of the attending physician. On the first day, it is forbidden to swallow, spit or expectorate saliva. You can only breathe through your mouth. In case of severe pain, the patient is prescribed painkillers.
A diet is recommended for all days of the postoperative period
- on the first day, adults should refrain from eating, and small children should not eat or drink for the next 6 hours;
- In the first week after surgery, it is recommended to eat liquid, smooth food;
- During the recovery period, food should be soft; it is not recommended to eat too hot, cold, sour, or spicy. This may irritate the mucous membranes of the throat and mouth.
- In the postoperative period, if necessary, a course of antibiotics is prescribed.
Figure 3. Memo: what you can and cannot eat after surgery.
Source: verywellhealth.com Bed rest must be observed for 2 days. In most cases, the patient is discharged from the hospital within a week for outpatient observation and treatment.
Material and methods
The study was carried out in patients with chronic decompensated tonsillitis who were admitted to the Department of Otorhinolaryngology of the St. Petersburg State Medical University named after. acad. I.P. Pavlova for planned surgical treatment. Group 1 included 23 patients aged from 20 to 43 years, who in the postoperative period received NSAIDs (Ketorolac) on demand for pain, as well as a homeopathic monocomponent herbal preparation Arnica Montana C9 (BOIRON) 5 granules 3 times a day for resorption from the 2nd day. The second (control) group of patients included 20 patients aged 19 to 42 years who received only on-demand NSAID therapy (Fig. 1).
Rice. 1. Distribution of patients in groups by age. The two study groups of patients were balanced by gender and age, thus, the studied differences between them reflect the effect of the drug Arnica Montana C9 (BOIRON). All patients underwent classical bilateral tonsillectomy under general anesthesia by the same operating team. In the early postoperative period, a number of criteria were assessed in all patients: body temperature in the morning after waking up and in the evening, the need to use NSAIDs, the amount of their use per day, pain assessment according to VAS, as well as changes in the pharyngoscopic picture and neck lymphadenopathy within 10 days after surgery.
The results of the study were entered into the developed computer database on a personal computer using Microsoft Excel tables. Using the application package Statistica for Windows v.10.0, analysis and statistical processing of the obtained data were carried out, and the parameters of descriptive statistics were determined.
Quantitative indicators were checked for compliance with normal distribution using the Kolmogorov-Smirnov test. For quantitative data having a normal distribution, the arithmetic mean ( M
) and standard deviation (
SD
), which are presented in the format
M
(
SD
); when describing indicators that differ from the normal distribution, medians (Me) were used in the Me format (Q1; Q3) and the lower Q1 (25%) and upper Q3 (75%) quartiles were used as an interval estimate. Qualitative indicators of the study are presented in absolute and relative values (%).
To find differences between normally distributed indicators, t
-Student's t-test.
Formula t
-Student's test:
where M
1 - arithmetic mean of the 1st compared group,
M
2 - arithmetic mean of the 2nd compared group,
m
1 - mean error of the first arithmetic mean,
m2
- mean error of the second arithmetic mean.
Statistical processing of the study results in groups was carried out with determination of significance using the nonparametric Mann-Whitney U test.
Mann-Whitney U test formula:
where n
1 - the number of elements in the 1st sample,
n
2 - the number of elements in the 2nd sample, T
x
- the larger of the 2 rank sums,
nx
- the corresponding sample.
Indicators changing over time were analyzed using paired Student's t test (in the case of normal distribution) or using t
-Wilcoxon test.
To analyze qualitative indicators, the χ2 test with Yates' correction was used (in cases of absolute numbers less than 10); if it was impossible to use it, the Z-test was used for proportions with correction for end points.
The difference between groups was considered statistically significant at p
<0,05.
Complications after removal of tonsils
The most common of them is bleeding, which can develop both on the first day after the intervention (primary bleeding, and 5-6 days after it. The incidence of postoperative pharyngeal bleeding ranges, according to various observations, from up to almost 60%. Minor bleeding after removal of the tonsils is stopped using a tampon, electrocoagulation, or the anterior and posterior palatine arches are sutured together to reduce the area of bleeding.
Also, as a side effect of the procedure, there is a risk of blood aspiration (blood entering the respiratory tract). Then the blood is urgently removed with an electric suction and bronchoscopy is performed.
After removal of the tonsils, swelling of the soft palate and larynx is possible. If signs of difficulty breathing appear, decongestant therapy is carried out.
If the wound becomes inflamed after removal of the tonsils, antibiotic therapy is prescribed.
In most cases, the operation takes place without complications or side effects. If the patient experiences pain, the doctor will prescribe analgesics on the first day after removal of the tonsils, and then non-steroidal anti-inflammatory drugs.
Sometimes the patient may experience voice changes, taste disturbances, and nasal sounds.
It is extremely rare to experience damage to the temporomandibular joint due to forceful opening of the mouth with a mouth opener during tonsil removal.
Complications
Complications after tonsillectomy can be associated directly with mechanical effects (bleeding) and with the addition of infection.
Bleeding may occur during or immediately after surgery, or several days after surgery. According to various sources, this complication occurs in 2-10% of cases. In the early period, bleeding develops due to incorrectly chosen surgical tactics, concomitant diseases of the patient, and incorrect preparation for surgery. Secondary bleeding occurs during the rehabilitation period, when films and scabs begin to come off, most often due to active interference in this process. To avoid complications, careful preoperative preparation is necessary, compliance with all doctor’s recommendations - abolition of blood thinners before the procedure, a period of rest after surgery.
As a result of bacterial complications, in the first 5-7 days after tonsillectomy, the patient may develop purulent foci at the site of intervention, bronchitis, pneumonia, pleurisy, and lung abscess. Failure to maintain sterility during surgery carries the risk of developing septicemia - generalized damage to the body as a result of bacteria entering the blood. An important measure to prevent this complication is compliance with the rules of asepsis and antisepsis during surgery, medical supervision of the patient in the first few hours after the intervention, and following the doctor’s recommendations during the recovery period.
Sources
1. Palchun V.T.
Otorhinolaryngology: national guidelines. M.: GEOTAR-Media, 2016. 2. Karpishchenko S.A., Svistushkin S.M. Chronic tonsillitis and tonsillitis. Immunological and clinical aspects. St. Petersburg: Dialogue, 2017.
3. Lukan N.V., Sambulov V.I., Filatova E.V. Conservative treatment of various forms of chronic tonsillitis. Almanac of Clinical Medicine, 2010, 23: 37-41.
4. Belov, B.S., Shcherbakova M.Yu. A-streptococcal tonsillitis: modern aspects. Pediatrics. 2009, 88(5): 127-135.
5. Turovsky A.B, Kolbanova I.G. Chronic tonsillitis - modern concepts. Doctor.RU, 2009, 49(5): 16-21.
Testing to confirm the need for tonsillectomy
This diagnosis of “decompensated form of chronic tonsillitis” is established on the basis of a set of data, including the history of the disease, clinical picture, laboratory data (biochemical blood test with determination of antistreptolysin-O, rheumatoid factor, C-reactive protein, study of the immunological function of the palatine tonsils), and also the presence of complications: rheumatism, infectious nonspecific polyarthritis, diseases of the heart, kidneys, thyroid gland, purulent complications (peritonsillar abscess), information about the ineffectiveness of previous conservative treatment.
Study of the functional state of the palatine tonsils