Author of the article: Goldstein Maria Anatolyevna
Doctor-expert
Specialization: Dentist-therapist
Total work experience: since 2008
Reading time: 7-8 minutes
- Direct restoration
If the aesthetic properties of teeth are lost, a person experiences certain discomfort. The quality of life deteriorates if uneven or unsightly teeth prevent you from smiling broadly or if the enamel is too yellow, chips and cracks lead to complexes. Modern dentistry allows us to solve these problems by offering various types and methods of restoration, which is an alternative to full prosthetics.
What you need to know about dental restoration?
If restoration of the anatomical shape of teeth, their aesthetic properties and almost full functionality is required, then a number of procedures will be required to achieve the desired effect. Dental restoration is a set of dental measures to restore and correct shape and color. The materials used make it possible to imitate natural fabrics as accurately as possible, guaranteeing the aesthetics of the result.
Formally, restoration is essentially similar to filling, for example, some of the materials used and a number of stages. At the same time, it is impossible to compare the results, since aesthetic restoration manipulations guarantee a flawless smile.
Advantages
The advantages of artistic dental restoration are:
- Relatively quickly obtaining the desired result
. The restored tooth is visually no different from the rest in the row. The emphasis of the procedure is on maximum aesthetics. - Durability
. The materials and work performed are guaranteed for up to 10-15 years. - Durability
. As a result of restoration, the functionality of the tooth is restored - it is as strong as the rest. After the procedure, there is no need to make adjustments or additionally visit the dentist. - Easy to care for
. It is enough to follow the rules of basic oral hygiene and not to use abrasive pastes and hard brushes. - Resistance to aggressive environments
. The materials used for restoration are highly resistant to most food dyes. They are less resistant only to the effects of tobacco smoke (during active smoking) and red wine.
In addition, the advantages include a minimized risk of recurrence of caries and other diseases that led to partial destruction of the tooth and the need for its restoration.
Disadvantages and nuances
It makes sense to talk about the disadvantages, which are more nuances and features. These include:
- The need for careful treatment.
No matter how durable the result of the restoration is, there is still a risk that the restored part may break. To avoid this, you need to be careful with your teeth and not chew hard objects (for example, nuts, crackers, nails, wire, thread, etc.). - Chewing function not fully restored
. Artistic restoration of teeth is a procedure that is aimed at restoring aesthetic properties. Chewing function, however, is not fully restored. Please note that in some cases, instead of restoration, it is better to use the service of full prosthetics. - Relatively high cost of the procedure
. This nuance is natural in comparison with filling. Restoration requires extensive experience from the doctor and competent selection of materials (including color).
It is worth noting one more nuance - when restoring using the indirect method, you will not get the result after the first visit to the dentist. In addition, there is a need for regular visits to the doctor for fitting and adjustment of dental structures.
You might be interested in:
Dental restoration
Dental treatment
Veneers
Restoration of anterior teeth in Moscow at the PROFI-Dent clinic
Our dental center uses only the most modern restoration methods and technologies, which allow you to quickly and efficiently restore the anatomical, aesthetic and functional components of the front teeth, ensuring an impeccable appearance and a beautiful, natural smile.
The main advantages of aesthetic restoration with us:
- the opportunity to restore a gorgeous smile in just one visit to the dentist;
- latest generation materials;
- long-term result;
- the most affordable prices for front tooth restoration in Moscow.
We can correct your front teeth, change their shape, length, position, and eliminate enamel defects quickly and efficiently. To be confident in the final result, our specialists carefully monitor every stage of work, following the highest international quality standards, and use only advanced materials and restoration technologies.
Types and stages of dental restoration
Today, dental clinics are ready to offer two methods of dental restoration, these are:
- Straight
. To achieve the desired result, self-curing filling materials (photopolymers) are used. This type of restoration is called aesthetic. The work is carried out by a dentist-therapist. - Indirect
. At its core, the method is similar to prosthetics, since veneers are used to achieve the result. The work is carried out by an orthopedic dentist.
Restoration is an individual approach for each individual case. Therefore, the choice of the optimally suitable method can only be made by a dental specialist.
Direct restoration
This procedure is indicated for damage to the front teeth and is carried out in six main stages:
- Preparation
. Consists of the following mandatory dental activities:- hygienic teeth cleaning (polishing paste and nylon brushes are used for these purposes);
- choosing the color of the filling material (the doctor uses a special color scale so that the tooth being restored is no different from the rest in the row);
- anesthesia (anesthesia is administered to relieve possible discomfort during the procedure).
- Preparation
. For example, it may be necessary to drill out caries or simply bring a damaged tooth into a form convenient for further restoration. At this stage, modern specialists use the most gentle technologies to preserve as much healthy tissue as possible. - Insulation from moisture
. Photopolymers used for restoration deteriorate their properties when in contact with saliva or wet breath. That is why it is very important to prevent their contact, for example, by using a rubber dam. - Fixing the pins
. This stage is carried out if there is a need to fix the pins in the tooth canals. If there is no such need, the specialist proceeds immediately to the fifth stage. - Rough modeling
. Using layer-by-layer application of photopolymers, primary (rough) modeling is carried out - the size, shape and relief are reproduced. - Final modeling
. This is the stage where the final restoration work is carried out using grinding and polishing.
This type of restoration is also called composite. As a result of a correctly performed procedure, the restored tooth is identical to its neighboring natural counterparts in shape and color (if the dentist takes into account all anatomical features) and the patient does not feel any discomfort or the presence of anything foreign in the mouth when closing the jaw and touching it with the tongue.
Indirect restoration
The procedure involves covering the entire front part of the tooth with a veneer. In this case, the veneer cannot be considered a crown, since it only covers 1-2 sides and not completely. Using this technique, you can achieve an even more aesthetic result than using photopolymer fillings.
Indirect restoration is carried out in five main stages:
- Definition of color
. This is necessary so that the veneer does not visually differ from the rest of the teeth in the row. Since ceramics is used as a material, at the manufacturing stage it can be given any shade and it is very important, at the first stage, to determine which one. - Preparation (turning)
. Only the front part is subject to grinding, where the veneer will be installed. As a rule, the enamel is ground down to a thickness of 0.5-1.5 mm (depending on the thickness of the lining) so that the veneer does not stand out and is flush with the rest of the dentition. - Taking impressions.
This requires that the overlays be made taking into account all individual anatomical features. - Installation of temporary protection
. To protect prepared and ground teeth from the negative effects of aggressive environments in the oral cavity, temporary veneers are installed for the patient. They will remain there until the permanent ones are ready. - Installation of permanent veneers
. Veneers made from impressions are installed with a special glue.
It is worth noting that indirect restoration has a number of contraindications, for example, this restoration method is not recommended for those who have a habit of biting their nails, opening bottles with their teeth, etc.
In what cases is the dental restoration procedure used?
The procedure allows you to solve the following problems:
- carious damage to most of the frontal tooth surface;
- gaps between teeth;
- chips and damage to enamel;
- more than 50% destroyed crown;
- changes in enamel shade.
Aesthetic restoration provides an opportunity to correct the shape and color of teeth. After the procedure, they look natural and match the appearance and function of healthy teeth.
The cost of such a procedure depends on the nature of the defect and the methods used to eliminate it. This issue can be discussed at a clinic appointment.
Indications for the procedure
The main indications for restoration include the following:
- Correction of aesthetic defects. It is an improvement in the appearance of teeth damaged by caries or having defects in hard tissues. As part of this, dentists offer: Correction of enamel color. Moreover, restoration allows you to even out the color of not only a living tooth (using veneers on the vestibular surface), but also a dead tooth (using an indirect restoration method with the production of composite veneers or crowns).
- Correction of tooth shape and size. The main advantage of modern dentistry in solving this problem is the ability to obtain results in one visit to the clinic, especially if the issue concerns a minor diastema or other purely aesthetic defects. If the case is complex or advanced, experts offer alternative correction methods, for example, using inlays or crowns.
- Correction of the position of the tooth(s) in the row. The use of composite materials can provide immediate results when a single “movement” of individual teeth is required. If the problem is not purely aesthetic, then planned orthodontic treatment will be required.
In general, aesthetic restoration of teeth is an opportunity to correct minor cracks and chips, even out unsatisfactory enamel color, correct slight curvatures of the dentition (arising, for example, as a result of periodontitis), and get rid of the consequences of interdental, cervical and deep caries.
Restoration of chewing teeth
To restore chewing teeth, recreate their shape and the strength of hard tissues, composite materials and special inlays are used that replace the missing parts of the enamel.
Expert of the article you are reading:
Bystrov Alexey Albertovich
Dentist orthodontist, general dentist
You may also be interested in:
Ceramic veneers Lumineers price for 1 tooth in Moscow Ceramic veneers E-max
Show more
Contraindications
Aesthetic dental restoration is not only an excellent result and an excellent alternative to prosthetics, but also a restoration technique that is not suitable for everyone. Like most other dental procedures, restoration has absolute and relative contraindications.
Absolute contraindications include the following:
- The patient has a pacemaker installed
. The use of a device such as a photopolymerizer for composite restoration can cause a disturbance in the pulse frequency of the pacemaker. This is a huge risk to the health and life of the patient, as it can lead to cardiac arrest. - Allergy to composite materials
. It is extremely rare, but if the patient has an allergic reaction to adhesive systems or photopolymer materials, then it is worth choosing other methods of solving aesthetic problems rather than restoration. - Inability to isolate the tooth from moisture
. Some patients experience a psychosomatic reaction that does not allow the installation of a dental dam in the oral cavity. In these cases, restoration with composite materials with a quality guarantee is simply impossible.
So far, no other absolute contraindications to restoration have been found. This means that if you do not have the listed points, it is worth studying the relative contraindications in order to understand whether this recovery method is suitable for you or not.
Relative contraindications include:
- Teeth wear due to incorrect (straight) bite
. In this case, restoration should be postponed until the occlusion correction is completed. - Bruxism
. Strong compression of the jaws can cause premature destruction of the composite materials used in restoration. Therefore, in case of involuntary teeth grinding, it is recommended to use not restoration, but more reliable restoration methods, for example, installing crowns or other orthopedic structures. - No chewing teeth
. If they are absent in the lateral parts of the oral cavity, restoration of the anterior teeth is contraindicated. The fact is that in this case, the entire chewing load will be redistributed to the front teeth, which will lead to premature wear and destruction of the restored parts. - Significant destruction of hard tissue
. If, at the time of contacting the dentist, the tooth is destroyed by a third or more, the restoration cannot guarantee the reliability of the structure. In this case, it is worth using alternative methods to solve the problem.
In addition, restoration by direct and indirect methods is contraindicated for those patients who do not observe regular and mandatory oral hygiene. For such people, it is better to get metal or ceramic crowns rather than using composite fillings.
How much does it cost to restore front teeth?
Our clinic values its patients, so we carefully plan our pricing policy. You will be pleasantly surprised not only by the highest quality of dental services. The price of restoration of anterior teeth in PROFI-Dent dentistry is in the budget range.
| Price list for dental | |
| Consultation with a dentist-therapist | FOR FREE |
| Restoration of wedge-shaped defect, enamel erosion | from 3,000 rubles |
| Restoration of the frontal group | from 5,000 rubles |
| Artistic restoration made from light-curing material | from 5,000 rubles |
| Ceramic-composite veneer | from 8,000 rubles |
| Installation of dental jewelry | 1,000 rubles |
Read also
Why do teeth crumble?
Tooth decay in general, and crumbling in particular, is not an aesthetic problem.
How to restore and strengthen tooth enamel
Enamel is the outer shell of the tooth, which bears the heaviest load (chewing). She is the first to take on the “blows” of active substances contained in food and drinks.
When is direct restoration needed and when is indirect restoration needed?
Direct restoration is indicated for minor damage to the hard tissues of the tooth. Such as:
- caries;
- damage to the proximal surface;
- the presence of cracks and chips within the enamel layer.
Indirect restoration is indicated for:
- restoration of 50% or more of damaged tooth tissue;
- malocclusion due to pathological abrasion;
- orthopedic rehabilitation after orthodontic correction;
- increased patient requirements for aesthetics;
- if desired, obtain a long-term predictable result.
Materials:
For direct restoration, doctors at a modern clinic use a light-curing composite from the group of nanohybrids.
For indirect, all-ceramic blocks and all-zirconium discs and blocks are used.
It is very important that the center, the Moscow clinic where the patient goes, works with proven manufacturers of high-quality dental material.
Requirements for materials for dental restoration
Both aesthetic and artistic restoration of teeth cannot be performed with any filling material. Despite the fact that there are a lot of them and they are all high-tech.
Important properties of filling material:
- best adaptation to dental tissues;
- long working hours. The dentist must have enough time for artistic modeling and restoration of teeth;
- high strength and durability;
- low percentage of shrinkage, absence of it. Do not shrink much during photopolymerization;
- have fluorescent properties. Match as closely as possible the degree of fluorescence of the tissues of your own teeth. Otherwise, in neon light, instead of beautiful restorations and fillings, we will get black spots.
Research results
The patient, 46 years old, complained of an aesthetic defect in her anterior teeth (Fig. 1). Objectively: in the 11th and 21st teeth, extensive partial restorations with signs of secondary caries and a violation of the marginal seal are determined. The central incisal line is shifted to the left. Pathological abrasion along the cutting edge. Color 21 slightly changed. According to the patient, the tooth darkened after primary endodontics many years ago. After repeated endodontics, the color did not change. The tooth doesn't bother me. The radiograph shows obturation of the canal to the apex, the periodontal fissure is not widened.
Rice. 1. Defects in the fillings of the 11th and 21st teeth.
In accordance with the clinical picture, a diagnosis was made: secondary caries of the 11th and 21st teeth. The patient was informed about alternative methods of orthopedic and therapeutic restorative treatment of anterior teeth. She chose the method of complete direct restoration of 11 and 21, which is consistent with the opinion of the dentist. This choice is justified by the following factors:
- a large volume of lost tooth tissue dictates the need to correct the crown height and color, which excludes partial restoration;
- the relative cheapness of the method, treatment in one visit is attractive for the patient, in contrast to prosthetics or indirect restoration;
- slight color change 21, time and economic factors excluded intracanal bleaching 21.
The patient signed a preliminary consent to perform the necessary manipulations. Teeth were cleaned of plaque mechanically using a product that did not contain fluoride and oil. For this purpose, Clint paste (VOCO) was applied to a special brush rotating at low speeds. To avoid heating the tooth, an excessive amount of paste was used. Then the tooth was thoroughly washed with a stream of water.
Next, the size, shape, and relief were planned, which is a strictly defined sequence of actions, including odontometry and odontoscopy of the central incisors. Based on visual assessment and measurement results, a rectangular crown shape was planned: the side surfaces are located almost parallel; the horizontal dimensions in the middle and lower thirds are close in value.
Evaluation of signs of teeth belonging to the side showed a predominance in size of the distal angle of the crown. The sign of crown curvature is not expressed. The description of the individual characteristics of the tooth consisted of assessing the type of macrorelief of the vestibular surface.
The selection of the desired shades of the Admira Fusion (VOCO) photocurable composite was carried out in natural light using special standards by comparing them with the intact lateral incisor before installing the rubber dam. The color of the composite was specified by applying a “drop” of the composite to the vestibular surface of the incisor directly from a syringe (Fig. 2, 3). The following syringes were selected: cervical region - A3.5, body - A2, transparent enamel - Incisal. The material allows intuitive selection of shades and makes it possible to create colors using both opaque and enamel shades.
Rice. 2. Selection of enamel shades of the composite.
Rice. 3. Selection of dentin shades.
Considering the slight difference in the color of the 11th and 21st teeth, it was decided to carry out a correction using enamel shades of the material. Thus, for the cervical area of the 21st tooth, a syringe GA3.25 was chosen (the original shade between A3 and A3.5 on the Vita scale), and shade A1 was used for the body of the veneer.
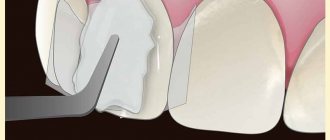
The preparation was performed with medium-grain diamond burs and began with the removal of low-quality fillings, protruding enamel edges, and dentin necrotomy (Fig. 4). The contours of the veneer coating were marked using a small spherical bur in the form of grooves no more than 0.5 mm deep.
Rice. 4. A set of burs for preparing a tooth “for veneer”.
In the proximal areas, to hide the edge of the veneer, the boundaries extended to the contact surfaces. The cervical border of the veneer is located along the border with the gum to avoid the transmission of pigmented tooth tissues. Cervical ledges are formed, internal angles are smoothed. The vestibular surface of the incisors was processed with a fine-grained cylindrical bur (Fig. 5, 6).
Rice. 5. Marked bur in sterile packaging.
Rice. 6. A diamond bur is placed in the turbine tip.
A rubber dam was installed with exposed teeth 14 to 24, which will allow you to focus on the dentition when creating the shape and distributing color areas. The quality control of preparations 11 and 21 was carried out (Fig. 7). Next, the technique of total etching of the prepared surfaces of the central incisors was carried out (Fig. 8).
Rice. 7. The central incisors were prepared.
Rice. 8. Total acid etching.
The gel used was Vococid (VOCO) - 35% phosphoric acid. The gel was washed off with a stream of water, and the teeth were dried with a reflected stream of air. Adhesive preparation was carried out with a universal bond, suitable for any adhesive technique (Fig. 9). A thin layer of Futurabond was applied to the etched surface of the teeth with a brush and cured with the light of a halogen lamp (Fig. 10). Next, the veneers were modeled using the following Grandio dentin shades for the 11th tooth: cervical area - color OA3.5, body - OA2 (Fig. 11).
Rice. 9. Futurabond U adhesive system.
Rice. 10. Adhesive preparation of the 11th tooth.
Rice. 11. Photo-curable material.
The production of a classic veneer began with the application of an opaque composite to the prepared surfaces. A restoration base is created that includes a dentin geometric outline to define the lateral and inferior boundaries of the veneer. The sign of the crown angle is modeled. The first layer of Grandio opaque filling material was placed on the mid-gingival area and moved towards the neck of the tooth. The next layer was placed on top of the previous one and distributed evenly over the entire area. The lateral surfaces of the veneer were not brought into contact with adjacent teeth by 1.0 mm, which is due to the type of transparency of the enamel in this area (Fig. 12).
Rice. 12. Opaque layers of the composite are applied.
In accordance with the instructions for using the composite material, the latter was added in layers no more than 2 mm thick, compacted to the tooth tissue and cured with halogen light. The prepared opaque base, which replenishes the shape and volume of the tooth dentin, was covered with enamel shades of the material. To form a periodontal contour, a portion of enamel composite was applied to the central gingival area of the tooth and smoothed from the center to the periphery.
When modeling the enamel layer, shades A3.5 and A2 were used, respectively. Space is left for the transparent Incisal shade in the area of the incisal edge and side edges (Fig. 13). The formation of contact surfaces was completed by applying a transparent composite, which was distributed taking into account the individual degree of transparency of the enamel. The same transparent material was used to model the cutting edge and cover the corners of the veneer.
Rice. 13. Modeling the enamel layer.
For the restoration of the 21st tooth, dentin colors were chosen similarly to veneer 11. Syringes of the enamel composite are presented in shades GA3.25, A1, Incisal (Fig. 14). Dentin shades for the formation of a veneer on the 21st tooth were applied in layers up to 2 mm thick, which ultimately filled the volume of missing dentin without involving the boundaries of the enamel layer (Fig. 15). Using individual tint enamel syringes, the effect of neutralizing color accents was achieved (Fig. 16). The surface of the restoration was covered with a transparent layer in accordance with the type of enamel transparency.
Rice. 14. Tint composite syringe.
Rice. 15. Opaque layer of the 21st tooth.
Rice. 16. Color neutralization has been completed.
Immediately after the aesthetic structure is manufactured, it is processed: the surface hybrid layer is removed and the relief is enhanced. Contouring and polishing of the vestibular surface of the veneer was carried out using Dimanto diamond instruments (VOCO) (Fig. 17). After removing the rubber dam, adaptation to the bite, grinding, and polishing are controlled (Fig. 18).
Rice. 17. Polishing system.
Rice. 18. Ready-made aesthetic restorations.
The final stage of treatment is coating the enamel surrounding the restoration with fluoride-containing varnish Bifluorid 12 (Fig. 19). Long-term quality control of the work performed shows the high efficiency of using the method of producing direct veneers from a photocurable composite.
Rice. 19. Fluoride varnish.