How can you get infected with herpes
The content of the article
The disease is caused by the herpes simplex virus (HSV, Herpes simplex virus). Of the eight types of this pathogen, genital lesions are the result of two infectious agents. HSV-2 causes 80% of cases of the disease, and HSV-1 - 20%. There are also combined infections, in which both viral types are to blame.
There is a misconception that herpes on the lips and genitals are completely different diseases. In fact, both types of pathogens often “swap places” during domestic infection and oral sex. And both infections are equally dangerous.
Both types of virus are transmitted:
- For all types of sexual contact - vaginal, oral, anal, during which the virus enters the body through microdamage to the mucous membrane. You can also become infected from a partner who does not have rashes on the genitals or other manifestations of the disease. This condition is possible with strong immunity, when the virus lies low and waits in the wings. A person becomes a carrier of a herpes infection, but does not experience any health problems.
- Through common objects - washcloths, sponges, bed linen, towels. A person with a cold sore caused by the type 1 virus can become a source of genital herpes infection.
- During autoinoculation (self-infection), when the patient transfers the pathogen from the face to the genitals.
- A child becomes infected from a sick mother when the virus penetrates from the vagina into the uterus or transplacentally through the placenta. During childbirth, infection occurs as the newborn passes through the birth canal.
Statistics of hidden and overt forms of herpes
The body cannot overcome the pathogen on its own. The virus settles in the roots of the spinal cord, and the infected person continues to live with the disease throughout his life.
The pathogen can remain in the body for many years without causing symptoms. Therefore, it is impossible to know without testing for herpes whether a person is infected with the virus. According to WHO, type 1 herpes, which causes a rash on the lips and genitals, affects 67% of the world's inhabitants, and type 2 affects 11% of people. Only 20% of the disease occurs in the classical form, which is beyond doubt. In the rest, the course of the disease is latent or asymptomatic.
Factors causing the disease
The herpes virus may be present in our body, but not manifest itself. The disease begins to develop under certain factors - the virus is activated. The reasons for the appearance of herpes on the face are the same as the reasons for the appearance of herpetic blisters on other areas of the skin:
- hypothermia;
- violation of work and rest schedules;
- hypovitaminosis (regardless of the time of year);
- fatigue;
- chronic disorders of the immune system.
For relapses, it is also important that a periodically ill person does not attach importance to herpes and lets everything take its course, each time expecting that “it will go away on its own.”
Primary herpes
There are three periods of illness:
- Prodromal
(precursor period), during which the temperature rises, the inguinal lymph nodes become inflamed, weakness, fatigue, and headache appear. A person experiences a condition similar to the symptoms of flu and colds. If you take an antiviral drug during this period, the disease may not develop. If the symptoms are ignored and treatment is not started on time, the second period of the disease begins. - A rash
that occurs three to four days after the onset of a flu-like condition. Common symptoms include pain, heat, swelling, itching in the genital area, anus, buttocks, pubis and perineum. Soon, numerous blisters filled with clear liquid appear on the inflamed skin and mucous membranes, reminiscent of a “cold” on the lips. The rash causes pain and itching, worse at night and leading to insomnia. - Ulcerations.
After some time, the blisters burst and ulcers (erosions) form in their place, surrounded by a focus of inflammation. Contact with stool and urine on the eroded surface increases pain and complicates tissue regeneration. - Healing,
during which the ulcers gradually heal. If the genital organs are poorly cleaned, the immune system is weak, and infection occurs, the healing process is delayed.
After the ulcers disappear, the disease goes into remission. During this period, despite the presence of the virus in the body, there are no rashes on the genitals.
Herpes on the lips. Prevention.
If you have a “cold” on your lips, follow these steps:
healthy lifestyle, giving up bad habits, active sports
systematic and correct use of barrier contraception during orogenital contacts
maintaining personal hygiene
maintaining immunity (avoiding factors that reduce immunity)
treatment of caries, ENT diseases that cause a decrease in local immunity
abstaining from kissing during an active form of the disease or relapse of herpes in the intimate area
timely treatment of herpes on the lips after consultation with specialized specialists (self-medication is not acceptable!).
Briefly about the Vitagerpavac vaccine:
Compound:
— The drug is a lyophilisate for preparing a solution for intradermal administration — Contains specific inactivated antigens of herpes simplex virus types I and II grown on a continuous cell line VERO, acceptable by WHO as a substrate for the production of vaccines
Indications:
- Patients with CGI are subject to vaccination.
- Preparing women with a history of recurrent chronic herpetic infection for pregnancy.
- HIV-infected patients in stages 1-2 of the disease.
Contraindications to the use of the vaccine:
- Active stage of herpes
- Acute infectious and non-infectious diseases
- Chronic diseases in the stage of exacerbation or decompensation
- Malignant neoplasms
- Pregnancy
- Presence of active AIDS symptoms
Vaccination against herpes is carried out in institutions under the supervision of a doctor
- The vaccine is administered in the remission stage 7-10 days after the disappearance of clinical manifestations
- The vaccination course consists of 5 injections with an interval of 7-10 days
- Revaccination - after 6 months
- For complicated herpes, the 2nd and subsequent injections are administered at intervals of 10-14 days - 5 injections. Such patients are recommended to undergo 4 courses of vaccination over 1.5 - 2 years.
Where to get vaccinated Get advice
Detailed information about the Vitagerpavak vaccine and its use can be obtained from the Methodological recommendations MZ3.3.1.0002-10 “Immunization with the Vitagerpavak vaccine (herpetic culture inactivated dry) for the prevention of relapses of infection caused by herpes simplex viruses types 1 and 2”, approved by the Head of the Federal service for supervision in the field of consumer rights protection and human well-being by the Chief State Sanitary Doctor of the Russian Federation G.G. Onishchenko. **** These recommendations came into force in 2010.
*author of the material - Alimbarova L.M. Associate Professor, Ph.D.
Recurrent herpes
In 50%-70% of people the disease becomes chronic. This is facilitated by:
- untimely or incorrect treatment;
- decreased immunity, including that caused by taking medications that suppress the immune system;
- presence of other STDs;
- strict diets, vitamin deficiencies;
- state of chronic stress.
Why do patients develop relapses, during which the disease affects the same parts of the body? There are several reasons for this:
- Having penetrated the body, the virus settles in the tissues of the genital organs. As it multiplies, it affects cells deeper and deeper until it reaches nerve cells - neurons connected to each other by processes - axons. Through them, like bridges, the pathogen reaches the cells of the spinal cord, into which it introduces its DNA.
- An infected brain cell becomes an “incubator” for viruses, which periodically return via axon bridges to the mucous membrane or skin, causing new rashes. Schematically, the process is similar to the migration of birds, constantly returning to their “native places.”
- The immune system cannot kill viruses hidden in the spinal cord, but it deals with those that have left the “shelter”. Therefore, with high immunity, relapses occur rarely or not at all. But as soon as the body “loses its vigilance” - weakens, gets sick, catches a cold, is exposed to stress - the pathogens begin to overcome the immune defense. As a result, they reach their target - the skin and mucous membranes of the genital organs. Here, the increased reproduction of viral particles inside the “captured” cells begins. Cellular structures, dying, release myriads of viruses that cause inflammation, redness, swelling and the appearance of blisters. Herpes is causing another aggravation.
- Gradually, the immune system fights back the virus, and within 10 days the ulcers at the site of the rash dry out and heal. Everything returns to normal, so that at the slightest weakening of the immune system it can start again.
From the mechanism of exacerbations, it becomes clear why herpetic eruptions appear in the same places. It’s just that the virus cells return back only through the nerve cell from which they penetrated deep into the body.
Types of recurrent herpes
Depending on the number of exacerbations, several types of the disease are distinguished:
- mild, occurring up to 3 times a year;
- moderate severity, in which exacerbations occur 4-6 times a year;
- severe, accompanied by frequent exacerbations, intervals between which do not exceed a month;
- arrhythmic, in which after a period of imaginary well-being, lasting from a month to five, rashes appear. This form of herpes is characterized by a pattern - the longer the remission, the more severe the disease;
- menstrual, manifested by rashes during menstrual periods. This type of disease is severe and difficult to treat;
- subsiding, in which the manifestations of the disease constantly become weaker, and the inter-relapse periods become longer. The subsidence of the manifestations of the disease indicates the positive dynamics of treatment and the restoration of immune defense that suppresses the virus.
Atypical forms of herpes
Sometimes genital herpes is erased. These forms of the disease account for 65% of cases of the disease:
- In women,
atypical herpes resembles inflammation of the vagina or vulva. There is pain, itching and swelling of the genital organs, profuse leucorrhoea and pain during sexual intercourse. External manifestations are limited to areas of redness or pinpoint rashes. - In men,
the atypical form of the disease is similar to inflammation of the head and foreskin (balanitis or balanoposthitis). A reddish rash appears on the mucous membrane of the penis, accompanied by pain and burning, which does not look like a herpetic rash. Inflammation of the prostate gland occurs, causing pain radiating to the anal area. Damage to the urethra leads to pain and burning when urinating, and the appearance of traces of blood in the urine.
There is a latent form of the disease in which there are no clinical manifestations, but despite this, the person remains a source of infection. But imaginary well-being does not last forever. With hypothermia, loss of strength, decreased immune defense, pregnancy, stress, severe concomitant diseases and other unpleasant conditions, the virus begins to multiply rapidly and the person becomes ill.
The disease is activated by concomitant sexually transmitted infections, especially ureaplasmosis. Due to the ability to rapidly “bloom” against a background of weakened immunity, herpes occurs in 90% of HIV patients. Therefore, if herpetic rashes appear, you need to be examined for other STDs.
Features of the course of genital herpes during pregnancy
The number of positive (seropositive) reactions to herpes viruses 1 and 2 in pregnant women is 50-70%. Due to the increased load on the body and decreased immune defense, herpes often relapses during this period. But only 30% of women experience the classic development of the disease. Basically, the symptoms of herpes during pregnancy are limited to the appearance of areas of redness and cracks, which women mistake for irritation.
The manifestation of a herpetic infection caused by recurrence is not dangerous for the child. The woman’s body has already built up immunity to infection by producing antibodies—substances that protect her from the virus. Some of the antibodies will pass from mother to baby, protecting him from infection.
Only a relapse that occurs immediately before childbirth is dangerous. To prevent infection of the baby and rupture of inflamed tissues, women with a herpetic rash on the genitals are advised to deliver by cesarean section.
It is much worse when the infection is primary. Herpes belongs to a group of infections, infection of which for the first time during pregnancy leads to the birth of children suffering from developmental delays and congenital defects.
Herpes tests for pregnant women: interpretation and prognosis of pathologies in the fetus
To determine the degree of risk for the baby, a woman’s blood is taken for IgM and IgG antibodies, the concentration of which determines when infection occurred. The analysis is carried out using the ELISA method (immunofluorescence), which reacts to IgM and IgG antibodies to the virus. By the presence or absence of antibodies, you can find out whether a woman is infected and when the infection occurred:
- IgM antibodies
appear after 2-3 weeks. after the onset of the disease, therefore indicating a “fresh” infection or relapse of infection. These antibodies disappear after 1-2 months. after recovery. The presence of IgM in the analysis is a bad sign. - IgG class antibodies
- appear as protection against the virus after 2 weeks. field of infection, quickly increase the titer (concentration) and persist throughout life. Their detection means that the body encountered a herpes infection and managed to cope with it.
It is bad if a fourfold increase in IgG is combined with the detection of IgM. This means that antibodies are being formed right now, i.e. the woman is sick.
Infection with the herpes virus is determined in the laboratory. It is better to undergo such an examination twice - before pregnancy and during it.
Table of interpretation of results for herpes
| IgM | IgG | What does it mean | What to do | |
| — | — | The woman is healthy (seronegative) - she has never had herpes | Before pregnancy | During pregnancy |
| In order not to become infected, you need to avoid contact with people who have manifestations of herpes, incl. on the lips. Periodic antibody monitoring is recommended | ||||
| — | + | Female carrier (seropositive) | The infection occurred a long time ago and does not pose a danger to the child, no measures are needed | |
| + | — | Recent infection | It is better to plan pregnancy after acute symptoms subside and re-examination | Consult a doctor and undergo additional diagnostics to find out if everything is okay with the baby. |
| + | + | Exacerbation of infection | It is better to plan pregnancy after acute symptoms subside | Recurrent herpes is less dangerous than primary herpes, so the likelihood of complications and intrauterine infection is only 0.02% |
Fetal pathologies in children infected with herpes during pregnancy
The most dangerous thing for a child is primary infection of the mother during pregnancy, which leads to many complications.
| Gestational age at primary infection | Possible complications |
| I trimester (up to 13 weeks) | Fading pregnancy, miscarriages, severe malformations |
| II trimester (14-27 weeks) | Child infection, internal organ defects, fetal death |
| III trimester (29-40 weeks) | Intrauterine infection, death of a child after birth, premature birth, hearing, vision, and nervous system defects of the child. Subsequently - mental retardation. |
Etiotropic therapy of herpes simplex: focus on valacyclovir
The first description of the symptoms of a “cold on the lips” was made by the famous Roman physician Herodotus. The first attempts at organized prevention of transmission of the “creeping” disease also date back to ancient times. The Roman Emperor Tiberius issued a decree banning public kissing in the Senate to stop the spread of infection. The disease was also known to the doctors of Ancient Greece. The writings of Hippocrates mention a skin disease that can quickly spread, “spread” among people, called “herpain”, which means “creeping”; this word was subsequently transformed into “herpes” [1].
Currently, according to WHO, the infection rate of the population with the herpes simplex virus (HSV) is extremely high and is actually approaching 100%. Recurrent forms of HSV affect about 20% of the population, and the number of cases increases every year by an average of 15–17%. The incidence of herpes viral infection ranks second among infectious pathologies, second only to influenza. In the structure of the incidence of sexually transmitted infections (STIs), genital herpes (GG) is in third place after gonorrhea and non-gonococcal urethritis, and, according to foreign studies, GG is the most common STI in the world, the most common cause of genital ulcers, and also an important risk factor for HIV acquisition and transmission [2–6].
HSV enters the human body through mucous membranes and skin. The main routes of infection are airborne and sexual. Primary infection is accompanied by viral replication only at the site of invasion. Next, the virus enters the sensory paravertebral ganglia by hematogenous or axonoplasmic route, where it persists for life, often leading to the latent phase of infection [3, 7].
Virus carriage in most cases is not accompanied by clinical manifestations of the disease. As is known, a child receives antibodies to HSV transplacentally from the mother, but their titer decreases significantly by the end of the first year of life, and by the third year they are completely eliminated from the body. In 80–90% of people aged 2 to 5 years, against the background of a decrease or absence of specific antibodies, upon the first contact of the body with HSV, infection with primary herpes occurs. Infection in most cases is not accompanied by clinical manifestations, but in a number of cases primary herpes develops - an acute disease.
Most often, primary herpes manifests itself in the form of herpetic gingivostomatitis. Single or multiple vesicles appear on the mucous membrane of the oropharynx, which quickly open to form painful erosions, which are then covered with a whitish coating. The oral mucosa and gums become swollen, hyperemic, cyanotic and sharply painful. The pain syndrome can be so severe that it makes it difficult to eat and drink. Gradually, acute inflammatory phenomena subside and erosions begin to epithelialize from the periphery to the center. Complete regression of the rash occurs after 2–3 weeks. After the disappearance of clinical manifestations of primary herpes or asymptomatic infection, the herpes viral infection becomes latent. During this period, HSV remains in an inactive state in the nerve ganglia, with HSV-1 most often infecting the trigeminal ganglia, and HSV-2 reactivated primarily from the sacral ganglia. At the same time, the production of antibodies to HSV begins. However, when immunity decreases under the influence of a number of unfavorable factors, relapses of the disease can occur with varying frequency - from several days to several months or even years [2, 5, 7].
Reactivation of herpes infection depends on a number of endogenous and exogenous factors [2, 7–10]:
- the amount of latent viral DNA located in the ganglia;
- type-specific sequences in the virus genome that determine the frequency of reactivation and relapse in a specific anatomical region;
- the patient’s immune status (decrease in the levels of alpha and gamma interferons, as well as CD4+ CD8± subpopulation of T-lymphocytes);
- exposure to UV radiation and hypothermia;
- psycho-emotional stress;
- increased level of physical activity;
- changes in hormonal rhythms (for example, menstruation);
- mechanical trauma, including after invasive cosmetic procedures;
- drinking alcohol.
Despite obvious clinical symptoms, sometimes doctors have difficulty diagnosing herpes infection. Thus, according to foreign studies, only 20% of those infected with the herpes virus are diagnosed with this disease; in 60%, the herpes infection, despite obvious symptoms, remains unrecognized. And in approximately 20% of the population, the disease occurs in a latent form, and this further complicates timely diagnosis and adequate treatment of the disease [4, 8, 10].
In the past, there was an opinion that HSV-1 selectively affected the orofacial area, and HSV-2 - the external genitalia. In recent decades, data have been obtained on their general tropism: both viruses can infect both the oral and genital areas, causing acute and recurrent forms of the disease. However, the incidence of HSV-2 does correlate with sexual activity and the prevalence of the virus among potential sexual partners; Antibodies to HSV-2 are rarely detected before sexual activity begins. HSV-2 causes orafascial herpes only in 10–20% (HSV-1 - 80–90%) of cases. The role of HSV-1 in the development of HH throughout the world is constantly growing. In the UK, for example, it was found that in 50% of cases of manifestations of primary HH were caused by HSV-1, mainly in sexually active women aged 16–20 years [2, 4, 8, 11–13].
There are two alternative hypotheses that explain the mechanisms of HSV persistence in the body - statistical and dynamic. According to the statistical hypothesis, HSV is found in the cells of the paravertebral sensory ganglion in an integrated (non-reproductive) state. Under the influence of a “trigger factor,” the virus moves from the ganglion along the axon of the peripheral nerve to epithelial cells, where it replicates. It is believed that this is largely due to cellular susceptibility and weakening of the patient's immunological control. The dynamic hypothesis assumes constant replication of the virus and its release from the ganglion. Reaching along the skin nerve, HSV causes microfoci of infection, restrained by defense mechanisms, which prevents relapses or weakens the manifestations of the disease. The development of relapses is influenced by the state of local immunity, the suppression of which contributes to the replication of the virus that has reached the skin [3].
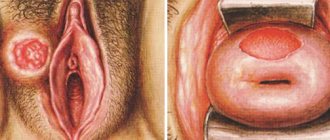
The facial area is one of the most favorite localizations for HSV manifestations. Most often, the rashes are located in the area of the red border of the lips (Fig. 1), in the vestibule and on the wings of the nose, in the perioral area, on the chin, and much less often in the area of the cheeks and forehead. With the development of a viral infection in the genital area, the rashes are often located in the pubic area, shaft of the penis, glans, on the inner layer of the foreskin, head groove - in men (Fig. 2) and in the vulva and perineum - in women. The blisters here usually exist for an extremely short time, quickly opening with the formation of painful erosions that do not heal for a long time due to constant maceration. Women may experience swelling, as well as the spread of rashes from the vulva to the mucous membrane of the vagina and cervix, which is accompanied by increased subjective sensations and the appearance of discharge. In some women, relapses of the disease coincide in time with the menstrual cycle (menstrual herpes). Herpetic rashes in this form usually appear on the skin of the buttocks and extend to the thighs. One unusual location for HSV rashes to be aware of is the fingers and palms. This localization of rashes is typical for medical workers who come into contact with the skin and mucous membranes of infected patients (for example, dentists), dressmakers due to the possibility of frequent injury, and hairdressers [4, 7, 8, 11].
In clinical practice, the most common form of recurrent herpes simplex is found. Regardless of the location of the pathological process, the disease in most cases (45–60%) begins with subjective sensations - “harbingers of relapse.” On average, a day before the appearance of the rash, mild sensations arise in the form of tingling, itching, burning, and, less often, pain. There may also be a disturbance in the general condition: a feeling of fatigue, weakness, headache, chills, a slight increase in temperature. These symptoms are usually mild, but most patients, especially with frequent recurrences of herpes simplex, immediately pay attention to them. After 1–2 days, erythema appears in the area of projection of subjective symptoms, accompanied by moderate swelling, against the background of which small grouped hemispherical bubbles begin to form. The contents of the bubbles are initially transparent, then become cloudy. Having existed from several hours to several days, they turn into erosions covered with thin serous crusts. After 7–9 days, the crusts are rejected, leaving behind a pinkish or brownish-brown secondary spot, which usually regresses after 7–14 days [7].
Thus, in the classical version, 4 successive stages of the disease can be distinguished: erythematous, vesicular, crustose, and the stage of clinical recovery. In some patients with frequent relapses of herpes in the same place or with the addition of a secondary infection, shallow small scars may remain at the site of resolved herpetic rashes. A relapse of herpes simplex may be accompanied by a reaction from the lymphatic system in the form of regional lymphadenitis and lymphangitis, the addition of a secondary infection, and symptoms of damage to the peripheral nervous system. In severe cases, skin manifestations of herpetic infection are aggravated by symptoms of general intoxication: low-grade fever, sweating, headache, malaise, joint pain, gastrointestinal disorders [2, 4, 7, 9].
The greatest difficulty in recognizing herpes viral infection occurs with abortive forms of HSV. H. Gouqerot was the first to draw attention to the existence of abortive forms of herpes simplex in 1921. A feature of these forms is the absence of the most characteristic stage of development of the pathological process - the stage of vesicle development. The occurrence of these forms of HSV infection is apparently associated with an increase in the body’s immune forces, when the pathological process does not develop beyond the initial stage of the disease. Abortive forms include erythematous, papular and pruritic. The duration of the disease in this case ranges from several days to a week [7, 8].
In rare cases, there are atypical manifestations of herpes simplex, the diagnosis of which causes great difficulties for doctors. These forms include rupioid, edematous, hemorrhagic, elephantiasis-like and impetigo-like. In immunocompromised patients, herpes infection can be severe. Severe forms include Kaposi's herpetic eczema, which occurs in children and adolescents against the background of severe atopic dermatitis, as well as ulcerative and generalized forms of HSV, often detected in patients with malignant tumors and leukemia [7].
Therapeutic tactics for managing patients with herpes viral infection are primarily aimed at effectively stopping relapses of the disease, reducing the risk of transmitting herpes to a healthy sexual partner or newborn (in the case of genital herpes), as well as preventing the development of clinical complications. The treatment strategy is determined by a number of factors: the severity of the clinical symptoms of the disease, the frequency of relapses, the state of the immune system, the presence or absence of concomitant pathology, psychosocial status, as well as the economic aspects of therapy. The main drugs used in the treatment of HSV are acyclic nucleosides: acyclovir, valacyclovir, famciclovir. They have a highly specific etiotropic antiviral effect that blocks HSV replication. Prescription of etiotropic therapy is the world standard for effective treatment of herpes infection.
Therapeutic approaches to the treatment of HSV with acyclic nucleosides include 2 regimens [2, 14–18]:
- episodic systemic antiviral therapy (done during relapse). It is most effective when initiated by the patient himself in the early stages of the disease (during the manifestation of precursors or on the 1st day of relapse). Prescribing antiherpetic treatment at a later date does not always lead to rapid relief of relapse.
- suppressive or preventive antiviral therapy, which is prescribed for a period of 6–12 months. patients: with frequent relapses of HSV (more than 6 episodes per year);
- with severe and prolonged episodes of the disease (impairing the quality of life in both HS and orofacial herpes);
- young women and girls immediately after the first episode of HS;
- with herpes simplex in association with recurrent erythema multiforme;
- with pronounced psycho-emotional reactions to the disease;
- undergoing chemical or abrasive procedures in the facial area and surgical procedures in the trigeminal nerve area;
- certain categories of medical workers in order to reduce the possibility of transmission of the virus.
According to studies, suppressive therapy prevents relapses of herpes simplex in 80% of cases and reduces the risk of transmitting the infection to a sexual partner during HH by 48% [14, 17, 19].
Systemic acyclic nucleosides presented on our pharmaceutical market have the same mechanism of antiviral action - selective phosphorylation in HSV-infected cells and competitive substrate inhibition of DNA polymerase, leading to the end of the reading of the viral DNA strand. The drugs differ in their bioavailability, solubility and concentration in the blood plasma [6, 15, 20].
The first acyclic nucleoside - acyclovir - has rightfully earned a reputation as an effective and safe drug, however, its low bioavailability (20%) and inconvenient dosage regimen (3-5 times / day), and therefore low compliance, led to the creation of drugs with higher bioavailability and compliance - valacyclovir and famciclovir [6, 15].
Valaciclovir is the hydrochloride salt of acyclovir L-valyl ester. This is a prodrug that in the body, under the influence of valacyclovir hydrolase, is quickly and almost completely converted into L-valine and acyclovir, which, after phosphorylation, acquires specific activity. Acyclovir is a structural analogue of purine nucleosides (normal components of DNA), interacts with viral DNA polymerase and blocks viral replication. Selective antiherpetic activity is due to affinity for thymidine kinase Herpes simplex types 1 and 2, Varicella zoster and Epstein-Barr virus. Under the influence of viral thymidine kinase, it is transformed into acyclovir monophosphate, with the participation of human cell guanylate kinase - into acyclovir diphosphate and then into the active form of acyclovir triphosphate. Triphosphate blocks viral DNA replication by competitively inhibiting viral DNA polymerase and inhibiting chain elongation.
The clinical efficacy and high systemic safety of valacyclovir have been proven in numerous domestic and foreign studies [21].
It was found that when taken orally, 54% of valacyclovir is absorbed from the intestine, compared to 20% when taking acyclovir. After taking valacyclovir, the same concentration of the drug substance is created in the blood that could be created only with intravenous administration of acyclovir. This feature provides the drug with a longer and more pronounced effect. When administered orally, its bioavailability is 3–4 times higher than that of acyclovir, while the safety profile is similar to acyclovir [6, 15, 16].
Two randomized, placebo-controlled, multicenter studies were conducted abroad on the treatment of exacerbations of orofacial herpes using short courses of valacyclovir. Both studies included 1,856 men and women. All patients were randomly divided into three equal groups: group 1 received valacyclovir 2 g 2 times a day for one day (one-day treatment); second - 2 g 2 times a day for the 1st day, then 1 g 2 times a day for the 2nd day (two-day treatment); the third group received a placebo. Therapy began when the first signs of exacerbation of herpes simplex appeared. As a result of the studies, similar results were revealed: the average duration of the disease statistically significantly decreased by 1.1 days with one-day treatment and by 0.7 days with two-day treatment. The number of patients in whom the progression of an exacerbation of herpetic infection was stopped or prevented increased by 6.4% with a one-day and by 8.5% with a two-day dosage regimen. The duration of existence of herpetic eruptions and subjective symptoms (pain, itching, discomfort) also significantly decreased in the groups of patients taking valacyclovir compared with the group of patients receiving placebo [22].
Valaciclovir has been proven to be highly effective as a suppressive therapy for HH. O. I. Letyaeva, O. A. Gisinger, O. R. Ziganshin, at the Ural State Medical University (Ekaterinburg), conducted a comparative study of the antiherpetic activity of acyclic nucleosides prescribed as suppressive therapy. The study involved 48 women with recurrent HH, who were divided into 2 groups. Group 1 (22 women) received acyclovir at a dosage of 400 mg 2 times/day, group 2 (26 women) received valacyclovir at a dose of 500 mg 1 time/day. Therapy was carried out for 6 months. When comparing the clinical effectiveness of the drugs, it was revealed that relapses after treatment in patients from the first group were observed 2.5 times more often than in women from the second group. Seven women receiving acyclovir for various reasons violated the prescribed regimen of taking the drug; there were only two such patients in the valacyclovir group. They noted that valacyclovir was well tolerated and had no side effects with long-term use. The frequency of detection of HSV after a year in the first group was almost 2 times higher and amounted to 13.6% - versus 7.59% in the second group of women [6].
A number of foreign studies have found that suppressive antiherpetic therapy with valacyclovir for HSV-2 reduces HIV replication, and therefore the viral load, and the effectiveness of valacyclovir in HIV-positive patients with HH was higher than when taking acyclovir. Thus, the level of HIV RNA in the blood plasma when taking valacyclovir is 2.94 copies/ml, and when taking acyclovir it is already 3.56 copies/ml [23, 24].
At the State Research Center of the Institute of Immunology of the FMBA, the effectiveness of systemic acyclic nucleosides: acyclovir, valacyclovir, famciclovir was studied in patients with recurrent HH, who had an average of about 6 relapses of the disease per year. The rashes were localized in the genital area, perineum, sacrum, and thighs. Therapy was prescribed according to two regimens: episodic (10 days) and suppressive (6 months). A total of 265 patients (96 men and 169 women) were examined and treated. A greater effectiveness of suppressive therapy was noted compared to episodic therapy: in 30% of patients with HH (regardless of the prescribed drug), the virus was again detected on the mucous membrane on the 28th day after the end of episodic therapy. Against the background of suppressive therapy after 1 month. the virus was not detected in any patient. The remission period after treatment with acyclovir was 4.1 months, with famciclovir - 9.2 months, and with valacyclovir - 10.5 months. [25].
The high effectiveness of suppressive therapy compared to episodic therapy has been proven in patients with labial herpes. The study included patients of both sexes who had 3 episodes of herpetic infection during the last year, who were divided into 2 groups: 1. those who took episodic antiherpetic therapy when the first signs of HSV appeared (in the prodrome) according to the regimen of 2 g / 2 times / day; 2. received preventive antiviral therapy according to the regimen of 1 g/day for six months. It was noted that the relapse rate within 3 months. after treatment is much higher in patients receiving episodic therapy. On average, when receiving episodic therapy, relapse occurred on the 81st day. No relapses were detected in the observed period (120 days) in patients receiving suppressive therapy. There were no statistically significant differences in the effect of the main clinical symptoms (lesion area, itching, etc.) on regression, with the exception of pain, which was significantly better reduced in the second group. The frequency of side effects in patients from the first group was higher and amounted to 6%, while in patients from the second group it did not exceed 3% [26].
At the Department of Skin and Venereal Diseases of the Moscow State Medical University, a comparative study of various forms of valacyclovir in the treatment of orofacial herpes was conducted. 40 (28 women and 12 men) patients aged 23 to 34 years were observed. The duration of the disease varied from 3 to 5 years, the frequency of relapses was 4–6 times a year. Verification of the diagnosis was carried out on the basis of a PCRrealtime molecular genetic study with determination of the viral load and HSV DNA typing. Using a random sampling method, patients were divided into two groups comparable in number, age composition, and severity of the disease. The 1st group (20 patients) was prescribed episodic therapy - the original valacyclovir 500 mg 2 times a day, the 2nd group (20 patients) received its generic according to the same regimen. The duration of treatment in both groups was 5 days. The duration of the relapse did not exceed 3–5 days. It was found that relief of itching and new rashes was comparable in both groups and took an average of 1–2 days. In 40% of patients in both groups, relapse was relieved on the 3rd day of drug use. In 55% of patients in both groups, epithelization of erosions was observed on the 4-5th day of treatment. In only 5% of patients, the use of drugs did not affect the duration of relapse. During control studies 30 days after the end of therapy, HSV DNA of types 1 and 2 was not detected in scrapings from the skin and mucous membranes in any patient. No adverse reactions were noted during or after use of both drugs. The authors conclude that both the original valacyclovir and the generic are comparable in effectiveness and safety [27].
Thus, we can conclude that long-term experience of use in domestic and foreign clinical practice and evidence-based studies on the effectiveness and safety of valacyclovir allow us to consider it the undoubted leader among systemic antiviral drugs. The drug has high antiviral activity against HSV-1 and HSV-2 and can be used both to treat relapses of herpes (episodic therapy) and to prevent relapses of infection (suppressive therapy). Prolonged therapy is of paramount importance both for adequate control of recurrent infections and for the prevention of transmission of HH to sexual partners. The absence of relapses of infection while taking the drug contributes to a significant reduction in psycho-emotional experiences about the disease, psychological rehabilitation of patients and a significant increase in quality of life. However, long-term antiviral therapy with the original valacyclovir is highly costly, and patients often cannot use it for economic reasons. In this regard, the line of generics of the original drug is constantly updated with new generic drugs. Reducing the cost of therapy increases its availability, and consequently, patient adherence to treatment. From this point of view, the use of a reproduced acyclic nucleoside, the drug Valogard (Farmak), seems promising.
Valogard is available as tablets containing 556 mg of valacyclovir hydrochloride, which is equivalent to 500 mg of valacyclovir. In the treatment of herpes zoster, Valogard helps relieve pain, reduces its duration and the percentage of patients with pain caused by herpes zoster, including acute and postherpetic neuralgia. The use of Valogard is effective in the treatment of infections of the skin and mucous membranes caused by HSV, including newly diagnosed and recurrent HH (Herpes genitalis), as well as labial herpes (Herpes labialis); prevention of recurrence of infections of the skin and mucous membranes caused by HSV, including HH; prevention of transmission of HH to a healthy partner when taken as suppressive therapy in combination with safe sex. In addition, in adults and adolescents from 12 years of age, Valogard is used to prevent cytomegalovirus infection, as well as acute transplant rejection (in patients with kidney transplants), opportunistic infections and other herpes viral infections after organ transplantation.
When treating herpes zoster in adults, the recommended dose of Valogard is 1000 mg 3 times a day for 7 days. Treatment of infections caused by HSV: adults - the recommended dose for treatment of an episode is 500 mg 2 times / day for 5 days. In more severe cases of disease onset, the duration of treatment should be increased from 5 to 10 days.
For recurrent HSV, it is ideal to prescribe Valogard in the prodromal period or immediately after the first symptoms of the disease appear. As an alternative for the treatment of labial herpes, the administration of the drug Valogard at a dose of 2 g 2 times / day is effective. The second dose should be taken approximately 12 hours (but not earlier than 6 hours) after taking the first dose. When using this dosage regimen, the duration of treatment is 1 day. Prevention of relapses of infections caused by HSV: adults - in patients with preserved immunity, the recommended dose is 500 mg 1 time / day, in patients with immunodeficiency - 500 mg 2 times / day.
To prevent infection of a healthy partner with HH, the recommended dose of Valogard for use by infected immunocompetent persons with relapses no more than 9 times a year is 500 mg 1 time per day daily for a year or more.
For the prevention of cytomegalovirus infection after transplantation: adults and adolescents 12 years of age and older - the recommended dose is 2 g 4 times / day, prescribed as early as possible after transplantation. The dose should be reduced depending on creatinine clearance. The duration of treatment is 90 days, but in high-risk patients the course of treatment can be extended.
Thus, the appearance of Valogard on the pharmaceutical market significantly expands the possibilities of the doctor and patient in choosing antiherpetic therapy.
Herpes in newborns
A child becomes infected with the pathogen from the mother in utero or by passing through an infected genital tract during childbirth. In newborns, the mucous membranes of the eyes and mouth, skin, and genitals are affected. When the pathogen enters the child’s brain, meningoencephalitis occurs, causing death or severe disability.
A generalized form is possible, in which all organs and systems of the newborn are affected. The child experiences jaundice, respiratory distress, and urinary retention. Children are restless, do not latch on to the breast, and are vomiting. Death occurs from shock, bleeding, dehydration, intoxication, and organ failure.
The likelihood of infection increases with primary infection of the mother in late pregnancy.
Diagnosis of herpes
If genital herpes is suspected, after an external examination, scrapings from the affected areas, blood, and urine are taken for examination. This will allow you to differentiate the disease from other skin lesions that have similar symptoms.
For diagnostics the following is used:
- Cultural method - during the study, the contents of the vesicles are transferred to a growing chicken embryo; if it dies, the disease is confirmed. The method is reliable, but too time-consuming.
- PCR is a test that detects viral DNA in tissues. The method allows you to calculate the pathogen even from a small amount of viral material. Effective for diagnosing any form of disease, incl. hidden. The method can be used immediately after infection before symptoms of the disease appear. PCR not only detects the virus, but also determines its type.
- Methods aimed at determining antigens and antibodies to the pathogen: ELISA - immunofluorescence diagnostics, CFR (complement fixation reaction), various types of agglutination reactions. With their help, you can identify the type of pathogen, determine its quantity and duration of infection.
A complete diagnosis of herpes virus infection allows you to make the correct diagnosis in order to prescribe treatment.
Maybe I should donate blood to find out whether I am in the active phase of the disease or not?
There are antibody tests that can be used to find out whether you have already had an illness or are in the active phase of the disease. Memory antibodies that store the data that you have been ill are called IgG. And others - IgM, show that you are sick now.
But the British Herpes Virus Association and the UK National Health Service consider these tests for diagnosing both types of HSV to be unreliable and do not recommend taking them. The American CDC also does not recommend self-testing for the herpes virus. They are needed only by certain groups:
- people with frequent relapses of herpes;
- partners of people infected with the herpes simplex virus;
- people with HIV infection or at high risk of HIV infection$
- those who are tested for STIs.
You need to remember that you are almost always contagious, but to a lesser extent when there are no symptoms, to a greater extent when they are present.
Complications of herpes
The worst thing is that a herpes infection brings not only unpleasant symptoms. This virus causes many terrible complications. The most obvious ones are:
- Irritation and dryness of the skin and mucous membranes of the genital organs;
- Cracks in the genitals caused by metabolic disorders in tissues caused by herpes;
- Adhesive and cicatricial deformities of the labia, vaginal opening, perineum, urethra and rectum. The complication arises due to the specific feature of herpetic rashes appearing on the same areas of the skin and mucous membranes
- Cervical erosion leading to cancer of the reproductive organs.
- Lacerations during childbirth caused by poor distensibility of inflamed perineal tissue.
- Infection of ulcers due to microbes entering tissues not protected by the mucous membrane;
- cicatricial deformities of the penis, provoked by constant inflammatory rashes and ulcerations.
- Chronic herpetic lesions of the genitourinary area, spreading to the urethra, bladder and kidneys.
- Herpetic proctitis is inflammation of the rectum.
- Erectile dysfunction and male and female infertility.
- Neurological symptoms caused by a viral infection of the nervous system. Patients complain of pain in the sacrum, lower back, and groin. With recurrent lesions on the inner surface of the thighs, hypersensitivity of the skin occurs, manifested by a burning sensation, crawling “goosebumps”, tingling.
In severe cases, with a pronounced weakening of the immune system, viremia occurs - viral infection of the blood leading to damage to the brain, liver, lungs, adrenal glands, and intestines. This condition, even with adequate treatment, is often fatal.
Treatment of genital herpes
It is difficult to cure such a dangerous disease. Treatment of genital and labial herpes is long and complex. Therapy includes:
- Prescription of antiviral agents that slow down the reproduction (replication) of viruses. To maintain the effectiveness of treatment during long-term therapy, it is necessary to constantly change the prescribed medications.
- The use of drugs based on interferons - proteins released in response to viral invasion. Scientists have found that a lack of this substance provokes exacerbations of the disease.
- The use of local antiviral ointments, gels and sprays that kill viruses that have penetrated the skin and mucous membranes.
- Prescribing symptomatic medications that combat the general symptoms of the disease - reducing pain, swelling, inflammation, lowering temperature, normalizing sleep.
- Local procedures - baths and irrigations that relieve pain and prevent the penetration of secondary infections.
- Taking immunoglobulins, immunomodulators and stimulators of cellular immunity, which improve the functioning of the immune system, activate the production of antiviral antibodies and prevent relapses.
Patients suffering from genital herpes are advised to avoid wearing synthetic underwear.
Prevention of infection consists of a thoughtful choice of sexual partners, compliance with hygiene rules, periodic examination by a gynecologist and the use of emergency measures at the first symptoms of the disease.
Where to get tested and cure herpes in St. Petersburg, prices
Doctors at the modern Diana Clinic treat herpes infections in St. Petersburg. Here you can take express tests for all infections - smears, blood, etc. Tests are performed using the best methods - PCR, ELISA, etc. The cost of visiting a doctor based on test results is 500 rubles. The price of tests depends on the type of examination. For example, the cost of taking blood from a vein is only 170 rubles.
Is herpes contagious? Should I now avoid kissing and sex if I have a flare-up?
Herpes is contagious and spreads from person to person. But in general, there is nothing wrong with this - the disease is not dangerous for most healthy people.
If you are afraid of infecting your partner with herpes or becoming infected yourself, always use a condom during vaginal, oral and anal sex. And during cunnilingus, create a barrier between the mucous membranes of the mouth and genitals using a special latex napkin - a rubber dam. But remember, such protection still does not provide a 100% guarantee that you will not become infected.
If you do not want to use a condom, and your relationship with your partner is long and monogamous, then a healthy partner can take a course of antiviral drugs to prevent the disease. This is advice from the Herpes Virus Association. In this way, you can reduce the risk of transmitting herpes, but you need to consult a general practitioner about treatment. He will tell you which pills to take, for how long and in what dosage.
During the period of exacerbation of herpes, it is better to avoid sex and close contacts. As soon as you have a burning and tingling sensation on your lips, blisters around your mouth or on your genitals, the virus is in an active reproduction phase. From now on until the rash and crusts disappear, it is better to refrain from close contact.