The lower jaw (mandibula) is unpaired, horseshoe-shaped, the only movable bone of the skull. It consists of two symmetrical halves, completely fused by the end of the 1st year of life. Each half has a body and a branch. At the junction of both halves in old age, a dense bony protrusion forms.
In the body (corpus mandibulae) there is a base (basis) and an alveolar part (pars alveolaris) . The body of the jaw is curved, its outer surface is convex and its inner surface is concave. At the base of the body the surfaces merge into one another; in the alveolar part they are separated by alveoli. The right and left halves of the body converge at an angle that is individually different, forming a basal arch. The shape of the basal arch is one of the main features characterizing the shape of the lower jaw. To characterize the basal arch, the latitudinal-longitudinal index is used (the ratio of the distance between the angles of the lower jaw to the distance from the middle of the chin to the middle of the line connecting the angles of the lower jaw). There are jaws with a short and wide basal arch (index 153-175), with a long and narrow one (index 116-132) and with an intermediate shape. The height of the jaw body is greatest in the area of the incisors, the smallest is at the level of the 8th tooth. The thickness of the jaw body is greatest in the region of the molars, and the smallest in the region of the premolars. The cross-sectional shape of the jaw body is not the same in different areas, which is determined by the number and position of the roots of the teeth. In the area of the front teeth it approaches triangular with the base facing downwards. In areas of the body corresponding to large molars, it is close in shape to a triangle with the base facing upward (Fig. 1-12).
Structure of the lower jaw
A - top view : 1 - head of the lower jaw; 2 - pterygoid fossa; 3 - coronoid process; 4 - mandibular pocket; 5 - molars; 6 - body of the lower jaw; 7 - premolars; 8 - fang; 9 - incisors; 10 - mental tubercle; 11 - chin protuberance; 12 - interalveolar septa; 13 - dental alveoli; 14 - chin hole; 15 - interroot septa; 16 - angle of the lower jaw; 17 - outer wall of the alveoli; 18 - oblique line; 19 — inner wall of the alveoli; 20 - retromolar fossa; 21 - buccal ridge; 22 — notch of the lower jaw; 23 - tongue of the lower jaw; 24 - neck of the lower jaw. ; B - rear view : 1 - incisors; 2 - fang; 3 - premolars; 4 - molars; 5 - coronoid process; 6 - condylar process; 7 - tongue of the lower jaw; 8 - mylohyoid groove; 9 - mylohyoid line; 10 - submandibular fossa; 11 - pterygoid tuberosity; 12 - digastric fossa; 13 - mental spine; 14 - sublingual fossa; 15 - angle of the lower jaw; 16 - canal of the lower jaw; 17 - neck of the lower jaw.
The structure of the lower jaw . B — internal view : 1 — buccal ridge; 2 - temporal crest; 3 - notch of the lower jaw; 4 - head of the lower jaw; 5 - neck of the lower jaw; 6 - tongue of the lower jaw; 7 - opening of the lower jaw; 8 - mylohyoid groove; 9 - mandibular ridge; 10 - pterygoid tuberosity; 11 - mylohyoid line; 12 - angle of the lower jaw; 13 - submandibular fossa; 14 - sublingual fossa; 15 - digastric fossa; 16 - compact substance of the lower jaw; 17 - spongy substance of the lower jaw; 18 — incisors; 19 - fang; 20 - premolars; 21 - molars
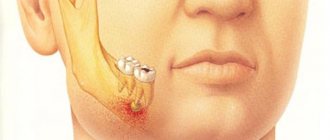
In the middle of the outer surface of the jaw body there is a chin protuberance (protuberantia mentalis), which is a characteristic feature of modern humans and determines the formation of the chin. The angle of the chin relative to the horizontal plane in modern humans ranges from 46 to 85°. On both sides of the mental protuberance, closer to the base of the jaw, there are mental tubercles (tubercula mentalia). Outside of them is the mental foramen (foramen mentale), which is the outlet of the mandibular canal. The vessels and nerves of the same name exit through the mental foramen. Most often, this hole is located at the level of the 5th tooth, but it can move anteriorly to the 4th tooth, and posteriorly to the space between the 5th and 6th teeth. The dimensions of the mental foramen range from 1.5 to 5 mm, its shape is oval or round, sometimes it is double. The mental foramen is removed from the base of the jaw by 10-19 mm; on toothless jaws of adults with an atrophied alveolar part, it is closer to the upper edge of the jaw.
In the lateral parts of the body of the lower jaw there is an obliquely located ridge - an oblique line (linea obliqua), the anterior end of which corresponds to the level of the 5-6th tooth, and the rear end, without sharp boundaries, passes to the anterior edge of the ramus of the lower jaw. On the inner surface of the jaw body , near the midline, there is a bone spine, sometimes double, called the mental spine (spina mentalis). This place is the beginning of the geniohyoid and genioglossus muscles. Below and lateral to the mental spine is the digastric fossa (fossa digastrica), in which the digastric muscle begins. Above the digastric fossa there is a flat depression - the sublingual fossa (fovea sublingualis) - a trace from the adjacent sublingual salivary gland. Further posteriorly, the mylohyoid line (linea mylohyoidea) is visible, on which the superior pharyngeal constrictor and mylohyoid muscle begin. The maxillary-hyoid line runs between the digastric and sublingual fossae at the level of the 5-6th tooth and ends on the inner surface of the jaw branch. Under the maxillary-hyoid line at the level of the 5-7th tooth there is a submandibular fossa (fovea submandibularis) - a trace from the submandibular salivary gland located in this place. The alveolar part of the jaw body contains 8 dental alveoli on each side. The alveoli are separated from each other by interalveolar septa (septa interalveolaria). The walls of the alveoli facing the lips and cheeks are called vestibular, and the walls facing the tongue are called lingual. On the surface of the body, the alveoli correspond to alveolar elevations (juga alveolaria), which are especially well expressed at the level of the canine and 1st premolar. Between the alveoli of the incisors and the mental protuberance there is a subincisal depression (impressio subincisiva). The shape, depth and width of the alveoli, the thickness of their walls are different for teeth of different groups. The alveoli of the incisors (especially the central ones) are compressed from the sides, their bottom is shifted to the vestibular compact plate, therefore the thickness of the lingual wall of the alveoli is greater than the vestibular one. The alveoli of the canine and especially the premolars are rounded, the lingual wall is thicker than the vestibular one. The deepest alveoli of the canine and 2nd premolar. The thickness of their walls is greater than the alveoli of the incisors. The alveoli of molars are distinguished by the presence of interradicular septa. In the alveoli of the first two molars there is one septum separating the anterior and posterior chambers for the corresponding roots. The alveolus of the 3rd molar is varied in shape and number of septa, which is associated with the variability of the shape of this tooth. Most often the alveolus is conical, without septa, but may have one and sometimes two septa. The walls of the alveoli of the molars are thickened due to the oblique and mylohyoid lines. This strengthens the lower molars and protects them from loosening in the buccolingual direction during transversal lateral chewing movements.
The area located behind the 3rd molar is triangular in shape and is called the posterior molar fossa (fovea retromolaris). Laterally from this fossa, on the outer plate of the alveolar part, there is a mandibular pocket (recessus mandibulae), which stretches from the 2-3rd molar to the coronoid process (Fig. 1-13).
Rice. 1-13. The structure of the lower jaw, the outer surface (diagram according to V.P. Vorobyov ), part of the dense bone substance of the outer plate has been removed: 1 - condylar process; 2 - coronoid process; 3 - opening of the lower jaw; 4 - tongue of the lower jaw; 5 - buccal ridge; 6 - retromolar fossa; 7 - incisors; 8 - alveolar elevations; 9 - chin eminence; 10 - fang; 11 - premolars; 12 — roots of teeth; 13 - canal of the lower jaw; 14 - angle of the lower jaw; 15 - chewing tuberosity; 16 — notch of the lower jaw; 17 — tongue of the lower jaw (external view); 18 - molars
The structure of the alveoli of the lower jaw is similar to the structure of the alveoli of the upper jaw. The wall of the upper third consists of two layers: solid and compact plates (inner and outer). In the area of the bottom and lower third of the alveoli, under the hard plate there is a spongy substance. In the spongy substance of the body of the lower jaw there is a canal of the lower jaw (canalis mandibulae), through which vessels and nerves pass. The canal begins with the opening of the lower jaw (foramen mandibulae), on the inner surface of the branch and ends with the mental opening on the outer surface of the body. The canal has an arcuate direction with a convexity facing down and forward, lies closest to the bottom of the alveoli of the 2-3rd molar and passes between the chambers for their roots. Small tubules extend from the canal, through which vessels and nerves pass to the roots of the teeth; they open at the bottom of the alveoli. Medially from the mental foramen, the mandibular canal continues in the form of a small tubule to the midline and along this length gives off lateral branches to the bottom of the alveoli of the anterior teeth.
The branch of the lower jaw (ramus mandibulae) has outer and inner surfaces, anterior and posterior edges, which pass into the coronoid process (processus coronoideus) and the condylar process (processus condylaris), respectively. These processes are separated by the notch of the lower jaw (incisura mandibulae). The coronoid process serves to attach the temporal muscle, and the condylar process serves to form the temporomandibular joint (TMJ). The shape of the mandibular ramus varies individually (Fig. 1-14).
Rice. 1-14. Extreme forms of the basal arch of the lower jaw , ventral view: A - wide and short; B - narrow and long
The condylar process has a head (caput mandibulae) with an articular surface for connection with the mandibular fossa of the temporal bone and a neck (collum mandibulae). On the anteromedial surface of the neck of the condylar process there is a pterygoid fossa (fovea pterygoidea) - the attachment site of the external pterygoid muscle. The head of the articular process is flattened and occupies a position in which the axes drawn through the largest size of both heads intersect at the foramen magnum at an angle of 120-178°, open anteriorly. The shape and position of the head are individually different and depend on the operating conditions of the TMJ and the condition of its components. Deviations leading to changes in the volume and direction of movement in the joint change the shape and position of the articular heads. The anterior edge of the ramus of the lower jaw laterally passes into an oblique line on the outer surface of the jaw body, and medially reaches the posterior alveoli, thus limiting the retromolar fossa. The medial part of the ridge, formed at the site of the transition of the anterior edge into the walls of the posterior alveoli, stands out under the name of the buccal crest (crista buccinatoria), from which the buccal muscle begins.
The posterior edge of the branch passes into the base of the jaw, forming an angle (angulus mandibulae), the value of which ranges from 110 to 145° (usually 122-133°) and changes throughout life. In newborns it is close to 150°, decreases in adults with preserved teeth and maximum chewing load, and increases again in old people with complete loss of teeth (Fig. 1-15). The outer surface of the branch contains a masticatory tuberosity (tuberositas masseterica), which occupies most of the branch and the angle of the jaw and is the site of attachment of the masticatory muscle. On the inner surface of the branch in the area of the angle and adjacent sections there is a pterygoid tuberosity (tuberositas pterygoidea) - the place of attachment of the medial pterygoid muscle. On the same surface, in the middle, there is an opening for the lower jaw (foramen mandibulae), which is covered in front and above by an inconsistently pronounced bony protrusion - the tongue (lingula mandibulae). Above and anterior to the uvula is the mandibular ridge (torus mandibularis) - the place of attachment of two ligaments: the maxillary-pterygoid and the maxillary-sphenoid. The branches of the lower jaw are usually turned outward, so that the distance between the condylar processes of the right and left branches is greater than the distance between the outer points of the angles of the jaw. Can be distinguished as extreme forms of the jaw with maximally and minimally deployed branches. The degree of divergence of the branches depends on the shape of the upper half of the face. With a wide upper half of the face, the branches of the lower jaw are less developed than with a narrow upper half of the face. The smallest width of the branch, which usually falls in the middle of its height, ranges from 23 to 40 mm (usually 29-34 mm). The width and depth of the jaw notch are also individually different: the width of the notch is from 26 to 43 mm (usually 32-37 mm), the depth is from 7 to 21 mm (usually 12-16 mm). People with a wide upper half of the face usually have jaws with the greatest width of the notch and vice versa.
Temporomandibular joint
The temporomandibular joint consists of articulations between three surfaces; the mandibular fossa, the articular tubercle (from the flat part of the temporal bone) and the head of the mandible.
This joint has a unique mechanism; The articular surfaces of the bones never touch each other - they are separated by the articular disc. The presence of such a disc divides the joint into two synovial articular cavities, each of which is lined with a synovial membrane. The articular surface of the bones is covered with fibrous cartilage.
The structure of the maxillary processes
The maxillary apparatus is formed by two paired bones.
They are divided into a body and four appendages:
- zygomatic;
- alveolar;
- frontal;
- pair of palatine processes.
The structure of the frontal process
The process starts from the maxillary base. In front it is attached to the nasal bone, the upper edge is adjacent to the nasal part of the frontal region of the face. The posterior part of the process is adjacent to the lacrimal ossicle.
The middle region of the process faces the inside of the nasal space. The middle turbinate is attached to it by the anterior edge. The anterior lacrimal crest runs along the sides of the frontal process, and the lacrimal groove runs nearby.
The structure of the zygomatic process
Adjacent to the upper edge of the body of the jaw, attached to the zygomatic bone. Exactly in the interval from the lower edge of the zygomatic process and the alveolar eminence belonging to the first painter lies the zygomaticalveolar ridge.
The main task is to redistribute the load during the process of chewing food and biting, so it is directed from the teeth to the zygomatic bone.
The structure of the palatine process
Palatine processes of the upper jaw, paired, symmetrical. Going from the right and left to the middle, they unite and form the anterior edge of the hard palate. Externally, they are thin, horizontally located bone plates.
They are attached to the alveolar process anteriorly and laterally. Their posterior part is fixed with the horizontal plate of the palatine bone.
The upward looking, smooth part of the palatine process of the maxilla faces the inside of the nasal space. The lower part, which is rougher, goes into the oral cavity. This zone, which has a large number of palatine grooves, is saturated with vessels, nerve fibers and pathways of the palatine glands. The largest groove is the one running along the bend of the alveolar formation.
A nasal ridge runs along the center of the nasal surface of the process, from the front part of which a bony outgrowth is formed - the anterior nasal spine.
The structure of the alveolar process
Alveolar ridge location
This process is a continuation of the body of the upper jaw. It is a bone structure curved in the shape of an arc. It consists of two halves, symmetrically located towards each other and connected in the center by an intermaxillary suture.
The maxillary alveolar structure includes alveoli, recesses. The roots of the teeth are located and firmly attached to them. There are eight alveoli in total, all of them are isolated from one another by a bony septum.
Holes are formed in the bottom surface to allow nerve fibers and the blood supply system to approach the teeth. These holes are also separated by bone plates. The shape, number and size of holes vary depending on the location and structure of the tooth.
Important: the shape of the holes also changes with a person’s age, during the development and change of teeth.
An alveolar elevation is formed for each alveolus; it can be felt through the gums at the roots of the teeth. The size of the alveolar elevation is influenced by the person’s age, the anatomical shape and size of his jaw and teeth, as well as the characteristics of the root system.
The formation of this bone structure occurs as a person grows and teeth erupt. During this time, its body thickens and increases significantly in size. First, giving the opportunity to grow baby teeth, and then permanent ones, the roots of which require a lot of space.
Important: sometimes dentists examine the alveolar eminence before removing a tooth; this manipulation provides information about the complexity of the upcoming procedure.
Causes of anomalies
Let's look at the main reasons why defects occur:
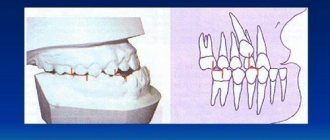
- Genetic factor. Mesial and distal occlusion are most often inherited.
For parents, knowing about the high risk of such a defect occurring in their child, it is easier to control treatment in childhood, during the formation of the maxillofacial system. - Developmental anomalies in the prenatal period. Various pregnancy pathologies can often affect the formation of the fetal dental system.
- Birth injury. Mesial occlusion is caused by displacement or dislocation of the baby's lower jaw during difficult childbirth.
- “Wrong” habits in childhood. These include constant pacifier or finger sucking, improper nipple latching, and improper sucking during bottle feeding. If the hole in the nipple is too large, the child’s lower jaw practically does not work when sucking and remains undeveloped.
- Frequent sinusitis and rhinitis, due to which the child constantly breathes through his mouth. With such breathing, the development of facial bones is disrupted.
- Violation of tooth change. Early removal of baby teeth often causes abnormal maxillofacial development.
- Incorrect prosthetics, lack of prosthetics.
- Hypertonicity of the masticatory muscles due to stress provokes abrasion of the incisors and displacement of the jaws.
- Various injuries of the maxillofacial area.