The main function of the salivary glands is the formation of a secretion that helps soften food, form a food bolus and facilitate its movement through the esophagus.
A whole complex of glands is responsible for the formation of saliva in the human oral cavity:
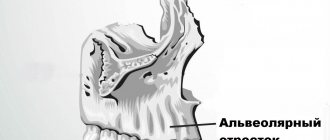
- three pairs of large ones
: parotid (located just below the auricle), submandibular (located under the lower jaw) and sublingual (located on both sides of the tongue); - many small ones
, divided by location into molar, labial, lingual, buccal and palatal.
In medical practice, there are various pathological conditions of the salivary glands that affect their functionality and cause a number of unpleasant symptoms. Patients of different age groups are diagnosed with: sialadenitis, mumps, duct blockage, salivary stone disease, benign and malignant tumors.
The provoking factors contributing to the development of the inflammatory process are:
- infectious diseases: influenza, pneumonia, encephalitis, etc.;
- disturbances in the functioning of the endocrine system;
- injuries and surgical interventions;
- taking medications that reduce saliva production and thickening;
- dehydration and malnutrition.
Each disease produces its own set of symptoms, the severity of which depends on the nature of the inflammation and the location of the affected gland.
General information
Sialadenitis is an inflammatory process in the salivary glands. In humans, there are three pairs of salivary glands in the oral cavity, which secrete saliva and discharge them into the oral cavity through special ducts, thereby ensuring a normal digestive process. These are the parotid , submandibular and sublingual glands.
The main functions of saliva are to soften food and also facilitate the process of swallowing it. During the inflammatory process, the production of saliva becomes difficult, and during the process of eating a person feels significant inconvenience. During the development of the disease, pain, swelling of the face, etc. are noted. If the process progresses, a purulent cavity or tumor may form. The disease develops in both young children and adults. Damage to the salivary glands requires consulting a doctor and carrying out the prescribed treatment. The ICD-10 code for sialadenitis is K11.2. How inflammatory diseases of the salivary glands manifest themselves, what treatment is most effective in such cases - this will be discussed in the article.
Prevention of violation
There are no vaccines or specially developed drugs against sialadenitis. The only exception is mumps. To prevent the development of the disease, the child is offered an inactivated vaccine against measles, mumps and rubella. All children over 1 year of age are vaccinated against the disease. After the vaccine, stable immunity to the pathogen remains in 96% of vaccinated people.
There are also nonspecific measures to protect against sialoadenitis, including:
- regular oral hygiene;
- timely treatment of wounds and mouth ulcers;
- elimination of chronic foci of infection;
- prevention of saliva stagnation in infectious diseases.
Treatment of salivary gland blockage should be carried out promptly. Otherwise, the disease threatens infection of the soft tissues of the face and further infection of the body. The consequences of sialadenitis require resuscitation measures to preserve the life and health of the patient. The list of dangerous consequences of pathology also includes: rapid destruction of enamel, disruption of oral microflora, chronic inflammation of the gums. For this reason, it is important not to bring your health condition to a critical level.
Pathogenesis
There are three pairs of major salivary glands in the human mouth. The parotids are located under the auricle in front and are the largest. The submandibular muscles are located under the lower jaw. Accordingly, sublingual - under the mucous membrane of the floor of the oral cavity on both sides of the tongue. These glands produce saliva, which is produced through ducts located in the oral cavity. Saliva ensures normal digestion by softening solid foods.
Reactive-dystrophic pathological processes occur in stages. At the initial stage , there are no symptoms of the inflammatory process, but the lymph stagnates near the blood vessels and ducts. The vessels become overfilled with blood, the lymph around the gland ducts stagnates, and the connective tissue loosens. The acini (terminal sections of the salivary gland) are completely preserved, and mucopolysaccharides and mucin accumulate in them.
The second stage of the disease is characterized by the presence of signs of an obvious chronic inflammatory process. There are signs of atrophic changes in the end parts of the gland, infiltrates are detected in the sclerotic stroma. Fibrous tissue appears near the excretory ducts of the gland. Lymphocytes and epithelial cells accumulate in the lumen of the ducts.
At the third stage, almost complete atrophy of the gland parenchyma occurs, and it is replaced by connective tissue. Blood vessels dilate, the ducts of the gland dilate or narrow if they are compressed by connective tissue.
Treatment of dacryoadenitis
If an acute form of the disease develops, hospitalization of the patient will be required; therapy in most cases is conservative. Treatment of chronic dacryoadenitis is selected depending on the underlying pathology.
Treatment of acute dacryoadenitis
The patient is prescribed antibacterial drugs. For maximum effectiveness, it is recommended to simultaneously use sulfonamides - antimicrobial medications that temporarily suppress the proliferation of bacterial agents.
In addition, it is necessary to take non-steroidal anti-inflammatory drugs - Indomethacin, Voltaren, Diclofenac.
For two to three weeks, drops are dripped into the conjunctival cavity without fail and local agents are applied:
- solutions of glucocorticosteroid drugs - to relieve inflammation and allergic reactions;
- solutions of non-steroidal anti-inflammatory drugs;
- antiseptic drugs;
- antibiotic ointments.
Classification
Taking into account the peculiarities of the process, acute and chronic sialadenitis are distinguished.
According to nosological independence, two forms of the disease are distinguished:
- Primary is an independent disease.
- Secondary – a complication in the development of other diseases ( flu , sore throat , etc.).
Taking into account the causes of the development of the disease, the following are distinguished:
- Traumatic – a consequence of injuries and the influence of external factors.
- Radiation – a consequence of irradiation.
- Toxic – a consequence of chemical influence.
- Infectious – develops after infection.
- Allergic.
- Autoimmune.
- Obstructive - a consequence of blockage of the excretory duct by a foreign body or cicatricial narrowing of the duct.
According to the location of the lesion there are:
- Inflammation of the sublingual salivary gland - the inflammatory process of the sublingual gland is also called sublingual gland.
- Inflammation of the parotid salivary gland - in this case, the cheeks swell and there are signs of general intoxication. Sialadenitis of the parotid gland is also called mumps .
- Sialadenitis of the submandibular salivary gland is an inflammatory process of the submandibular salivary gland. When this gland is damaged, calculous sialadenitis , which is characterized by the development of stones in the ducts of the salivary glands or in their parenchyma.
Taking into account the condition of the parenchyma, the following forms of the disease are distinguished:
- interstitial sialadenitis - only stromal damage occurs.
- parenchymal sialadenitis - in addition to the stroma, the parenchyma is also affected.
Depending on the nature of the inflammatory process, the following forms of sialadenitis are distinguished:
- Purulent.
- Serous.
- Hemorrhagic.
- Connective tissue.
- Destructive.
- Granulomatous.
- Fibroplastic.
- Sialadenitis without deformation of the gland.
- Sialadenitis with scarring of the gland.
There are also epidemic and non-epidemic sialadenitis.
- The epidemic form of the disease develops against the background of viral diseases and infections.
- Non-epidemic form - diagnosed if there is a blockage of the salivary gland. Such blockage can develop as a result of injuries, salivary stones, or foreign bodies entering the ducts.
Theory and practical experience in ultrasound diagnosis of salivary gland pathology
Ultrasound machine HM70A
Expert class at an affordable price.
Monocrystal sensors, full-screen display mode, elastography, 3D/4D in a laptop case. Flexible transformation into a stationary scanner with a cart.
In domestic and foreign literature there are many works devoted to sialogy (from the Greek Sialon - saliva and logos - study) - the science of diseases and injuries of the salivary glands, methods of their diagnosis and treatment. According to various authors, diseases of the salivary glands account for up to 24% of all dental pathologies. Currently, in clinical practice, the most common are dystrophic, inflammatory diseases of the salivary glands (sialoadenoses, sialadenitis), as well as tumors and congenital malformations of the salivary glands. In addition, pathological changes in the salivary glands often accompany other diseases (diabetes mellitus, bronchiectasis, sarcoidosis, liver cirrhosis, hypertriglyceridemia, lymphogranulomatosis, etc.).
Various instrumental methods are used to diagnose diseases of the salivary glands [1]:
- radiography (if the formation of stones in the ducts of the salivary glands is suspected, but in 20% of the stones of the submandibular salivary glands and 80% of the parotid salivary glands are non-radiographically opaque);
- sialography (examination of the ducts of the salivary glands with a radiopaque substance, is rarely useful in differentiating tumors from inflammatory processes, but it can help differentiate the mass formation of the salivary glands from formations in neighboring tissues. In patients with suspected autoimmune disease of the salivary glands, a characteristic pattern of saccular expansion may be detected ductal system. In case of acute infection of the salivary glands, sialography should not be performed [2]);
- computed tomography together with sialography;
- ultrasound method (is the most accessible, safe and informative in the process of differential diagnosis of the pathological condition of the salivary glands).
Anatomy of the salivary glands [3]
There are three pairs of major salivary glands (SG) and many small ones. The large ones include paired parotid, submandibular and sublingual SGs. The parotid salivary gland (PSG) is located on the outer surface of the branch of the lower jaw at the anterior edge of the sternocleidomastoid muscle, as well as in the retromandibular fossa. Dimensions vary widely: length 48-86 mm, width 42-74 mm, thickness 22-45 mm. The OSJ is covered by the parotid fascia, which is its capsule and is tightly fused with it. Sometimes, at the anterior edge of the parotid duct, there is an additional lobule measuring 10-20 mm, which has its own duct flowing into the parotid. The parotid duct emerges from the gland at the border of its upper and middle thirds, then it passes along the outer surface of the masticatory muscle parallel to the zygomatic arch and turns 90° inward, penetrating the fatty tissue and buccal muscle. The projection of the parotid duct onto the skin of the cheek is determined on the line connecting the tragus of the auricle and the corner of the mouth. The parotid duct opens in the vestibule of the oral cavity at the level of 1-2 large molars. The diameter of the duct is on average 1.5-3.0 mm, its length is 15-40 mm. The thickness of the gland contains the branches of the external carotid artery, the facial nerve and its branches, and the auriculotemporal nerve. There are many lymph nodes around the OUSG and in its parenchyma (Fig. 1), which can serve as a primary or secondary collector for draining lymph from teeth and oral tissues.
Rice. 1.
Lymph nodes in the thickness of the parotid salivary gland.
The submandibular salivary gland (MSG) is located in the submandibular triangle between the body of the mandible and the anterior and posterior bellies of the digastric muscle. The dimensions of the gland are: anteroposterior 20-40 mm, lateral 8-23 mm, superior-inferior 13-37 mm. Posteriorly, the PNJ is separated from the OSJ by a process of the fascia propria of the neck. The medial surface of the gland in the anterior section lies on the mylohyoid muscle. The submandibular duct, bending over the posterior edge of this muscle, is located on the lateral surface of the hyoglossus muscle. Then it goes between the medial surface of the hyoid gland and the genioglossus muscle to the point of its exit in the area of the hyoid papilla. The facial artery and its branches, the lingual artery and the veins of the same name pass through the gland.
The sublingual salivary gland (SSG) is located on the floor of the mouth in the sublingual region parallel to the body of the lower jaw. The dimensions of the gland are: longitudinal 15-30 mm, transverse 4-10 mm and vertical 8-12 mm. The duct of the parathyroid gland passes along its inner surface and opens in the region of the anterior section of the sublingual ridge independently or together with the submandibular duct. Sometimes the PJS duct flows into the middle section of the PJS duct.
The minor salivary glands - labial, buccal, lingual, palatine, incisive - are located in the corresponding areas of the mucous membrane. They can be a source of development of adenocarcinomas of the oral cavity.
Pathology of the salivary glands
SG malformations are rare. The most common are anomalies in the size of the glands (agenesis and aplasia, congenital hyperplasia (Fig. 2) and hypoplasia), their location (heterotopia, accessory glands), and anomalies of the excretory ducts (atresia, stenosis, ectasia, cystic transformation, ductal dystopia).
Rice. 2.
Hyperplasia of the left sublingual salivary gland.
Sialadenitis is a large group of polyetiological inflammatory diseases of the gastrointestinal tract (Fig. 3). Primary sialadenitis - sialadenitis considered as an independent disease (for example, mumps). Secondary sialadenitis is sialadenitis that is a complication or manifestation of other diseases (for example, sialadenitis with influenza). The echographic picture for different etiologies is not very specific. Etiology has clinical significance in determining treatment tactics.
Rice. 3.
Sialadenitis of the right submandibular salivary gland.
According to the etiological factor, sialadenitis is classified [4] into:
- sialadenitis developing under the influence of physical factors (traumatic sialadenitis, radiation sialadenitis (Fig. 4) occurs during radiation therapy of malignant tumors of the head and neck);
- sialadenitis developing under the influence of chemical factors (toxic sialadenitis);
- infectious sialadenitis (routes of infection penetration into the fluid: stomatogenic (through ducts), contact, hematogenous and lymphogenous);
- allergic and autoimmune sialadenitis (recurrent allergic, Sjogren's disease and syndrome, etc.);
- myoepithelial sialadenitis caused by a pathological process, previously designated as a benign lymphoepithelial lesion. The term benign lymphoepithelial lesion was first used by JT Godwin in 1952, replacing the concept of Mikulicz disease;
- obstructive sialadenitis, which develops when there is difficulty in the outflow of saliva due to obstruction of the excretory duct with a stone (Fig. 5-7) or thickened secretion, as well as due to cicatricial stenosis of the duct. According to the prevalence of the process, they distinguish between focal, diffuse sialadenitis and sialodochitis - inflammation of the excretory duct. The course of the process can be acute or chronic;
- pneumosialadenitis, which develops when there is air in the gastric tissue in the absence of a bacterial gas-forming infection. Air enters the gland from the oral cavity when the pressure there increases through the duct. Pneumosialadenitis is typical for a number of professions, primarily for glassblowers and musicians playing wind instruments.
Rice. 4.
Post-radiation sialadenitis.
Rice. 5.
Stone of the duct of the submandibular salivary gland.
Rice. 6.
Stone in the parenchyma of the submandibular salivary gland.
Rice. 7.
Stone in the duct of the submandibular salivary gland.
Tumors of the salivary glands
Tumors of the salivary glands are divided into two groups: epithelial and non-epithelial. Epithelial tumors predominate in adults (95%). In children with SG, epithelial and non-epithelial tumors are equally common. In addition to true tumors, processes resembling tumors (tumor-like lesions) develop in the GS.
Among epithelial tumors of the gastrointestinal tract, benign neoplasms are distinguished, as well as malignant ones - carcinomas.
Benign epithelial neoplasms of the stomach include ductal papillomas, adenomas and benign sialoblastoma. SG adenomas are divided into two groups: polymorphic (the most common SG adenoma) and monomorphic (all other) adenomas. Tumors of different structure, origin and prognosis were artificially included in the group of monomorphic adenomas.
Pleomorphic (polymorphic) adenoma (mixed tumor of the gland) is a adenoma of the gland, built from two types of cells: ductal epithelium and myoepithelial cells. Macromorphological picture. The tumor is usually an elastic or firm nodule of lobulated grayish-white tissue, usually partially encapsulated. Typical of a pleomorphic adenoma is the so-called chondroid stroma, resembling hyaline cartilage. Variants of the echographic image of pleomorphic adenomas are presented in Figure 8.
Rice. 8.
Pleomorphic adenoma of the gastrointestinal tract.
Warthin's tumor is an adenolymphoma in which multiple cystic cavities are formed, covered with double-layered epithelium. The papillae protrude into the lumen of the cysts. A pronounced proliferation of lymphoid tissue occurs in the tumor stroma. This tumor almost exclusively develops in the parotid gland.
Other types of benign tumors are less common. These are benign oncocytoma (oxyphilic adenoma), basal cell adenoma, tubular adenoma, benign cystadenoma sialoblastoma.
Among benign primary non-epithelial tumors, the most common are hemangioma, lymphangioma, neurofibroma and lipoma.
Among malignant non-epithelial tumors, malignant lymphomas are more often found (they arise, as a rule, against the background of myoepithelial sialadenitis, Sjögren's disease and syndrome).
Tumor-like lesions of the salivary glands
Rice. 9.
Salivary gland cysts.
- Salivary gland cysts (mucoceles). There are two types of mucocele of the gland: the retention type (retention cyst of the small gland, formed when saliva is retained in the excretory duct) and the type of interstitial secretion, when, when the wall of the duct is injured, saliva enters directly into the fibrous tissue surrounding the gland. Mucoceles in the floor of the mouth are also called ranulae.
- Cysts of the excretory ducts of large SGs are pronounced dilatation of the excretory duct due to retention of secretions in it. Blockage of salivary outflow can be caused by various reasons: tumor, stone, thickened mucus, post-inflammatory stenosis, even cicatricial obliteration of the lumen.
- Sialoadenosis (sialosis) is a non-tumor and non-inflammatory symmetrical increase in SF due to hyperplasia and hypertrophy of secretory cells. The outcome of sialosis is often SG lipomatosis. The process has a chronic relapsing course. Sialosis occurs in a number of diseases and conditions: diabetes mellitus, hypothyroidism, malnutrition, alcoholism, liver cirrhosis, hormonal disorders (hypoestrogenemia), reactions to medications (most often antihypertensive), neurological disorders.
Adenomatoid hyperplasia of small SGs leads to their increase to 0.5-3.0 cm in diameter. The causes of adenomatoid hyperplasia are trauma and prolonged exposure to ionizing radiation.
Oncocytosis is age-related changes in secretory cells and epithelium of the ducts of the gastrointestinal tract. In this case, the SF may slightly increase, but usually their value does not change.
To summarize, I would like to note that ultrasound using Doppler sonography in many of our observations helped to accurately determine the nature of the pathological process in the gastrointestinal tract. However, this diagnostic method does not allow one to unambiguously confirm or refute the malignant nature of the formation of the salivary glands.
Literature
- Benign and malignant tumors of soft tissues and bones of the face. A.G. Shargorodsky, N.F. Rutsky. M.: GOU VUNMTs, 1999.
- Topographic anatomy and operative surgery. I.I. Kagan, S.V. Chemezov. M.: GEOTAR-Media, 2011.
- Salivary glands. Diseases and injuries. V.V. Afanasiev. M.: GEOTAR-Media, 2012.
- Inflammatory diseases of the tissues of the maxillofacial area and neck. A.G. Shargorodsky. M.: GOU VUNMTs, 2001.
Ultrasound machine HM70A
Expert class at an affordable price.
Monocrystal sensors, full-screen display mode, elastography, 3D/4D in a laptop case. Flexible transformation into a stationary scanner with a cart.
Causes
There are a number of factors that provoke the development of sialadenitis:
- Wrong approach to oral hygiene.
- Diseases in which the composition and viscosity of saliva changes.
- Postponed surgeries.
- Infectious diseases - influenza, encephalitis , herpes , ARVI , etc.
- Oral diseases – caries , pulpitis , periodontitis , etc.
- Dry mouth.
- Treatment with chemotherapy , radiation therapy .
- Diabetes.
- Disorders of mineral metabolism leading to stone formation.
The epidemic type of the disease develops as a result of infectious processes. Most often, this condition develops with mumps (mumps) . This virus is transmitted from infected people through airborne droplets.
The non-epidemic form of the disease is usually associated with blockage of the glands. This happens with injuries or exposure to foreign bodies. Also the cause of the development of this form of the disease is the so-called salivary stone disease ( sialolithiasis ). If a person develops sialolithiasis of the submandibular salivary gland, the resulting stones may block the ducts.
Causes of disease development
Functional disorders of the lacrimal glands are the result of a disorder of innervation or reflex irritations. They can occur with autoimmune and endocrine diseases, when undergoing hormone therapy, when exposed to external irritants (frost, strong wind, smoke, bright light), prolonged work at the computer, and in heavy smokers.
The main causes of inflammation of the lacrimal glands are infectious diseases (influenza, tonsillitis, scarlet fever, mumps, pneumonia, acute respiratory viral infections, measles, typhoid fever). Other factors can also provoke the inflammatory process - narrowing of the tear ducts, trauma, a foreign body in the eye, overheating or hypothermia of the body, prolonged exposure to a dusty room, conjunctivitis, diabetes mellitus.
Symptoms of salivary gland inflammation
The signs that inflammation manifests largely depend on where exactly the pathological process is localized.
submandibular sialadenitis develops , symptoms may be as follows:
- Pain in the submandibular area, which becomes worse when chewing.
- Swelling in the area of the salivary gland, which may increase.
- Temperature increase.
- Taste of salt or pus.
- Swelling of the face.
- Redness and swelling in the mouth.
If sialadenitis of the sublingual salivary gland , similar symptoms develop. The mouth of the exit ducts of the gland turns red and swelling develops. The pain may be more severe than with submandibular sialadenitis .
With parotid sialadenitis, more pronounced symptoms appear. There is marked swelling and asymmetry of the face, redness of the skin. The patient is bothered by dry mouth. The pain intensifies when palpating the affected area. The temperature rises and the general condition worsens. Shortness of breath may bother you . Palpation of the parotid salivary gland leads to the appearance of cloudy saliva mixed with pus.
Symptoms of salivary stone disease can manifest themselves in a similar way. I am concerned about soreness and dry mouth. At the same time, it is difficult for a person to open and close his mouth.
Symptoms of dacryoadenitis
Clinical manifestations vary depending on the form of dacryoadenitis. Acute is accompanied by the following symptoms:
- pain when pressed;
- hyperemia, swelling and drooping of the outer edge of the upper eyelid;
- deformation of the palpebral fissure (becomes similar to the letter S) or complete closure.
The disease begins abruptly, and swelling may spread to the temples and half of the face, causing the palpebral fissure to completely close.
Acute dacryoadenitis causes enlargement of the lymph nodes, after which they begin to hurt. The eyeball becomes deformed, deviating towards the lower and inner side, and also protrudes slightly from the orbit, causing double vision. There is a disturbance in the movement of the visual organs to the outer and upper side. If you pull back the upper eyelid, you can see that the conjunctiva is swollen and red.
If acute dacryoadenitis occurs in a child with weak immunity, then in severe cases an abscess or phlegmon of the gland may develop, spreading to the space behind the organ of vision.
In addition, symptoms of acute dacryoadenitis include a general deterioration in health:
- temperature increase;
- the appearance of headaches;
- sleep and appetite disturbances.
The duration of the disease is usually 7-21 days.
Chronic dacryoadenitis does not manifest symptoms of an acute inflammatory process. The lacrimal gland thickens and enlarges, and pain occurs less frequently when pressed. The color of the skin of the affected area does not change. Due to the enlargement of the lacrimal gland, the palpebral fissure on the outside may narrow. The visual organs move as usual. Clinical manifestations do not develop immediately, so it may take quite a long time before the patient sees an ophthalmologist.
Dacryoadenitis with syphilis
The disease may develop with primary and tertiary syphilis. In the first case, the gland enlarges and thickens, but there is no pain. In the second, a soft formation forms in the affected area. Diagnosis of dacryoadenitis is carried out by collecting anamnesis, during which the doctor identifies signs of syphilis from other body systems.
For Mikulicz's disease
This disease is a chronic lymphostasis of the lacrimal and salivary glands. It develops against the background of leukemia and pseudoleukemia. In this case, the symptoms of dacryoadenitis are that the glands are enlarged on both sides (mainly submandibular, in more rare cases - parotid, sublingual). The magnification is so strong that the organ of vision shifts to the lower and inner side. The eye may bulge forward. The eyelids droop, the lymph nodes enlarge, causing the palpebral fissures to become narrow. The patient experiences dryness in the oral cavity and organs of vision. This is due to the fact that the function of the glands decreases.
Pseudotumorous pathology
The disease belongs to the group of orbital pseudotumors. Such diseases arise due to the inflammatory process, and their course resembles the development of a malignant tumor. Pseudotumors are considered to be autoimmune pathologies, despite the fact that to date it has not been precisely established why they appear.
Inflammation of the lacrimal gland is characterized by the following symptoms:
- iron increases noticeably;
- when pressed, a dense, smooth formation is felt, there is no pain;
- the upper eyelid swells and droops slightly.
With a long course, the inflammatory process spreads to adjacent tissues. Then the connective tissue grows and scars appear.
For sarcoidosis
This systemic disease belongs to granulomatosis. It is not known exactly what exactly causes them. With this disease, a large number of small nodes form in the skin, lymphatic system, and internal organs. Formations in granulomatosis are of the same type and clearly limited from adjacent tissues. Dacryoadenitis, as a rule, develops against the background of general symptoms of the disease, but can appear without involving other organs. In the first stages, the disease does not manifest itself in any way and is characterized by a long course. The lacrimal gland usually enlarges evenly, the sarcoid node is not clearly visible. There is no pain when pressed. Diagnosis is difficult.
For chronic tuberculosis
The lacrimal gland swells, it gradually increases in size, and pain is felt when pressed. In addition, other symptoms of tuberculosis are noticeable - the cervical lymph nodes are enlarged, changes in the lungs are visible on x-rays.
Tests and diagnosis of sialadenitis
Diagnosis of sialadenitis is carried out using clinical, instrumental and laboratory methods.
The essence of clinical methods is the collection of complaints and anamnesis. The doctor also examines the patient.
Laboratory methods - a general blood and urine test, a biochemical blood test are performed. A study of saliva is also carried out, in which, during the inflammatory process, leukocytes and an admixture of pus are found.
Hardware methods - diagnosis of diseases of the salivary glands involves, first of all, sialography with contrast, that is, x-rays of the gland. With the help of such a study, stones, narrowing of the lumen of the excretory duct, as well as other obstacles to the normal secretion of saliva are determined.
CT, MRI - it is advisable to carry out if the presence of stones is suspected.
Ultrasound - allows you to determine the structure of the gland and the characteristics of the inflammatory process.
Thermosialography – the temperature of the gland is measured.
Salivary gland biopsy - performed under ultrasound guidance.
Sialendoscopy.
Decoding the result
The interpretation of the ultrasound of the salivary glands is carried out by a specialist who compares many parameters, deviations in which, alone or in combination with other factors, can serve as the basis for making a diagnosis. As a rule, the specialist pays attention to the size of the glands, their contours and position, and the condition of the lymph nodes. In addition, echogenicity (the ability of tissues to reflect sound) is important on ultrasound of the ear glands. The rate of echogenicity varies from organ to organ. However, the indicator is extremely important for making a diagnosis, since reduced echogenicity of the ear glands detected by ultrasound may indicate swelling or inflammation, and an increased indicator may be a sign of a neoplasm.
Treatment with folk remedies
Traditional methods in the treatment process can only be used as auxiliary ones. It is advisable to use the following methods of traditional treatment:
- Rinsing the mouth - for this purpose, a solution of soda and salt can be used (1 teaspoon of salt and soda for 1 glass of water). It is also recommended to rinse the mouth with infusions of herbs - sage, oak bark, calendula, chamomile. To prepare the infusion for rinsing, 2 tbsp. l. raw materials should be poured into 3 liters. boiling water Leave for an hour and rinse your mouth several times a day. In case of purulent processes, rinsing is contraindicated.
- To stimulate salivation, it is recommended to consume lemon juice, cranberry juice, and chewing candies.
- 5 tbsp. l. pine needles pour 1 liter of water, bring to a boil, leave and take 50 ml 2 times a day.
Treatment
Therapy for sialadenitis is carried out in a hospital. Most often, signs of pathology are eliminated with the help of medications and physiotherapeutic procedures. Less commonly, doctors resort to surgery to cleanse or remove the gland. The operation is indicated for purulent or gangrenous type of problem.
For mumps, patients are prescribed antiviral drugs. Symptomatic treatment is also carried out, aimed at reducing the temperature and relieving pain in the affected area.
Acute blockage of the salivary gland requires complex therapy. To normalize the function of the gland, patients are prescribed a special salivary diet. The diet includes crackers, sour fruits and vegetables, and berries. Drink a 1% solution of pilocarpine hydrochloride orally. The substance promotes contraction of the muscles located next to the salivary gland. All measures are aimed at accelerating the removal of foreign objects and pathogenic particles by enhancing the secretory function of the gland.
If the disease is infectious, the use of antibacterial agents is required. Penicillin antibiotics and antiseptic solutions are injected into the ducts to disinfect the affected area (Miramistin, Dioxidin)
To relieve swelling and inflammation, compresses with Dimexide are applied to the problem area. The procedure is carried out twice a day for 30 minutes. The drug also reduces the intensity of pain.
Additionally, the inflamed glands are heated using UHF. If the situation worsens, a novocaine-penicillin blockade is performed. The procedure is necessary to prevent infection of neighboring tissues.
Chronic sialadenitis is treated according to a different scheme:
- The inflamed ducts are massaged daily with the introduction of antibacterial drugs. The procedure acts as a prevention of purulent complications of sialadenitis.
- Injections with novocaine are made into the subcutaneous fat to improve the secretory function of the glands.
- For 10 days they undergo daily treatment with electric currents.
- To prevent exacerbation of the pathology, iodolipol is injected into the problem area once every 3 months.
Diet
Diet to boost immunity
- Efficacy: therapeutic effect after 3 weeks
- Terms: 1-3 months or more
- Cost of products: 1600-1800 rubles. in Week
During the treatment period, it is recommended to eat properly to strengthen the immune system. Sometimes doctors advise sticking to the so-called salivary diet. However, if a patient is diagnosed with calculous sialadenitis, then in this case it is necessary to carry out mechanical removal of stones, since nutritional correction will not help cure the calculous type of disease.
The salivary diet involves introducing the following products into the menu:
- Sauerkraut, sour berry fruit drinks, lemon juice, pickles.
- Citrus.
- Sour lollipops.
- Fresh vegetables.
- Juices from cabbage, carrots.
- Rose hip decoction.
You need to exclude from your diet foods that contribute to the formation of stones:
- Cheeses, cottage cheese.
- Tofu.
- Almonds, sesame.
- Fish.
- Milk.