Treatment of caries for children Caries is a very common dental lesion, which is important to pay attention to. Baby teeth are no exception; they need to be treated, despite the fact that even at a young age they are completely replaced with permanent ones. The health of permanent teeth, the oral cavity as a whole, and the child’s quality of life depend on the condition of baby teeth. One of the main principles in this case is high-quality prevention, professional treatment tactics and minimal intervention.
Causes of caries
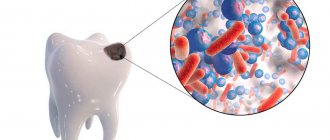
Caries occurs “thanks” to microorganisms living in the thickness of dental plaque. These bacteria - primarily streptococci, lactobacilli and actinomycetes - process food debris that remains on the teeth and produce acids that corrode the tooth enamel, leaching calcium from it. The tooth enamel begins to deteriorate.
The activity of bacteria varies from person to person: it is higher if a person brushes their teeth irregularly or not thoroughly enough, since soft interdental plaque is an excellent nutrient medium for them.
Why does caries occur in childhood?
It is known that caries is a pathological process that occurs in the hard tissues of teeth under the influence of internal and external factors. Carious lesions arise as a result of the “work” of cariogenic bacteria living in the oral cavity.
In this article
- Why does caries occur in childhood?
- Features of caries of milk teeth
- Symptoms of carious lesions in baby teeth
- Why is caries treated for young children?
- How is caries treated in children?
- Methods for treating childhood caries without drilling
- Invasive treatment of caries
- Do they give anesthesia to children?
- Prevention of childhood caries of primary teeth
By processing carbohydrates that enter the mouth with food, these bacteria produce acid. It is this that contributes to the destruction of enamel, dentin and other tooth tissues. Several factors contribute to the proliferation and active activity of cariogenic bacteria, which ultimately leads to the development of caries in children.
- Improper dental hygiene.
Insufficient cleaning from plaque, infrequent cleaning.
- Eating high in carbohydrates.
Children who eat a lot of sweets and flour, drink sweet compotes at night, and snack on chocolates are more susceptible to developing caries. A favorable breeding ground for microbes is formed in their mouth.
- Reduced immunity.
Weakened immune defense does not allow the body to effectively resist negative influences, so children with weak immunity develop caries more often.
- Features of intrauterine development.
The formation of teeth occurs in the first trimester of pregnancy, and it can be affected by the lifestyle, health, and previous diseases of the expectant mother.
These factors contribute to the fact that tooth enamel begins to lose mineral substances, cariogenic microbes multiply in the mouth, and as a result, dental caries develops.
Possible causes of caries in children
- Poor dental hygiene.
- Poor nutrition. Bacteria multiply more actively in the mouth of people who prefer foods with a high content of easily digestible carbohydrates and sugars.
- Insufficient production of saliva, its increased viscosity.
- Lack of solid foods in the diet, which helps remove soft plaque.
- Lack of calcium and phosphorus in food.
- Lack of fluoride in water (below 1.5 mg/l).
- Crowding of teeth, since it is impossible to clean plaque from the interdental space in this case.
- Some diseases predispose to increased activity of the carious process: diabetes mellitus, thyroid disease.
Do they give anesthesia to children?
Many parents are concerned about how to painlessly treat teeth in children under 5 years old.
Non-invasive methods are absolutely painless. If a cavity needs to be prepared, anesthesia may be required. Children most often undergo two-stage anesthesia. First, the gum area is treated with an anesthetic gel, which numbs the injection site, and then an anesthetic injection is given.
In some cases, it is advisable to use sedation - when the child is introduced into a relaxed state of half-asleep using a special gas. Choosing the optimal method of pain relief and treatment is the responsibility of the dentist.
Clinical picture of caries
The first stage of the carious process
Caries occurs in the spot stage and in the superficial layers of enamel. Then we observe a stain on the surface of the tooth, which gradually becomes more dull, rough and porous.
The second stage of the carious process
If the enamel is chipped and a defect is formed, the tooth becomes more sensitive to irritants. Transient pain appears after eating cold, sweet and sour foods.
The third stage of the carious process
A carious cavity in dentin (tooth tissue located under the enamel). In this case, toothache appears depending on the situation, for example, when chewing on a diseased tooth or when there is a sudden change in the temperature of food, air, or when food gets into the cavity of a damaged tooth.
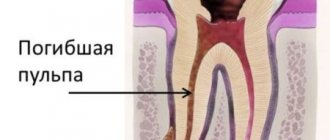
The fourth stage of the carious process
With further destruction, a deep carious cavity appears in the tooth, which gradually increases in size, so that eventually the tooth is destroyed and the pain appears spontaneous and constant. At this stage, an urgent visit to the dentist is necessary, as this indicates damage to the nerve of the tooth. In this case, it is not always possible to save the tooth.
Meet our tooth fairies and find out prices
Stages of the carious process
The carious process on baby teeth is more intense, this is due to the structural features of the enamel and dentin of children's teeth. The hard tissues of the tooth are poorly mineralized, the surface of the tooth is more porous, and the dental pulp is immature.
The first stage is a carious spot. If the plaque that has formed on the surface of the tooth is not removed within 24 hours, then the bacteria inhabiting it begin to actively reproduce. acids are formed that wash away fluoride and calcium from tooth enamel. As a result, cariogenic bacteria penetrate deeper into the tooth and damage it. This is the first stage of caries - a carious spot. At this stage, the process is quite easily reversible; it can be cured even without a drill. There is a modern and safe method of chemical-mechanical treatment of tooth enamel with a special gel - ICON. At this stage, it is almost impossible to determine tooth decay on your own, which is why it is recommended to visit the dentist regularly.
In the second stage - initial caries , bacteria damage dentin, thereby forming visible tooth decay. The tooth begins to react briefly to cold and sweet stimuli. If there is a cavity (even the smallest one), ICON will not help - invasive treatment with removal of carious tissue and filling is required.
The third stage is middle caries . Here, bacteria cross the enamel-dentin boundary, and dentin destruction occurs faster than enamel. In an adult, the process will be slow. Since protective dentin begins to be produced, the tooth “fights” the disease, but in baby teeth such protection is significantly lower. At this stage there is already a carious cavity, which is probed. And the reaction to irritants is more pronounced, food begins to get stuck in the cavity.
The fourth stage is deep caries. Bacteria penetrate closer and closer to the center of the tooth, to the pulp. By this time, most of the dentin has already been destroyed, there is a large carious cavity, the tooth reacts strongly to irritants: cold. hot, sweet, the pain goes away only with time, but at this stage the tooth itself does not hurt yet. In all three cases: from initial to deep caries, the tooth can be cured by placing a regular filling. inlay or crown, leaving the tooth “alive”.
The fifth stage is pulpitis. This is already inflammation of the neurovascular bundle located in the pulp chamber. These tissues are destroyed. Accompanied by severe throbbing pain, both in response to irritants and spontaneously. Very often, parents pay attention to tooth decay in their child only at this moment, the toothache is very acute and a visit to the dentist is urgent.
The sixth stage is periodontitis. This is an inflammatory process outside the tooth. It can be asymptomatic in an already pulpless tooth and lead to complex consequences. such as bone loss. At this stage, the tooth hurts when eating hot food or biting.
Diagnosis of caries in children
How to recognize caries in a child? A parent cannot always do this, since caries in children becomes noticeable only when there is already a hole in the tooth. Often a child is brought to the dentist “just to check his teeth,” and the doctor finds several caries after examining him with instruments.
The usual methods for diagnosing caries are inspection and probing. As a rule, this is enough to determine the presence of caries. The depth of the lesion can be assessed based on the child’s complaints and by x-ray examination.
Deep caries in a child is visible to the naked eye. At the same time, deep carious lesions on a tooth will almost always require x-rays so that the doctor can understand how far the carious process has gone, whether it is possible to save the tooth or whether removal is necessary.
Special offer
Participate in the promotion
Promotion “1+1”: child and parent
You have entrusted NovaDent with the treatment of your child’s teeth, as a token of gratitude we are giving you a free consultation with any specialist (surgeon, implantologist, therapist, orthodontist, hygienist), as well as an orthopantomogram (panoramic photograph of the teeth) sent by email.
Take time for your health and take advantage of this great offer! Participate in the promotion
Expert of the article you are reading: Lapshina Maria Aleksandrovna Dentist, pediatrician
21 years
Clinical experience
Krasnogorsk
Moscow region, Krasnogorsk, Podmoskovny Boulevard, 5
+7
Free consultation with this specialist
Caries of primary teeth in children
Caries in young children can occur immediately after the first teeth erupt. There are many reasons: the course of pregnancy, illnesses in the first years of life, the rules and regimen of feeding, and the nature and composition of early complementary foods.
Bottle or “circular” (circular) caries in children affects the necks of the upper incisors and canines, since in these areas the enamel is usually the least durable.
Caries of primary teeth in children at the initial stage manifests itself in the form of a chalky or white spot on the tooth. If you visit the dentist frequently, such caries can be stabilized. However, the enamel of baby teeth with stains can be damaged and destroyed very quickly. First, the stain becomes grayish or brownish, then softens and falls off, and after 2-3 months the carious process already damages the dentin. A cavity forms on the tooth - a clearly visible dark depression. If you see a cavity with a pigmented bottom (“hollow”) on a child’s tooth, do not put off going to the dentist, since at this stage the tooth already needs surgical and restorative treatment.
Anesthesia for the treatment of childhood caries
Local anesthesia. Used in the vast majority of cases. There are 2 types: application and injection anesthesia. The first does not involve an injection. The risk here is that the child may swallow saliva containing lidocaine. Injections are safer and more effective.
Anesthesia. Used if the child is restless or simply afraid to have their teeth treated. This method is common in the West. Many parents are afraid of memory impairment due to general anesthesia. However, this happens extremely rarely. In addition, general anesthesia becomes the only option when you need to fill several teeth at once in one trip to the dentist. After all, this can take 2 or more hours. Before general anesthesia is administered, the child must undergo the following tests:
- Blood biochemistry.
- General blood and urine analysis.
- Electrocardiography.
- Blood for sugar.
Before the introduction of general anesthesia, you cannot eat for 6 hours, and drink for 4 hours. The child is gently put to sleep using a sedative gas containing sevoflurane. To wake him up, it is enough to increase the oxygen supply. This can be done at any time. After recovery from anesthesia, all reflexes are restored within the first 15 minutes.
Caries of permanent teeth in children
Newly erupted teeth have lower mineralization, which is finally completed only by 4-5 years after eruption. Young permanent teeth are especially vulnerable in the first year of development. The enamel on them is easily permeable to caries bacteria, so a junior schoolchild should be helped to brush his teeth and be sure to consult with a dentist about the need to seal the fissures and make a protective coating for the enamel.
Meet our tooth fairies and check prices.
Caries of permanent teeth in children is a serious medical and social problem. A feature of the pathogenesis of caries of permanent teeth in children in the first years after their eruption is the initial physiological hypomineralization of hard dental tissues: both enamel and dentin [1, 2]. It is known that the final maturation of the hard tissues of the tooth occurs within 2-3 years after eruption, mainly due to the remineralizing potential of the oral fluid. Accordingly, during the period of eruption and maturation, hard tissues are the most susceptible to caries. When treating caries of permanent teeth with immature enamel, it is necessary to take into account the above pathogenetic features [3, 4]. It is known that the use of orthophosphoric acid in the treatment of caries of teeth with a low degree of mineralization leads to excessive decalcification of hard tissues, which increases the risk of secondary caries. In this regard, in the clinic of pediatric therapeutic dentistry, the use of self-etching adhesive systems and preventive filling materials is very promising in the treatment of caries. By the age of 7-9 years, the prevalence of caries is 95-100%, in children 11-12 years old it decreases to 70-80% due to the physiological change of teeth and the formation of a permanent dentition. Starting from 13-14 years of age, the prevalence of caries increases. Treatment of caries is a therapeutic measure aimed at preventing the transition of the process into its complications.
Description of a clinical case
On December 4, 2012, patient E., 7.5 years old, was admitted to the specialized department of the Department of Pediatric Therapeutic Dentistry with complaints of pain in tooth 3.6 from chemical irritants; the pain quickly went away after rinsing the mouth with water.
Previous and concomitant diseases:
chicken pox; ARVI 1-2 times a year; there were no surgical interventions; Allergy history is not burdened.
History of the disease:
Over the past month, he has noticed pain in tooth 3.6 from chemical irritants, which passes quickly. We contacted the clinic of the Department of Pediatric Therapeutic Dentistry of Moscow State Medical University for oral sanitation.
Visual inspection:
the configuration of the face is not changed, the skin is of normal color and clean. Visible mucous membranes are pale pink, evenly moisturized; The red border of the lips is dry and tight. Opening the mouth is free, palpation of the temporomandibular joint is painless; palpation of the masticatory muscles (masticatory, temporal) is painless. Palpation of regional lymph nodes (submandibular, mental, anterior cervical) - submandibular lymph nodes are palpated on the right and left, 0.5 cm in diameter, slightly painful (the patient was sick 2 weeks ago), mobile, dense elastic consistency.
Oral examination
Vestibule of the oral cavity:
the frenulum of the lower lip has a normal attachment, the vestibule of the oral cavity is shallow (depth less than 5 mm). The frenulum of the upper lip has a normal attachment. A clear secretion is secreted from the excretory duct of the parotid gland.
Bite:
replaceable, there is a tendency to retroposition of the lower jaw.
Examination of the oral cavity itself:
the mucous membrane of the gums, hard palate, sublingual area is pale pink, moisturized; the frenulum of the tongue has a normal attachment; the dorsal surface of the tongue is covered with a small amount of white plaque.
kp = 4 kp = 2
The teeth of both jaws are covered with a soft plaque (Fig. 1).
Figure 1. Oral examination. Soft plaque on the teeth of the upper and lower jaw.
OHI-S=2.4 (hygiene level unsatisfactory)
Examination of tooth 3.6
3.6 - on the occlusal surface there is a carious cavity, within the enamel and dentin, filled with softened dentin, probing is painful along the bottom of the carious cavity (Fig. 2);
Figure 2. Dentition of the lower jaw, sublingual region. 7.3, 8.3 - fillings, carious cavities on the vestibular and lingual surfaces; 8.5 - filling, caries; 3.6 - caries.
3.6 - there is a carious cavity on the vestibular surface, within the enamel and dentin, probing is painful along the walls of the cavity.
Preliminary diagnosis (according to ICD-10): 3.6 - dentin caries K 02.1.
Additional examination methods
The patient was prescribed orthopantomography to clarify the diagnosis for tooth 3.6 (Fig. 3, 4).
Figure 3. Orthopantomogram.
Figure 4. Enlarged fragment of the orthopantomogram, tooth 3.6.
In addition, an orthopantomogram will be required in the future, since the patient will be sent to the department of orthodontics and pediatric prosthetics for consultation due to multiple early removal of primary teeth and a tendency to retroposition of the lower jaw.
Diagnosis
3.6, 4.6, 7.3, 8.3, 8.5 - dentin caries (K 02.1); soft plaque (K 03.6); meteorological cheilitis (K 13.0); small vestibule of the oral cavity; distal occlusion (K 07.2) (according to the opinion of the orthodontist).
Treatment plan:
1) professional oral hygiene;
2) sanitation of the oral cavity - treatment of caries 3.6, 4.6, 7.3, 8.3, 8.5;
3) recommendations on oral hygiene, training in oral hygiene;
4) rational nutrition, correction of the carbohydrate factor;
5) remineralizing therapy at home, local fluoride prophylaxis in the dental office 4 times a year;
6) consultation with a dental surgeon;
7) consultation with an orthodontist;
 control examinations once every 4-6 months.
control examinations once every 4-6 months.
Treatment
The surfaces of the teeth were cleaned using rotating brushes with paste (Fig. 5).
Figure 5. Cleaning tooth surfaces from soft plaque.
Under application anesthesia, mandibular anesthesia and infiltration anesthesia on the buccal side with a local anesthetic solution were performed (Fig. 6).
Figure 6. Performing mandibular anesthesia.
The carious cavity on the occlusal surface was opened with diamond burs,
necrectomy with carbide burs, formation of a cavity for filling (Fig. 7).
Figure 7. View of the prepared tooth cavity 3.6. A cavity was formed on the vestibular surface in a similar way. When probing, the bottom is dense, healthy dentin “creaks.”
Using a caries detector, the quality of the preparation was checked (Fig. 8).
Figure 8. a - insertion of a caries detector; b — assessment of the formed cavity.
A self-etching two-component system was used as the bonding system.
Compomer prophylactic material (A2) was used as a filling material. A general view of the restoration is shown in Fig. 9.
Figure 9. General view of restoration 3.6.
After checking the occlusal relationships (Fig. 10, a),
Figure 10. a - alignment of occlusal relationships.
The filling was grinded and polished (Fig. 10, b)
Figure 10. b - polishing the restoration.
using diamond burs with yellow markings, silicone caps, brushes with paste (Fig. 10, c).
Figure 10. c - rotating tools for grinding and polishing.
The final view of the restoration of tooth 3.6 is shown in Fig. eleven.
Figure 11. Final view of tooth restoration 3.6.
Recommendations were given: 1) correction of oral hygiene; 2) advice on rational nutrition, correction of the carbohydrate factor; 3) the use of rosehip oil, an oil solution of vitamin A for the treatment of meteorological cheilitis; 4) continued sanitation of the oral cavity.
Conclusion
Recently, cases of early damage to the first permanent molars by caries have become more frequent. The first permanent molar - the first tooth to appear in the mouth - is affected by caries unnoticed by parents and the child, since they mistake it for a temporary tooth that will soon “fall out”. But this tooth - the main tooth in occlusion - should be preserved as long as possible. Of course, preventive measures must be taken. The simplest and most affordable way is fissure sealing (invasive or non-invasive), but in order to catch the moment when sealing is still possible, all parents must be notified en masse of the need to perform it in advance.
In situations, as in this clinical case, when the carious process has affected the deep layers of enamel and dentin, it is necessary to treat caries and restore tooth function. Up to 12 years, in permanent teeth with immature enamel, composite materials using the total etching technique have limited use; preference is given to self-etching systems and further restoration of the crown part from a compomer material, which combines the positive aspects of composite materials (packability, abrasion resistance, aesthetic characteristics ) and glass ionomer cements (fluoride release).
Types of caries
According to the place of manifestation
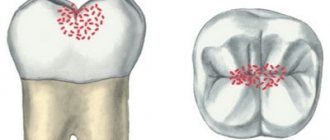
- Fissure caries affects the grooves and grooves on the surface of the chewing teeth - fissures. Food debris accumulates inside the fissures, which means bacteria that cause caries.
- Approximal (interdental) caries occurs between adjacent teeth, especially often when teeth are crowded. It is very difficult to clean out food debris from the interdental spaces, so plaque often accumulates there.
- Cervical caries destroys the enamel next to the gum, since it is in this place that it has lower mineralization and minimal thickness.
- Root caries characterizes the destruction of the tooth root under the gum. To diagnose root caries, additional methods are needed, since it is difficult to detect visually. In children, it occurs when there is severe destruction of baby teeth.
According to the speed of development
- Compensated caries proceeds slowly; many months can pass from the spot stage to the development of deep caries. In some cases, the process may even be reversible, but only by restoring the mineralization of the enamel in a tooth with caries in the stain stage.
- Decompensated caries develops quickly and on several teeth at the same time; sometimes from the stain stage to deep caries it can take less than 2-3 months. Numerous foci of carious lesions, increased sensitivity of teeth to irritants, deterioration of the enamel structure are signs of decompensated caries.
How to brush your teeth?
Each specialist has his own opinion about when to brush a child’s teeth using toothpaste. The composition of the toothpaste must correspond to the age of the baby - all information about this can be found on the packaging. Toothpastes for children under three years of age should not contain fluoride. Children at this age, not having the skills to rinse, swallow the paste. If a large amount of paste containing fluoride enters a child's body, serious health problems may arise, so in this case you should consult a doctor immediately. Children from about 4 years of age after brushing their teeth can partially spit out the remaining toothpaste. This is why toothpastes for this age contain fluorides. The maturation of tooth enamel is accelerated if hygiene products containing active fluoride are regularly used. This has been proven to help reduce the risk of tooth decay.
Children's toothbrushes are varied. For very small children, you can use special finger brushes, with which mother can easily remove plaque from her child’s teeth. By the age of 2.5-3 years, you gradually need to give the child a toothbrush in his hand and teach him to brush his teeth on his own.
Choose a toothbrush with soft bristles, the width of which corresponds to 2-3 teeth. It is recommended to change it every month, because frayed bristles can hurt your gums and are also a source of bacteria. The child should have an individual toothbrush; it should be stored separately, without a case, with the bristles facing up. Before brushing your teeth, as well as after the procedure, the brush should be rinsed well with running water. Oral care with additional hygiene products
- You can use dental floss or floss when all 20 baby teeth have erupted (most often at the age of 2-2.5 years). Dental floss should be used if the teeth fit tightly together. This must be done very carefully so as not to accidentally injure the gums.
- Dental rinses (elixirs) can be used as an additional hygiene product for children with a high risk of developing caries. Special children's elixirs contain fluoride in the amount that a child of a given age needs. You can use it twice a day after brushing your teeth or eating foods that contain a lot of sugar. Chewing gum should not be given to children until after 3 years of age. The sweeteners they contain (sorbitol, xylitol, etc.) have a beneficial effect on tooth enamel and prevent the occurrence of caries. Chewing gum also promotes increased salivation and self-cleaning of the oral cavity. They can be given to children regardless of the presence or absence of a filling in the mouth. Chewing duration is no more than 10-15 minutes.
Complications of caries in children: pulpitis and periodontitis
Pulpitis is an inflammation of the neurovascular bundle of a tooth (where its nerve endings and blood vessels are located). Pulpitis can develop from caries very quickly - within 3-4 months. Up to three years of age, pulpitis of primary teeth in children usually develops on the front teeth, after three years - on the chewing teeth. In acute pulpitis, the pain in the tooth is very severe, the temperature may rise, and the child refuses to eat.
Chronic pulpitis in children can occur asymptomatically or be similar in symptoms to deep caries. Such pulpitis develops under fillings or in teeth with advanced caries. If a child of any age develops pulpitis, he must be treated immediately, since pulpitis, in turn, is fraught with serious complications.
Periodontitis is an inflammation of the tissues located near the root of the tooth. Acute periodontitis in children develops quickly and leads to severe pain in the affected area, especially when pressing or touching hot food. The general condition deteriorates sharply, the body temperature can rise to 39 degrees, the child cannot eat. Chronic periodontitis in children can develop slowly and is characterized by mild pain when pressing on the tooth or chewing on the affected side. The mucous membrane next to the tooth swells and becomes bright red.
Complications of childhood caries
It is important to treat baby teeth. After all, deep caries can penetrate the tissue so much that it damages the permanent dentition. In addition, the condition of temporary teeth subsequently affects the child’s bite. Removal leads to abnormal growth of the jaw. As a result, permanent teeth may appear out of place. Because of this, the child will have to wear braces.
Deep caries leads to inflammation of the pulp, periodontitis, and the formation of basal cysts. Treating these problems is very difficult and painful. It requires root canal filling.
If periodontitis starts, it can cause an abscess and even osteomyelitis. This is already dangerous for the child's life.
Treatment of caries of primary teeth in children
Preservation of primary teeth is very important for the growth of the facial skeleton and for the subsequent development and correctness of permanent teeth. If baby teeth have to be removed, chewing food, diction, and the development of the rudiments of permanent teeth suffer. Therefore, treatment of caries in children must begin in a timely manner. Treatment methods for caries in children may vary depending on the stage of the process and the age of the child.
Fluoridation and mineralization
We have already written above that in order to treat caries at the stain stage, it is sometimes sufficient to remove the stain and ensure the restoration of the enamel composition. For this purpose, there are solutions, gels and resins containing calcium and fluorine. Remineralization of enamel is also a good prevention of caries.
Fissure sealing
This procedure is recommended to prevent the development of fissure caries on primary and permanent chewing teeth. The dentist cleans the fissures and seals them with a special liquid sealant that penetrates the enamel fissures and then hardens under the influence of special light. A sealant containing fluoride or calcium fills the recesses of the tooth surface and protects this surface from damage for several years, creating a mechanical obstacle to the penetration of plaque and microorganisms into these physiological recesses of the tooth.
Sealing
The traditional technology for treating medium and deep dental caries in children is filling. Under local anesthesia, the dentist opens the cavity and cleans it. If a child’s caries is not very deep, sometimes you can do without a bur, using only hand tools. The dentist then places a filling.
Meet our tooth fairies and check prices.
Treatment of caries in a child under anesthesia
Sometimes we suggest parents treat their child’s teeth under general anesthesia, in medicated sleep. If the child is small and cannot sit with his mouth open, if several teeth need to be treated at once, if we are talking about a special child, then treatment in medicinal sleep will be the only opportunity to provide him with full dental care.
We also have a video in which we filmed the treatment process in medicated sleep. Look