Dental clinic No. 2
In order to always anticipate surprises, the doctor must be prepared to expand access to the dental cavity to facilitate the preparation of complex root canals and carefully examine the floor of the tooth cavity to look for such anatomical variations.
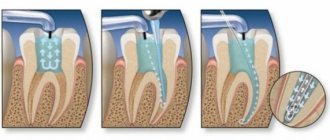
Endodontic dogma is that careful cavity and root canal preparation and obturation is the key to successful canal therapy. Endodontic preparation can be divided into cavity preparation (coronal preparation) and root canal preparation (radicular preparation). Transferring the principles of preparation of carious cavities according to Black in relation to endodontics, the following endodontic principles of preparation can be distinguished: creation of external, comfortable, retention (holding) and resistant forms. A complete preparation along the entire length of the tooth is the external form. In turn, the external shape can be modified for a comfortable shape to accommodate anatomy, canal curves and instrumentation. In some endodontic techniques, the canal can be prepared with slight retention of the first gutta-percha point (retention form). But the most important is the resistant form, in which the so-called “apical stop” is prepared in the apical section, a barrier that protects the tissues of the apical periodontium from the removal of the filling material and irrigating solution beyond the apex and creates a limit for the compaction of gutta-percha in the canal (Fig. 1).
| pic 1 |
Basic tools for preparing a tooth cavity. For trephination of an intact tooth crown, Ingle JI suggests using a cone-shaped fissure bur with a working rounded top for a turbine tip (Fig. 2 B). It is first directed at a right angle in the long axis of the tooth to remove only the enamel. Then it should be located parallel to the longitudinal axis of the tooth (Fig. 2 C, D). The roof of the tooth is removed using a low-speed tip with a round bur (Fig. 2 E, F) No. 2, 4 less often No. 6 of regular length (9 mm) for molars and premolars or surgical length (14 mm) for incisors and canines. The protrusion (“shoulder”) inside the cavity of the anterior teeth, which prevents the direct passage of the endodontic instrument into the root canal, is eliminated using a long, conical diamond bur on a turbine drill (Fig. 2 G). The remaining pulp from the pulp chamber is removed using a spherical bur No. 1 or 2 (Fig. 2 H).
| pic 2 |
It is necessary to remember the following axioms of the structure of the coronal cavity of the tooth and root canals when searching for root canal orifices (Ingle JI). 1. The two root canal orifices of the first maxillary premolars are located further buccal and lingually than is usually realized (Fig. 3 A). 2. The orifices of the mesiobuccal canals of the upper and lower molars are located under the mesiobuccal cusps, and the external shape should often be more expanded due to these cusps (Fig. 3 B, C). 3. The mouth of the palatal canal in the upper molars is located not so far to the palatal wall of the tooth cavity, but in the center of the medial half of the tooth (Fig. 3 B). 4. The orifice of the distal-buccal canal of the upper molars is not located so distally-buccally, but almost directly to the buccal side of the palatal canal (Fig. 3 B). 5. The orifice of the distal canal in mandibular molars is not so distally located, but in fact almost exactly in the center of the tooth (Fig. 3 C, E). 6. The orifice of the mesial-lingual canal of the lower molars is not so far mesial-lingual, but in fact directly buccally from the orifice of the distal canal (Fig. 3 B). 7. Certain anatomical variations that occur quite often: The mesial buccal root of the maxillary first molar often (up to 95% [4]) has an additional mesiopalatal canal located exactly oral to the orifice of the main canal. The mouth of the additional channel is located in the groove, which forms the mouth of the main channel like a “comma tail”. This entire groove should be examined to locate the mouth of the accessory canal (Fig. 3 B). The lower second molar often has a common mesial orifice, which divides approximately 1 mm below the floor of the dental cavity into mesial buccal and mesial lingual canals (Fig. 3 D). The lower first and second molars may have two distal canals with separate orifices or a common one. orifice, like the previously described medial canals (Fig. 3 E). The mandibular first premolar often has a second canal that branches off from the main canal buccally or lingually a few millimeters below the floor of the dental cavity (Fig. 3 E). The lower incisors and canines often have two canals. The medial lingual canal is hidden under the internal protrusion (“shoulder”), which corresponds to the lingual girdle. This protrusion should be removed with a #2 long shank round bur or finishing diamond cone bur to allow proper exploration of the root canals (Figure 3 G).
| pic 3 |
Table 1. Degree of deviation of teeth from the central axis
When preparing a tooth cavity, it is necessary to take into account the degree of deviation of the tooth from the central axis in the vestibulo-oral and medio-distal projections (Table 1). The upper incisors and canines are inclined palatally by 29°, the lower incisors are inclined lingually by 20°. The lateral lower and upper incisors are deviated medially at 17 and 16? respectively. If the doctor does not know about these deviations or ignores them, then he can make a perforation and a ledge on the walls of the tooth cavity (Fig. 4. A, B, C)
| pic 4 |
Table 2. Incidence (%) of root canals.
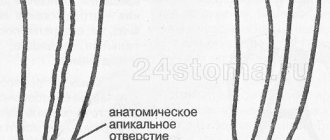
For successful endodontic treatment, it is also extremely important to know the variations in the number of root canals in order to avoid the error of missing a canal. Although back in 1921, Hess W., studying 513 teeth, indicated that four canals were found in 54% of the first molar, this fact was ignored. F. Pineda, J. Cutler (1972), studying the medial buccal roots of the first molars, found that in 39% of cases this root has one canal, in 61% - 2 canals. Later studies (J.K. Kalild and D.D. Peter, 1990) showed that in a study of 51 medial buccal roots of the upper first molars, a two-canal variant of the structure was identified in 95% of cases. Table 2 summarizes information from various authors about the frequency of occurrence of additional channels. As follows from this table, in the lower incisors, canines and premolars it is always necessary to look for the second canal, and the first upper molar should be considered a four-canal. Lower premolars can be extremely difficult teeth to treat endodontically. Two narrow canals are usually located vestibulo-orally; division into two roots can occur in the apical third. At higher magnifications, it is often possible to view more complex anatomy. The dentist’s knowledge of the anatomy of the tooth cavity and root canals is an important part of endodontic treatment, guaranteeing the success of the treatment and avoiding errors and complications.
Author: Trigolos N.N.
Material and methods
The study involved 60 patients aged 18 to 75 years who came for complaints or for examination and who had indications for primary endodontic treatment. The object of our study was the distal root canal of the first molars of the mandible. In total, 60 such teeth were studied.
The inclusion criteria for patients were as follows: men and women, Caucasian race, age from 18 to 75 years, presence of at least one mandibular molar and indication for its primary endodontic treatment.
Non-inclusion criteria: any race other than Caucasian, age under 18 or over 75 years, absence and/or previously endodontically treated mandibular first molars, presence of anchored pins and/or orthopedic structures on mandibular first molars.
After familiarizing themselves with the study design, patients signed informed voluntary consent to participate in it.
All study participants were divided into 3 groups: 1st group - young, 20 people aged 18 to 44 years; 2nd group - middle-aged people, 20 people - from 45 to 60 years old; Group 3 - elderly people, 20 people from 61 to 75 years old. To assess the anatomy of the root canals, all patients underwent an X-ray examination (CBCT) on a Vatech computer tomograph before starting endodontic treatment, and then data analysis was carried out in the Ez3D plus program. To summarize the data, a special questionnaire was developed, which reflected all the parameters we were interested in at once.
conclusions
1. According to CBCT data and a dental microscope with a magnification of up to ×40, the anatomy of the root canals of the distal root of the first lower molar directly depends on the patient’s age and changes significantly throughout life.
2. Modern cone-beam computed tomography makes it possible to obtain high-definition images of root canals with a radiation dose in the range of 1.79–3.5 mGy. In turn, visualization of the anatomical and topographical features of the structure of the root canals of teeth even at the stages of treatment planning makes it possible to determine the frequency of visits, the choice of instruments, the technique of filling root canals, as well as reduce the percentage of errors at all stages of treatment and make endodontic treatment more predictable.
The authors declare no conflict of interest.
The authors declare no conflict of interests.
Root canal treatment
Root canal treatment is most often carried out according to the following protocol.
- Anesthesia. Since the doctor works directly with the nerve, the anesthesia must be of very high quality. Until recently, preliminary devitalization of the pulp with arsenic or formaldehyde was practiced, and treatment was postponed until the next visit to the dentist. Modern medications allow you to completely relieve pain and carry out the procedure in one visit.
- Tooth isolation using a rubber dam. This is a latex membrane, thanks to which saliva does not enter the procedure area, and tooth fragments and medications do not enter the oral cavity.
- Creating convenient access to root canals. To do this, the tooth cavity opens wide.
- Cleaning and expansion of root canals. It begins with measuring the length of the canal using an x-ray or an electronic apex locator device. Next comes the turn of special endodontic instruments: these could be, for example, profiles or pro-tapers. The goals of this stage are to remove pulp tissue and infected dentin from the canal, and also to give it a cone-shaped shape convenient for filling.
- Drug treatment. No less important for canal disinfection than mechanical cleansing. The modern approach is to rinse with a large amount of solution from a syringe, which destroys microorganisms, destroys necrotic tissue, and removes dentin filings.
- Filling. Filling the root canal system with a biocompatible material to prevent its communication with both the periodontium and the dental cavity. Without this procedure, the tooth cannot be considered cured, since sooner or later it provokes periodontal inflammation. Gutta-percha (a natural analogue of rubber) in combination with paste sealants is considered the optimal filling material. A gutta-percha pin is inserted into the canal, sealed, the quality is controlled on an x-ray, and then the cavity is closed with a temporary filling or a permanent restoration is immediately installed [2, 3].
After treatment, discomfort may be felt, especially when chewing. Normally, sensitivity goes away within a few days.
Root canal manipulation is rightly considered one of the most difficult tasks in dental practice. Their high-quality processing takes considerable time and at the same time requires jewelry precision, because many dental canals are comparable in thickness to human hair. Areas close to the root apex are processed almost blindly, which means the dentist must have considerable experience and skill. That is why, for root canal treatment, you should contact a trusted clinic with highly qualified specialists.
List of sources:
- Grigoriev S. S., Sorokoumova D. V., Chernysheva N. D., Chagai A. A., Epishova A. A. Morphology of root canals. Endodontic access. Ekaterinburg: Circulation, 2022. // URL: https://dental-press.ru/ru/storage/download/42762 (access date: 09/03/2021).
- Borovsky E.V. Therapeutic dentistry: a textbook for students of medical universities. M.: Medical Information Agency, 2003. // URL: https://www.booksmed.com/stomatologiya/153-terapevticheskaya-stomatologiya-borovskij.html (access date: 09/03/2020).
- Krotova I.V. What you need to know about root canal treatment. // URL: https://medexpert.by/stati/lechenie-kornevyix-kanalov/ (date of access: 09/03/2021).
In what cases is it necessary to treat root canals?
Root canal treatment means cleaning them of pulp, followed by expansion, medicinal treatment and sealing. As a result of this procedure, the tooth loses communication with the periodontium and ceases to receive nutrients, so it is resorted to for medical reasons. These include:
- Pulpitis. An inflammatory process in the pulp, most often caused by a bacterial infection. Canal treatment is indicated when pulpitis is irreversible, that is, the pulp, even after eliminating the source of infection, is no longer able to recover.
- Periodontitis. Inflammation of the ligamentous apparatus of the tooth in the area of the root apex. Usually develops due to tooth trauma or bacterial infection that comes from the root canals.
- Cyst. A cavity in the bone near the apex of the root. It may be a complication of periodontitis or poor-quality root canal treatment, when the infection affects the bone tissue and causes it to dissolve.
- All kinds of injuries and fractures of teeth, accompanied by exposure of the pulp.
- Pulp necrosis. A consequence of a long-term inflammatory process in the absence of treatment. Represents complete tissue death.
- Prosthetics with crowns or bridges. In the second case, it is necessary to seal the canals of healthy teeth, which will become a support for the structure [2, 3].