home
Aesthetic dentistry
Dental restoration
Front teeth
Do chips, chips, gaps between teeth, a crooked or chipped tooth complicate your life and prevent you from smiling sincerely? Forget about it! Today everyone can become the owner of a beautiful smile.
Restoration of the anterior group of teeth has not been a problem for a long time, especially if you go to a good dental clinic!
Dental restoration is a procedure aimed at restoring and correcting the shape and color of enamel. The main indications for its implementation are:
- change in tooth shape;
- the presence of cracks and chips in the enamel;
- chips and gaps between teeth;
- pigmentation and darkening of the enamel that cannot be eliminated by bleaching.
The PROFI-Dent clinic offers the most affordable prices for the restoration of anterior teeth in Moscow. Our dentists, like real restoration artists, will recreate the lost tooth surface, return it to its flawless appearance, while simultaneously correcting all existing defects and imperfections.
Methods for restoring anterior teeth
There are direct and indirect methods of dental restoration:
Straight
Restoration of the anterior group of teeth has not been a problem for a long time, especially if you go to a good dental clinic!
With the direct restoration method, the dentist applies layer after layer of composite material until he has completely restored the anatomical shape of the enamel in the smallest detail. The doctor recreates not only its shape, but also its color and transparency. Such delicate work requires from a specialist not just high professionalism, but real artistic talent. These are the dentists who work at the PROFI-Dent clinic.
Indirect
This technique for restoring anterior teeth is performed using veneering, dental inlays, crowns and half-crowns, that is, structures that are pre-made in a dental laboratory using individual impressions.
Includes several stages:
- Preliminary preparation of enamel for impression taking.
- Manufacturing of dental structures.
- Fixing the finished structure to the tooth in need of correction.
The restoration method is selected by the doctor depending on the clinical case, patient preferences and the desired result.
Regardless of the restoration technique, professional hygienic cleaning and treatment (if necessary) are first carried out.
Working with the frontal zone has its own nuances and features - to achieve the best result, special materials are used that have high strength and color stability. The cost of anterior tooth restoration directly depends on the materials used and the method used.
Indirect dental restoration
The orthopedic or indirect method involves the installation of replacement structures - veneers, lumineers, inlays, crowns. Essentially, this is microprosthetics.
Crowns are installed if most of the tooth has lost its integrity, and the task is not only to improve its aesthetics, but also to provide reliable protection from further destruction. Crowns are placed on both chewing and front teeth.
Aesthetic dental restoration involves the use of veneers and lumineers.
A veneer is a thin plate with a thickness of 0.2 mm, made of ceramics, glass ceramics, zirconium or other materials.
These structures are made from a patient’s impression in the laboratory and then glued to the front of the tooth. Before installing the veneer, the top layer of enamel is ground down.
Advantages of veneers:
- High aesthetic characteristics.
- The color of the materials is resistant to dyes and changes little over time.
- Durability (subject to manufacturing technology and proper patient preparation).
Disadvantages of veneers:
- High price.
- The likelihood of increased tooth sensitivity due to filing of enamel.
- The enamel is cut down irreversibly. If the veneer falls off or there is a need to remove it, additional tooth restoration will be needed.
- Several visits to the dentist are required to install the veneer.
Lumineers are ultra-thin transparent veneers, the manufacturing technology of which is patented by the American company Cerinate.
No grinding of the enamel is required to apply them. Lumineers can be removed and replaced without damaging healthy tooth structure. However, their price is even higher than that of conventional veneers. If there is a significant change in the color of the enamel, the transparent lumineer will not be able to perform a masking function.
Restoration of anterior teeth in Moscow at the PROFI-Dent clinic
Our dental center uses only the most modern restoration methods and technologies, which allow you to quickly and efficiently restore the anatomical, aesthetic and functional components of the front teeth, ensuring an impeccable appearance and a beautiful, natural smile.
The main advantages of aesthetic restoration with us:
- the opportunity to restore a gorgeous smile in just one visit to the dentist;
- latest generation materials;
- long-term result;
- the most affordable prices for front tooth restoration in Moscow.
We can correct your front teeth, change their shape, length, position, and eliminate enamel defects quickly and efficiently. To be confident in the final result, our specialists carefully monitor every stage of work, following the highest international quality standards, and use only advanced materials and restoration technologies.
Methods
The process of restoring the front teeth is carried out using one of the existing methods, which is selected individually by a specialist. The composite material is fixed directly into the cavity or an inlay is first made, which is then attached to an adhesive composition:
- direct reconstruction involves applying a filling compound to the prepared area in accordance with the technology and rules for using the selected material;
- indirect restoration involves the use of inlays, which are made outside the patient’s mouth in a laboratory setting. Fixation is carried out in the damaged area using special cement.
In order to determine the most suitable restoration method, the specialist assesses the extent of the damaged area, the bite and other characteristics of the patient. Without a preliminary examination and elimination of the consequences of caries or other types of lesions, no specialist will choose a method and material. Errors made at the preparatory stage negatively affect the service life of fillings and inserts, so there is no need to speed up the restoration process. In addition, they are incredibly durable, subject to a tiny percentage of abrasion, and have low polymerization shrinkage.
How much does it cost to restore front teeth?
Our clinic values its patients, so we carefully plan our pricing policy. You will be pleasantly surprised not only by the highest quality of dental services. The price of restoration of anterior teeth in PROFI-Dent dentistry is in the budget range.
| Price list for dental | |
| Consultation with a dentist-therapist | FOR FREE |
| Restoration of wedge-shaped defect, enamel erosion | from 3,000 rubles |
| Restoration of the frontal group | from 5,000 rubles |
| Artistic restoration made from light-curing material | from 5,000 rubles |
| Ceramic-composite veneer | from 8,000 rubles |
| Installation of dental jewelry | 1,000 rubles |
Restoration of non-carious lesions of anterior teeth
Teeth with non-carious signs of damage also require restoration:
- enamel hypoplasia/hyperplasia;
- endemic fluorosis;
- various anomalies;
- hereditary factor;
- lesions resulting from eruption (trauma, erosion, surface and location defects, etc.);
- integrity of dental tissue;
- the extent of the outbreak;
- intensity of tissue breakdown;
- allergic reaction of the patient materials and drugs.
Just 15 years ago, dental defects due to non-carious lesions were solved by installing crowns. Now you can use both filling material and composite reflective material. If there is a slight curvature, wearing braces is no longer necessary; the problem can be eliminated in other ways.
Frontal prosthetics: implantation
Prosthetics of the frontal area of the upper jaw using dental implants is the most complex procedure in modern dentistry, and not only because it requires a certain level of knowledge and skills from a surgeon and orthopedist. To a greater extent, this is due to the increased aesthetic expectations of the patient, who is not ready to put up with even minimal visual discomfort, which would indicate the presence of something unnatural in the oral cavity (according to the authors’ observation, even with a low smile line).
Today, absolutely all patients of our clinic are extremely demanding about the results of prosthetics on implants in the frontal area.
This is largely due to the increased amount of information that our patients receive via the Internet, from various forums and simply publications. In some cases, such information is, unfortunately, far-fetched, since some dentists make “mystical” conclusions, refusing the opportunity to learn from the experience of recognized masters, whose books are no longer in short supply in Russia.
The purpose of this publication is to confirm those common truths, without which prosthetics on implants in aesthetically significant areas is simply unthinkable.
Preparation for implantation. Planning.
Planning of the entire treatment begins with communication between the orthopedic surgeon and the dental technician as the main team players with the patient, where the main attention is paid not to the possible development of the situation during implantation or subsequent prosthetics, but to the following factors:
- patient expectations,
- smoking,
- smile line height,
- gum biotype,
- the shape of the remaining or restored teeth,
- infection in the area of upcoming implantation,
- orthopedic status of the teeth adjacent to the defect area, type of dentition defect,
- width of bone and soft tissue in the edentulous area,
- height of bone and soft tissue in the edentulous area.
After detailing the patient’s specific wishes, the orthopedic doctor is obliged to confirm or deny the possibility of obtaining the requested result.
Alas, it is worth recognizing that in most cases such communication is absent, and there is only one reason - to earn money at any cost and install an implant as soon as possible after the first request. However, after a long and unsuccessful treatment, a fiasco often sets in for both the doctor and the unfortunate patient!
Implantation can be immediate after tooth extraction, or delayed, no less than two months later - as a rule, after tooth extraction in case of acute or exacerbated chronic infectious inflammation. Let's look at a number of proven rules that will allow us to talk about successful surgical treatment.
Tooth extraction and immediate implantation
The basic rule that a surgeon should never violate is atraumatic removal, which will allow preserving the alveolar vestibular wall and installing an implant. In this regard, elevators and forceps cannot be used without first fragmenting the tooth with cutters and working with periotomes.
After the tooth is removed, the doctor needs to make sure, through simple probing, that the anterior wall of the alveoli is intact - in the case of obvious and pronounced fenestrated defects, implantation is impossible.
When installing an implant, you must remember that the use of implant diameters of more than 4.5 mm is highly recommended! The judgment of some Russian surgeons is erroneous that if the size of the socket allows the installation of implants up to or more than 5 mm, then this is justified by the ideal primary stabilization of the implant. However, in the foreseeable future, contact of the implant to the vestibular wall of the alveolus, even in the upper third of the socket, will lead to resorption of the wall, which in turn will cause an unsatisfactory aesthetic result.
Primary stabilization of the implant is probably the main factor influencing the positive outcome of the entire treatment, but it is unacceptable to achieve it by bicortical wedging of the implant in the socket of the extracted tooth. All that needs to be done is to deepen the hole by at least 3-4 mm and shift the axis of the implant palatally so that there is no contact with the anterior wall of the alveolus along its entire length (Fig. 2).
The distance between the implant and the anterior wall should be between 1.5 and 2 mm. If this distance exceeds the specified value, then we recommend using autogenous bone mixed in equal proportions with the Bio-Oss material, since the latter will act as a scaffold to support the autogenous bone.
The flap is folded back, it is planned to remove 11 and 21 with simultaneous implantation (Fig. 3).
Teeth 11 and 21 were removed (Fig. 4).
Biohorizon implants with a diameter of 3.8 were installed (Fig. 5).
A correctly made template allows you to position not only the axis, but also the location of the implant neck (Fig. 6).
The position of the implants shifted in the palatal direction is clearly visible in Fig. 7.
Autogenous bone from the mandibular ramus is mixed with Bio-Oss and tightly condensed between the implant and the alveolus (Fig. 8-10).
Temporary prosthetics with immediate implantation
Temporary prosthetics using a fixed structure, such as screw-retained crowns to achieve an aesthetic result and social rehabilitation of the patient, is only possible with good fixation of the implant. If there is the slightest doubt about this, as well as during NTR, we recommend suturing the implant and fixing the Maryland structure.
Temporary implant prosthetics can be performed with cement or screw fixation, when a temporary plastic abutment acts as the core of the crown, onto which the technician presses acrylic material (Fig. 11).
Personally, I do not recommend making cement-retained temporary crowns on temporary abutments that have not been customized to the gingival contour. They have nothing to do with the anatomy of the operated area, since the unpredictability of the degree of immersion of the crown edge towards the implant neck and, as a consequence, the release of temporary cement in close proximity to the latter, can lead to the occurrence of peri-implantitis.
Screw fixation
Screw-retained crowns can be made either directly by the doctor in the clinic during the patient’s appointment, or in the laboratory.
The ability to use the direct method is a necessary tool in the orthopedic arsenal, which can be used either due to the distance of the laboratory from the clinic, or in the event of unexpected removal and installation of an implant, and the inability to release the patient without a temporary restoration.
The advantages of the direct method over the laboratory method include the ability to control the necessary support of soft tissues in the cervical area, low cost, and timing.
The disadvantages are not very high or even low aesthetics.
It should be noted that using the screw fixation method should not be done with caution. The number of unscrewing and screwing of such crowns should be limited, especially with a thin gum biotype, since (especially on poorly polished structures) large recessions are possible due to the resulting false attachment and constant trauma.
The laboratory method involves taking an impression and, after receiving a plaster model from the laboratory, remodeling the gingival margin according to the required aesthetic contour (see laboratory method below). After the acrylic crowns are ready, the doctor performs anesthesia in the area of the implants and screws them until gum ischemia occurs (RVG control is required).
It is important to remember that this design should only apply pressure to soft tissue. In the case of such pressure on the underlying bone, a powerful pain syndrome always develops with prolonged inflammation and, as a consequence, serious recession (Fig. 12-13).
The remodeling of tissues in the oral cavity takes from 4 to 6 weeks and, with a sufficient amount of attached gum, always demonstrates a 100% result, which consists of a perfect imitation of the natural gingival margin. However, if prosthetics of teeth adjacent to implants is also planned, the dentist must remember that without immersing the ledge under the gingival area from the proximal sides at the border with the implants, he risks losing the gingival papilla due to the lack of its support.
To illustrate these theoretical constructs, let me give a small example.
Clinical case
Patient 29 years old, 11 – fracture in the lower third.
After a detailed analysis of the situation in the presence of a dental technician (Dmitry Nikonenko), a decision was made to remove 11 with the immediate installation of an implant, a temporary crown with screw fixation and prosthetics of 4 incisors after 6 months.
After this period, we began endodontic treatment 21 and the production of a core inlay. It was decided to make an individual abutment and two crowns on zirconium dioxide frames for teeth 11 and 21, and for vital teeth 12 and 22 - frameless crowns with a thickness of no more than 0.5 mm! (Fig. 14-17).
Despite the excellent epithelialization, before fixing the crowns, it is necessary to place an unimpregnated retraction cord with a diameter of no more than 000 or 00 between the abutment, teeth and gum to capture excess cement.
Using the positioner in RVG, you can see the facts of “under-fitting” of the crown frame on the abutment or teeth! Pay attention to the distorted image 17a, where it may seem to an inexperienced doctor that the position of the crown on the abutment is ideal, but with the correct positioning of the positioner, a gap is visible in the medial-proximal zone of the crown on the 11th tooth.
Rice. 18 – crowns fixed with self-etching and self-adhesive cement after 7 days.
The situation after three months is shown in Fig. 19.
After a year the situation looks like this - Fig. 20.
Neither the dentist, nor the technician, nor the patient has any complaints about the work performed. But this is the frontal zone...
Author:
Ordzhonikidze G.Z., orthopedic dentist (Moscow)
Contraindications
If the patient has periodontitis, caries, bruxism, a small amount of enamel on the teeth, as well as in the case of some occlusion pathologies, insufficiently erupted teeth, it is first necessary to eliminate the existing pathology, and then carry out aesthetic restoration. At the same time, contraindications include malignant tumors during radiation or chemical therapy and some time after its completion, diseases of the skeletal system that reduce its regenerative capabilities, diseases of the circulatory system that impair blood clotting, serious diseases of the heart, central nervous and immune systems, intolerance anesthesia, mental disorders in the acute stage.
Teeth whitening
Changing the color of teeth is associated with the abrasion of the snow-white enamel, under which there is dentin - dental tissue that has a yellowish tint. Another reason is exposure of teeth to dyes (foods or medications). Mostly people with naturally dark teeth apply.
Teeth Lightening and Whitening: What's the Difference?
Lightening involves the use of gentle techniques to return teeth to their natural shade. This can be achieved, for example, with the help of professional cleaning AIR FLOW, aimed at eliminating plaque and tartar. Whitening – lightening the natural color of teeth by several shades.
Which method of professional teeth whitening is the most gentle?
The latest comprehensive teeth whitening system, ZOOM, is very popular, which allows you to achieve a snow-white smile without damaging tooth enamel. The method involves the use of a special gel, the action of which is activated by a lamp. At the end of the procedure, the teeth are treated with fluoride. Whitening lasts on average about one and a half hours, and the result is a change in the shade of teeth by an average of 8 tones.
How to whiten teeth at home?
The most effective is professional home teeth whitening using trays and gel, which is controlled by the dentist. Mouthguards (plates) are made from a dental impression. They are filled with gel and worn for several hours (usually overnight) for 2 – 3 weeks.
How harmful is professional whitening to teeth?
Most modern professional systems do not contain acids. Special technologies and materials (gels) do not act on tooth enamel, but on the pigment itself, which is then removed. If the gel contains hydrogen peroxide, then before teeth whitening it is recommended to carry out fluoridation, which helps strengthen the enamel. For whitening to be safe, the procedure must be performed by an experienced, qualified dentist.
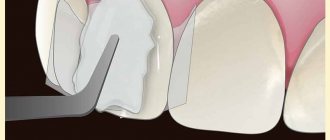
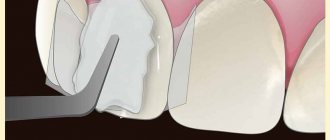
Stages of restoration with ceramic veneers
- Preparatory. The dentist performs the procedure of taking an impression of the existing dentition.
- Based on the bite, a technician in the laboratory creates a plastic model of future teeth, which is tried on the patient.
- If the patient is satisfied with the appearance of the teeth and the way they fit in the mouth, the technician makes ceramic veneers.
- Then, after grinding the patient’s teeth, the veneers are permanently bonded to the surface of the teeth.
After installation of veneers, there is no expected recovery period. The first few days the patient may feel slight discomfort due to the pads, but this quickly passes. A prerequisite for patients with veneers is regular oral hygiene and preventive examinations by the dentist.