1615
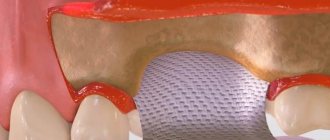
Barrier membranes are a modern surgical thin-sheet material designed to isolate surgical wounds filled with bone substitute for guided osteoregeneration.
Membranes are used to increase the efficiency of bone regeneration, accelerate wound healing, and eliminate bone resorption and postoperative complications.
Barrier films are used in dental surgery for various types of bone grafting, flap periodontal surgery, surgical correction of maxillodental anomalies, etc.
General overview
The American company Osteogenics Biomedical produces barrier membranes of various characteristics from natural and artificial materials.
Resorbable materials are made from natural raw materials - cattle tendons and porcine collagen.
The starting material for non-resorbable membranes is polytetrafluoroethylene. PTFE material can have a non-textured or textured surface, or be modified (hardened) with titanium.
Osteogenics Biomedical Barrier Membranes
| Resorbable | Size, mm | Non-resorbable | |||||
| Untextured | Size, mm | Microtextured | Size, mm | Titanium Reinforced | Size, mm | ||
| Cytoplast RTM Collagen | 30x40, 20x30, 15x20. | Cytoplast GBR-200 Singles | 12x24 | Cytoplast TXT-200 Singles | 12x24 | Cytoplast TI-250 ANTERIOR | 14x24, 12x24 |
| Cytoplast GBR-200 | 25x30 | Cytoplast TXT-200 | 25x30 | Cytoplast TI-250 BUCCAL | 17x25 | ||
| Cytoplast TI-250 POSTERIOR | 25x30, 20x25 | ||||||
| Cytoplast TI-250 XL | 30x40 | ||||||
Non-resorbable polytetrafluoroethylene (PTFE) dental membrane is an exclusive product not produced by anyone else other than Osteogenics Biomedical.
The material is intended for targeted regeneration of bone and gum tissue during surgical operations in dentistry.
Among the main purposes of Cytoplast GBR-200:
- providing primary wound coverage;
- preventing bone resorption;
- stimulating the growth of bone tissue from osteosubstitute;
- protecting the wound from pathogens;
- acceleration of wound healing;
- simplifying the work of surgeons.
Correction of malocclusions using Vector Tas microimplants and features of their use.
Come here if you are interested in the characteristics and purpose of Bio Oss bone material.
At this address https://www.vash-dentist.ru/implantatsiya/metodiki/temperaturyi-posle-zubov.html find out how long the temperature lasts after dental implantation with a positive outcome of the operation, and what indicators indicate the need to see a doctor.
More information about Cytoplast membranes
Titanium reinforced membranes
Advantages • Titanium frame increases rigidity and ensures that the desired shape is created and maintained • Since soft tissue does not grow through the membrane, removal is much easier than titanium mesh • Since bacteria 2-5 microns in diameter cannot penetrate the membrane, the membrane can be left exposed in throughout the entire healing period
The Cytoplast line contains non-resorbable high-density Ti-250 membranes. This textured membrane, made from titanium-reinforced polytetrafluoroethylene (PTFE), features a patented Regentex surface that helps withstand potential membrane exposures by stabilizing both the membrane and the flap. The edges of the membrane are covered with soft tissues 360°. The Regentex surface also allows for increased cell attachment surface area, promotes better membrane stabilization and prevents soft tissue retraction. The titanium part of the reinforced membranes is plastic - this makes it easier to position the membrane in the defect area. If there is a lack of structural support during horizontal and vertical augmentation of the alveolar process in the socket of an extracted tooth, the installation of temporary membranes is often necessary to prevent the socket from collapsing. Titanium frame-reinforced Cytoplast membranes are based on the latest manufacturing technology, have specific dimensions for the specific application site, and have a Regentex surface required for bacteria. Using Cytoplast membranes for transplantation, you will certainly reach new heights.
Dimensions of “titanium membranes” Ti-250: ANTERIOR narrow 12x20mm - suitable for use after the extraction of one tooth, especially if one or more bone walls of the alveoli are missing. ANTERIOR single 14x24mm is the ideal size and shape of a post-extraction defect when removing one tooth, especially in the absence of alveolar walls. BUCCAL 17x25mm - intended for implantation in case of significant defects of the buccal wall. POSTERIOR single 20x25mm - designed and ideal for shaping the desired shape of the alveolar process. POSTERIOR large 25x30mm - intended for large bone defects. XL 30x40mm - designed for very large defects, especially alveolar bone augmentation.
Microtextured membranes
Advantages • Minimum soft tissue detachment • Reduced surgical time because the membrane can remain exposed • Preservation of the soft tissue architecture, interdental papillae of the keratinizing mucosa • After bone formation under the membrane, secondary epithelium begins to grow • Easy non-surgical removal without re-operation and anesthesia
The Cytoplast line contains non-resorbable microtextured membranes TXT-200. This is a temporarily implanted material (non-absorbable) for use as a space barrier in the treatment of periodontal defects. The textured membrane consists of dense micro-textured PTFE with pores smaller than 0.3 microns. The textured surface with hexagonal indentations increases the area of fastening of fabrics.
Dimensions of “microtextured membranes” TXT-200: Singles PTFE 12x24mm - used for single tooth extraction. For large defects and areas where primary wound closure is not possible due to insufficient flap. PTFE 25x30mm is the ideal size and shape of a post-extraction defect when removing one tooth, especially in the absence of alveolar walls.
Main characteristics
Cytoplast Regentex GBR 200 material is a dense polymer film 0.2 mm thick with a smooth surface.
The latter feature is a significant advantage over traditional resorbable membranes, the surface of which promotes retention and invasion by bacteria, causing rejection of the covering material and inflammation of the wound.
The smooth surface of GBR-200 “repels” pathogenic microorganisms, preventing infection and inflammation of the operating area.
The Cytoplast Regentex membrane has a microporous structure with a pore size of up to 1.26 microns, which does not allow bacteria to pass through the film, but at the same time is permeable to proteins.
The plastic-elastic consistency of the material allows it to be stretched and deformed, giving it the desired shape to adapt to the operating area.
Cytoplast has self-adhesive properties to the wound surface. As an additional measure of fixation, suturing the edges of the flap laid over Cytoplast can be used with light, tension-free sutures that do not affect the membrane itself.
The material comes in standard sizes 12x24 mm and 25x30 mm . From these blanks you can cut pieces of any size required in a specific clinical situation with scissors.
Suture material
Cytoplast PTFE suture material is an ideal tool for bone grafting and implant procedures. The soft monofilaments prevent bacteria from entering the surgical site, unlike most suture materials, and patients appreciate the softness of Osteogenics sutures.
| Name | vendor code | Price |
| Suture material PTFE Prem/Perio | CS0618 Prem/Perio | 190 $ |
| Suture material PTFE USP 2-0 | CS0418 | 150 $ |
| Suture material PTFE USP 3-0 | CS0518 | 150 $ |
| Suture material PTFE USP 4-0 | CS0618 | 150 $ |
Osteogenics Biomedical's Cytoplast products are guaranteed to meet and exceed national and international regulatory standards. Cytoplast production is certified and has been inspected by authorities such as the FDA.
Download: ISO 13485:2003/13485:2012 QMS-MD / ISO 13485:2003 CMDCAS (Canada) / ISO 9001 QMS / MDD/93/42/EEC (European Union - CE Mark) / ISO Class 7.
| Cytoplast Product Knowledge Base |
| Augmentation of the alveolar process simultaneously with implantation with Cytoplast Ti-250 XL membrane |
| Instructions for use of Cytoplast Regentex GBR-200 membrane |
| Instructions for use of Cytoplast Regentex TXT-200 membrane |
| Non-resorbable Barrier Membrane for maxillofacial surgery and implantology Cytoplast Regentex GBR 200 |
| Reconstruction of the alveolar process with a buccal wall defect |
Composition and properties
The GBR-200 membrane consists of one PTFE (polytetrafluoroethylene (Teflon)) - a fluorocarbon compound that is resistant to almost any aggressive chemical agents.
Under human body conditions, PTFE is absolutely insoluble in substances and physiological fluids.
Physico-chemical and biological properties:
- chemical stability;
- extremely low allergenicity;
- self-adhesiveness to the wound;
- gas and light tightness;
- impermeability to bacteria;
- permeability to proteins.
Prices for treatment of epiretinal membrane of the retina
| Surgical removal of the epiretinal membrane (difficulty category 1) | 35,000 rubles |
| Surgical removal of the epiretinal membrane (difficulty category 1) | 53,000 rubles |
| Surgical removal of the epiretinal membrane (difficulty category 1) | 69,000 rubles |
ATTENTION! The exact cost of treatment can only be determined after an in-person consultation, when the condition of the patient’s retina has been determined, a treatment plan has been drawn up, and the need for general anesthesia has been determined. You can find out the cost of basic procedures and operations in the PRICES section.
Advantages and disadvantages
Cytoplast has a number of clinical and technological advantages compared to traditional suture materials, making it very popular among dental surgeons.
Advantages
- There is no need for primary flap closure of the wound fragment (no need to prepare and stretch the flap material).
- Non-germination of epithelium , due to the high barrier properties of the material.
- Elasticity (the membrane stretches in any direction, adapting to the wound).
- Stability of the structure (does not swell).
- There is no need to cover the membrane with anything from above , the film can remain completely exposed. To completely close the wound area, one Cytoplast GBR-200 is sufficient.
- Self-adhesive to the wound due to its special microstructure. There is no need to use complex fixing elements to attach the film to the bone; the edges of the wound do not need to be sutured.
- The absence of any negative consequences and chemical reactions when the material comes into contact with intraoral fluid.
- Fast wound healing.
- Preservation of the shape of the augmented alveolar bone tissue.
- Easy non-surgical removal of the membrane from the wound in 21-25 days. Removal is done through a small hole using a probe.
- Complete absence of any complications.
Flaws
Numerous tests have not revealed any significant drawbacks, which are often observed when using other types of membranes.
No rejection, inflammation, proliferation or other tissue reactions that negatively affected the healing process were noted.
The only drawback is the need for a dental surgeon to have practical skill in using the material , for which he has to undergo preliminary training.
Surgical membranes are most widely used in dental implantation.
Let us recall that the “classical” implantation method involves two stages: implantation and the subsequent orthopedic part of the planned treatment (that is, installation of a prosthesis on an established implant). Since usually a fairly long period passes after the loss of a tooth and before the operation to implant an artificial root, work directly with the implant is preceded by an operation to restore the required volume of bone (osteoplasty), due to the fact that bone tissue atrophy is observed.
When performing such operations, the doctor uses either fragments of the patient’s own bone tissue (plantation of bone blocks) or materials/preparations that promote bone growth. In both cases, the surgeon can use a membrane (bone blocks can be secured with titanium screws; for fixation of osteoplastic material, the use of a membrane is advisable and is determined by the physical properties of the material). In this case, the membrane performs a kind of reinforcing function: it holds the osteoplastic material in the required correct position. As a reinforcing agent, the membrane can also be used during implantation with simultaneous replanting of osteoplastic material. The membrane can be attached to the bone or to the teeth adjacent to the intervention site.
Indications
The GBR-200 membrane is recommended for use in dentistry in all cases associated with directed bone regeneration:
- After tooth extraction to restore the bone tissue of the alveolar process.
- Before installing an implant if the bone volume is small.
- During or after installation of the implant - to close the wound.
- For augmentation in a wide variety of clinical cases.
- For peri-implantitis (inflammation of bone and soft tissues adjacent to the implant, their resorption and loss of the implant).
- For flap operations in the oral cavity, plastic surgery and gum recession.
- When restoring jaw proportions (for example, with a planar osteotomy, accompanied by replanting of bone tissue between separated fragments of the jaw bones).
- During sinus lifting (Cytoplast is placed on the bottom of the maxillary sinus to eliminate the risk of penetration of the osteosubstitute into the sinus through perforations in the mucous membrane).
Let's discuss together the pros and cons of dental implantation in comparison with other prosthetic methods.
In this publication we will tell you whether you need to take antibiotics after dental implantation and why.
Follow the link https://www.vash-dentist.ru/implantatsiya/metodiki/rashozhdeniya-shvov-posle-zubov.html to find out when the sutures are removed after dental implantation.
Bone grafting is a solution to the problem of atrophy
For quite a long time, bone grafting has been recognized as the most effective method of restoring the width and height of the alveolar process. The technique is constantly modified and becomes safer and less traumatic. In addition, dentists are trying to achieve conditions under which simultaneous implantation will be possible.
There are several basic bone grafting techniques:
- Sinus lift. Restoration of bone volume in the upper jaw in the area of the projection of the bottom of the maxillary sinus. The operation is performed more often than others, since it is here that bone resorption is predominantly observed. The essence of the surgical intervention is that the dentist, in one of the ways (closed or open), gains access to the mucous membrane of the maxillary sinus. He disconnects part of the membrane from the periosteum, and fills the resulting cavity with prepared material of natural or synthetic origin.
- Splitting of the alveolar ridge. An effective technique for correcting the width of any jaw. First, the alveolar ridge is cut and spread apart, after which the graft is placed inside. The advantage of the technique is that the structure is immersed in the spongy tissue of the jaw, where regeneration and replenishment of the bone block is actively taking place. That is why the use of expensive osteoplastic materials is not required here.
- Guided tissue regeneration. This type of bone grafting includes two components: a graft and a collagen membrane. These two components, interacting with each other, help restore the deficit of both the width and height of the alveolar process in any part of the jaws. The technique is rarely used with simultaneous implantation.
- Bone block grafting. This technique involves the use of a natural, preferably autogenous, graft, which is placed on the area where implantation is planned and where the bone tissue has atrophied. The disadvantage of this technique is that the graft is connected to an area of the bone where there are no blood vessels. Engraftment in such conditions occurs slowly.
Patients tend to be afraid of bone grafting, since it is a full-fledged surgical intervention on the teeth. However, all manipulations are carried out under local or general anesthesia, so they do not cause any discomfort. The risk of complications with this manipulation is minimal, and the benefits are undeniable. Even if the atrophy of the alveolar process does not allow immediate implantation, and patients have to wait six months for the implants to take root, it is still better to give preference to bone grafting rather than alternative methods of tooth restoration. Moreover, in modern conditions there are many designs that increase the benefit and effectiveness of bone grafting, for example, fixation of a barrier membrane.
Technique of use
After filling the surgical wound with a bone substitute, Cytoplast GBR-200 is placed on top of it, overlapping the edges of the wound by 2-3 mm. In addition to self-adhesiveness, the film can be fixed to the wound using light, tension-free suturing of flaps placed on top of the Cytoplast.
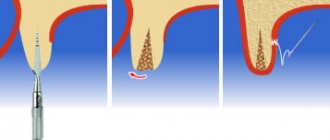
The membrane is removed 21-25 days after the operation. The deadline is 28 days. Repeated surgery to remove Cytoplast is not required.
If a flap has been placed and sutured over the membrane, the material is extracted (pulled out) using a probe through a small hole . In most cases, anesthesia is not required (in extreme cases, topical anesthesia is used), bleeding, as a rule, does not occur.
After covering the surgical wound under the Cytoplast, bone and secondary epithelium begin to quickly form. Fusion of the flap with the newly formed epithelium usually occurs a month and a half after the operation.
In the video, watch the technique of using the Cytoplast membrane.
Causes
An epiretinal membrane can develop in humans against the background of certain ophthalmological diseases. Such diseases include:
- Diabetic retinopathy;
- Retinal tear;
- Vitreous detachment;
- Retinal vein thrombosis.
This process can be activated by hemorrhages and inflammatory processes in the eye. True, in most cases, the epiretinal membrane is an idiopathic phenomenon, the origin of which remains unclear. It is known that it contains retinal pigment epithelial cells, fragments of the vitreous body, collagen, as well as fibrocytes and macrophages and macrophages.
Clinical results
In order to determine the effectiveness of the GBR-200 membrane, the developer conducted studies of the material on a group of 10 patients in 3 clinical cases:
- tooth extraction;
- tooth extraction with implantation of a bone substitute;
- tooth extraction with implantation.
The following conditions for the operation were provided:
- the membrane was cut out using scissors according to the shape of the defect;
- when applied, the membrane overlapped the hole by 2-3 mm;
- adherence of the material to the wound was ensured by stretching and pressing with fingers and an instrument, taking into account the configuration of the alveolar process;
- The cytoplast remained on the wound for 21 days, after which it was carefully pulled off with tweezers.
Research results
- In no case of use of the GBR-200 material did an inflammatory process, cell proliferation or other negative tissue reactions occur.
- None of the membranes were rejected.
- All films were easily removed from the wound after 21 days without the use of anesthesia.
- On the wound surface, which was under the membrane, there was no resorption of surrounding tissues or epithelial growth. Only in some places along the edges of the wound were there migrating small areas of epithelium.
- The wound surface after removal of the Cytoplast was a newly formed bone structure.
Based on the results of the study, it was concluded that when Cytoplast GBR-200 was used for 3 weeks, a reliable barrier was created on the surface of the wound, which prevented the germination of epithelial tissue.
Installation of a barrier membrane in the DentalPRO dental clinic
Branches of our dental clinic “DentalPRO” are located in different districts of Moscow. Make an appointment with a dentist by phone. If you need professional advice, order it with just one call to our clinic. We work from 10:00 to 21:00 seven days a week and will call you back as soon as possible.
Our specialist will answer all your questions and provide full information about installing a barrier membrane at the DentalPRO clinic. We use advanced materials and practice the most modern methods of dental treatment. By contacting our dental clinic, you can count on effective and painless membrane installation for dental implantation at a price that is affordable to everyone. If you don’t have toothache, make an appointment with a dentist at our DentalPRO clinic right now!
Reviews
The use of barrier membranes during surgical interventions is a new, modern technology that has not yet received the distribution it deserves.
If you have undergone surgery using Cytoplast barrier membranes, share your impressions of this material with other visitors to our site, leave your comment at the bottom of the page.
If you find an error, please select a piece of text and press Ctrl+Enter.
Tags: implantation, implantation methods
Did you like the article? stay tuned
Previous article
Should I save or remove a tooth in case of purulent periodontitis?
Next article
Universal trainer I-3 for the correction of malocclusions in children
How to install a barrier membrane?
The innovative method of using a barrier membrane requires certain experience from the dentist, as well as clear knowledge of the technique of performing the stage. The structure is fixed as follows:
- Performing local or general anesthesia with the addition of sedatives (the last point is not always necessary);
- An incision in the outer soft tissues of the gums and moving them away from the bone of the alveolar process;
- Replenishment of the required amount of bone tissue using one of the previously selected methods;
- Fixing a modern structure made of collagen or metal with special titanium screws to adjacent teeth or to the jaw bone itself;
- Repositioning the soft gum tissue and securing it with surgical sutures.
When using a membrane that does not dissolve, after a certain time almost all steps are repeated to remove the structure.
A prerequisite for the patient’s successful recovery is careful oral care in the postoperative period. A person must maintain personal oral hygiene and follow all recommendations of the dentist. It is also important to quit smoking a few days before surgery and for the entire rehabilitation period.