CHEWING MUSCLES
- a group of muscles, the contraction of which moves the lower jaw in directions that ensure chewing.
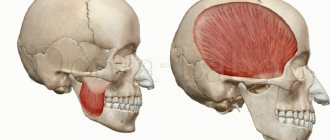
Topographically, this group of muscles includes some muscles of the head (masseter proper, temporalis, lateral and medial pterygoid muscles - Fig. 1) and neck muscles located above the hyoid bone (mylohyoid, geniohyoid and digastric muscles). Rice. 1. Chewing muscles: a - temporal and chewing muscles; b - pterygoid muscles; 1 - temporal muscle; 2 - the masticatory muscle itself: 3 - the lateral pterygoid muscle; 4 - medial pterygoid muscle; 5 - pterygomandibular suture; 6 - buccal muscle.
Anatomy
The masseter muscle itself
(m. masseter) lies on the outer surface of the branch of the lower jaw; consists of three parts: superficial, intermediate and deep. The superficial part (pars superficialis) begins with a tendon from the lower edge and inner surface of the zygomatic arch, goes down and attaches to the masticatory tuberosity of the lower jaw. The intermediate part (pars intermedia) starts from the inner surface of the zygomatic arch and from the anterior slope of the articular tubercle of the temporal bone, goes down and back, attaching to the outer surface of the branch of the lower jaw. The deep part (pars profunda) starts from the inner surface of the zygomatic arch and bone, attaching to the tendon of the temporal muscle. Function of the masticatory muscle: the superficial part pushes the lower jaw forward, the intermediate and deep part lift it.
Temporalis muscle
(m. temporalis) lies in the temporal fossa, fan-shaped starting from the platform of the bone, from the temporal surface of the greater wing and the infratemporal crest of the sphenoid bone, from the parietal, scales of the frontal and temporal surface of the zygomatic bones and is attached by a powerful tendon to the coronoid process and branches of the lower jaw in the area mandibular notch and oblique line. Function of the temporal muscle: the anterior and middle bundles lift the lower jaw, the posterior bundles pull it back.
Lateral pterygoid muscle
(m. pterygoideus lat.) triangular in shape lies in the infratemporal fossa. It starts with two heads: upper and lower. The superior head starts from the infratemporal surface and the infratemporal crest of the greater wing of the sphenoid bone, goes backward, attaching to the articular capsule and articular disc of the temporomandibular joint. The lower head starts from the outer surface of the pterygoid process of the sphenoid bone, goes back and up, connects with the upper head and attaches to the pterygoid fossa on the neck of the lower jaw. Its function: with bilateral contraction, it pushes the lower jaw forward, with unilateral contraction, it shifts it to the opposite side.
Medial pterygoid muscle
(m. pterygoideus med.) quadrangular in shape lies on the inner surface of the ramus of the lower jaw. It begins with tendon and muscle fibers from the pterygoid fossa of the pterygoid process of the sphenoid bone, goes back and down, attaching to the pterygoid tuberosity of the lower jaw. Function: with bilateral contraction, it raises the lower jaw, with unilateral contraction, it moves it to the opposite side.
Mylohyoid muscle
(m. mylohyoideus) flat, trapezoidal in shape. It begins on the inner surface of the lower jaw along the mylohyoid line. The muscle fibers are directed from top to bottom, from outside to inside and from front to back to the midline, where they form a tendon suture. Attaches to the body of the hyoid bone.
Geniohyoid muscle
(m. geniohyoideus) triangular in shape; starts from the mental spine of the lower jaw, goes down and backward, attaching to the body of the hyoid bone.
Digastric
(m. digastricus) has two abdomens: the posterior (venter post.) begins from the mastoid notch of the temporal bone and the anterior (venter ant.) - from the digastric fossa of the mandible; they unite into one intermediate tendon, which is attached to the greater horn of the hyoid bone. The function of the mylohyoid, geniohyoid and anterior belly of the digastric muscles is that when the hyoid bone is fixed, they lower the lower jaw.
Depending on the function, the stomach m., providing chewing (see), can be divided into three groups: lifters, protractors and lowerers. The levators include the masticatory, temporal and pterygoid muscles themselves, the protractors include the lateral pterygoid, and the depressors include the mylohyoid, geniohyoid and digastric muscles. Blood supply - from the branches of the infratemporal part of the maxillary artery, branches of the facial and lingual arteries.
Innervation of the masticatory muscles
occurs due to the third branch of the trigeminal nerve (n. mandibularis) and the facial nerve (n. facialis)
Anatomy of the masticatory muscles:
I. Temporal muscle (musculus temporalis)
The largest and most visible muscle of mastication. Unlike all other chewing muscles, its abdomen is located on the cranial vault (fornix cranii).
In green I highlighted the outline of the temporal muscle itself, in blue - the outline of the powerful tendon with which the muscle is attached to the coronoid process (processus coronoideus) of the lower jaw. I outlined the coronoid process in yellow, I hope you remember it from craniology. When you show the location of the temporal muscle during the test, you should outline the entire contour, that is, both the muscle and its tendon.
The temporal muscle is located in the temporal fossa (fossa temporalis). If you take a dissected skull, or even a high-quality artificial specimen, you will see impressions on the sides. These impressions are shallow, but occupy a large area. It is these depressions that are called the temporal fossae. In the picture from Wikipedia, the temporal fossa is highlighted with a black frame:
Origin: The temporalis muscle begins on the temporal surface of the frontal bone, as well as on the squamous surface of the temporal bone.
Attachment: The temporalis muscle attaches to the coronoid process of the mandible (the sharpest process of the mandible). Don't forget that the chewing muscles start from the stationary part and are attached to the bone that they move.
Function: the temporalis muscle closes the mouth, raising the lower jaw until the teeth are closed. Also, if you push your lower jaw forward, like a drawer in a table, it is the temporalis muscle that will push it back to its normal position.
II. Chewing muscle (musculus masseter)
It is also a very noticeable and large muscle. If we look at a tablet with an image in profile, it is impossible to confuse the masticatory muscle with anything else. See:
The chewing muscle is extremely important for survival, so our distant ancestors developed this muscle to be very powerful and strong. The masticatory muscle consists of two parts - superficial (pars superficialis) and deep (pars profunda). You can easily distinguish the superficial part - it is attached to the anterior part of the zygomatic arch (arcus zygomaticus). The deep part is also attached to the zygomatic arch, only not in front, but in the back.
I highlighted the superficial part with a green outline, and the deep part with a blue outline:
Origin: Both parts of the masticatory muscle begin from the zygomatic arch.
Attachment: both parts of the masticatory muscle are attached to a special place on the lower jaw - to the masticatory tuberosity (tuberositas masseterica). Let me remind you that the chewing tuberosity is located on the outer surface of the branch of the lower jaw (ramus mandibulae).
Function: raise the lower jaw, chewing and helping to pronounce words. Also, the superficial part of the masseter muscle helps push the jaw forward. We will push it back using the temporal muscle, as you remember.
III. Lateral pterygoid muscle (musculus pterygoideus lateralis).
Now we need a tablet with a skull, which we look at as if from inside the oral cavity (cavitas oris). Something like this:
We turned the skull with the back of the head towards us and sawed it in the frontal plane so that we could look from the inside at the oral cavity, gums and teeth.
Let's look at the lateral pterygoid muscle. Here we can see both lateral pterygoid muscles, so I've highlighted both:
The lateral masseter muscle has two parts - upper and lower.
a) Upper part.
Origin: Infratemporal crest of the greater wing of the sphenoid bone. Let's remember the sphenoid bone (os sphenoidale) - it has a body (corpus), large wings (alae majores) and small wings (alae minores), as well as pterygoid processes (processus pterygoidei).
For some reason, many people like to confuse large wings and pterygoid processes. Let's look at a simplified diagram (front view) so as not to confuse these anatomical formations:
We are interested in the large wing. It is on this that the small infratemporal crest (crista infratemporalis) is located. This is where the origin of the superior portion of the lateral pterygoid muscle is located:
The upper part of the lateral pterygoid muscle is attached to the temporomandibular joint (articulatio temporomandibularis).
b) The lower part of the lateral pterygoid muscle also begins with the sphenoid bone. Now we need to shift our attention from the large wing a little lower - to the pterygoid process (processus pterygoideus). It seems to split into two plates - medial and lateral. Look at the penultimate picture - there I highlighted the pterygoid processes in brown.
Let's find the lateral plate (lamina lateralis) of the pterygoid process. This is, in general, not difficult:
It is from this plate that the lower part of the lateral masseter muscle begins.
So, the beginning: the lateral muscle (its lower part) begins with the lateral plate. Great memory, by the way.
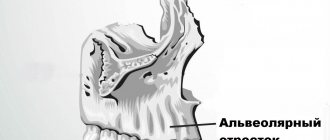
Attachment: pterygoid fossa (fovea pterygoidea) of the lower jaw. Not a particularly well-known anatomical formation, so I found this diagram:
Our pterygoid dimple is located at number 4.
The function of the lateral pterygoid muscle is to raise the jaw (like all masticatory muscles), as well as to abduct the lower jaw in the direction opposite to the muscle. For example, the left lateral pterygoid muscle, when contracted, moves the lower jaw to the right side.
IV. Medial pterygoid muscle (musculus pterygoideus medialis). Let's take a tablet we already know to look at this muscle:
Beginning: Pterygoid fossa (fossa pterygoidea) of the sphenoid bone. By the way, the lower jaw also has, as you remember, a pterygoid fossa, only it is called fovea pterygoidea, so as not to be confused. Ancient anatomists are very prudent guys, definitely.
To be honest, I find it difficult to show it on a tablet. I don’t have a skull at hand at the time of writing this article, but the respected Sinelnikovs indicate in their atlas that “... the medial and lateral plates limit the pterygoid fossa.” Moreover, in the illustration closest to the text, the fossa pterygoidea is indicated on the lateral plate (two pictures ago I highlighted the lateral plates of the pterygoid processes in red). The Sinelnikovs are right in any case - they are the kings of anatomy, after all. I advise you, dear readers, on occasion to ask your teachers about the location of this hole.
In general, speaking about the beginning of this muscle, we focus on the lateral plates of the pterygoid processes of the sphenoid bone and clarify the fossa with the teachers.
Insertion: pterygoid tuberosity of the lower jaw. There won't be any difficulties here anymore, here's where this place is:
Function: Raises the mandible, as well as “pushes” the mandible to the opposite side (i.e., similar to the lateral pterygoid muscle).
Pathology of the masticatory muscles
Pathology of the masticatory muscles can manifest itself in the form of dysfunction - paresis, paralysis; for example, with damage to the trigeminal nerve or its nucleus, atrophic paralysis of the stomach is observed. With unilateral damage to the trigeminal nerve, chewing, although difficult, is possible due to the healthy side. With bilateral atrophic paralysis of the stomach, chewing is impossible, the lower jaw droops. This picture can be observed in amyotrophic lateral sclerosis, when the pyramidal tracts and nuclei of the motor cranial nerves are affected. The gland can also be affected by tick-borne encephalitis. The function of the stomach m. is sharply disrupted by trismus (see) - a tonic spasm of the stomach m., which can be caused by an inflammatory process in the lower jaw or in the soft tissues adjacent to the area of location or attachment of the stomach m. Spasm of the stomach m. .—a characteristic symptom of tetanus, can be observed with meningitis, in some cases - as a hysterical reaction.
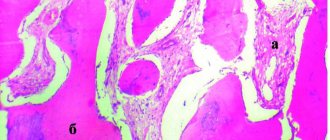
Rice. 2. True bilateral hypertrophy of the masticatory muscles themselves.
Hypertrophy of the m. is rarely observed, and unilateral hypertrophy of the m. is more common. masseter There are so-called true and false hypertrophy of m. masseter False hypertrophy is the development of lymphoid tissue or a vascular tumor in the area of the masticatory muscle. True hypertrophy of the stomach m. has not been sufficiently studied. Occasionally it is observed with malocclusion. Clinically, hypertrophy manifests itself only as a violation of the configuration of the face (Fig. 2); on the side of hypertrophy, the shape of the angle of the lower jaw can also be changed. It is necessary to differentiate true hypertrophy from benign neoplasms in the area of the gastrointestinal tract (lymphoma, lipoma).
G. m. are involved in patol, the process of jaw injuries, facial wounds, specific inflammatory processes (actinomycosis), as well as malignant tumors on the face.
Features of the masticatory muscles:
- All chewing muscles are attached to the lower jaw (mandibula);
- All masticatory muscles elevate the lower jaw, performing chewing and facilitating the correct pronunciation of words;
- The chewing muscles, unlike the facial muscles, have fascia.
These features are not indicated in atlases and textbooks, and, as a rule, they are not required to be mentioned in tests. I brought them specifically to make it easier for you to navigate - as soon as we talk about any masticatory muscle, you immediately understand that it attaches to the lower jaw and lifts it. That is, one name of a muscle group is enough to remember the function and place of attachment.
Treatment
Treatment of patol, conditions of glandular m. consists of treating the underlying disease (infectious disease of the nervous system, injury, tumor); with true hypertrophy of the t. masseter - orthodontic treatment (see Orthodontic methods of treatment) in order to eliminate malocclusions; with pronounced hypertrophy, resulting in facial asymmetry, partial surgical excision of the hypertrophied muscle is possible; if a tumor localized in the area of the gastrointestinal tract is detected, appropriate treatment is given.
Bibliography:
Vorobiev V. and Yasvoin G. Anatomy, histology and embryology of the oral cavity and teeth, p. 119, M., 1936; Gorenshtein Ya. I. On hypertrophy of the masticatory muscles, Dentistry, No. 4, p. 87, 1965; Ivanitsky M. F. Human Anatomy, vol. 1, p. 379, M., 1965; L e r n e r I. O. Hypertrophy of the masticatory muscles, Dentistry, No. 2, p. 40, 1960, bibliogr.; LimbergA. A. Vascular tumor with multiple stones in the thickness of the masticatory muscle, ibid., No. 4, p. 90, 1965; Morphology of the maxillo-mandibular apparatus, Proc. symp. 9th. Int. congr. Anat., Lpz., 1972; S i with her H. Oral anatomy, St Louis, 1965.
HH Mosolov, V. M. Bezrukov.
Lexical minimum
- Mandibula;
- Musculus temporalis;
- Fornix cranii;
- Processus coronoideus;
- Fossa temporalis;
- Musculus masseter;
- Arcus zygomaticus;
- Tuberositas masseterica;
- Ramus mandibulae;
- Musculus pterygoideus lateralis;
- Cavitas oris;
- Os sphenoidale;
- Alae majores;
- Alae minores;
- Processus pterygoidei;
- Crista infratemporalis;
- Articulatio temporomandibularis;
- Lamina lateralis;
- Fovea pterygoidea;
- Musculus pterygoideus medialis;
- Fossa pterygoidea.