Other causes of dental deformities
In addition to deformations of the development of the skull, other reasons can lead to changes in the dentition:
- Poor posture. When posture is impaired, the body begins to adapt. Not only the position of the spine changes, but also other parts of the musculoskeletal system. These adaptive changes affect the dentofacial apparatus. A defect in the dentition develops.
- Bad habits in a child. This may involve prolonged pacifier or finger sucking. Such habits greatly affect the formation of the dentition and can lead to tooth movement and changes in bite.
- Intrauterine pathologies. They may be due to various reasons. For example, diseases suffered by the mother during pregnancy. As a result, deformations of the jaws and tooth buds may develop.
- Periodontal diseases. Weakened tissues cannot hold teeth in their normal position. They begin to shift, the dentition becomes deformed.
- Partial edentia. When one or more units are lost, the rest begin to shift. As a result, a dental defect develops.
Classification of dentition defects
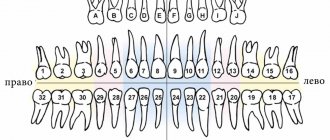
With the loss of a certain number of teeth, from one to fourteen on one jaw, pathological changes in the dentition occur. These changes are manifested by very diverse clinical manifestations, which depend on the number of missing and remaining teeth, on their function, their location in the dentition, the nature of the bite, the condition of their hard tissues and the complex of tissues surrounding them (periodontal).
The main complaints that the patient makes depending on a particular defect related to a specific group of teeth:
- Partial or complete absence of the frontal group of teeth. In this case, patients complain of an aesthetic defect, speech impairment, difficulty biting food, even the inability to do so.
- Partial or complete absence of chewing teeth. The main complaint is a violation of physiological chewing of food and the integrity of the gum mucosa. In the absence of fourth and fifth teeth, aesthetics are compromised, since they are located in the smile zone.
- Loss of a large number of teeth. Clinically manifested by a possible decrease in the height of the lower part of the face, retraction of the lip and cheek.
To select the optimal orthopedic design for replacing dentition defects, attempts were made to somehow systematize and classify these defects. But it is important to note that a universal classification that describes all the existing signs of missing teeth does not yet exist in nature.
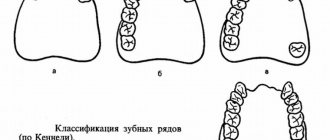
Classification of dentition (according to Kennedy): a - first class; b - second class; c - third grade; g - fourth grade.
The most commonly used and widespread Kennedy classification of dentition defects. It distinguishes 4 classes:
- End defects of the dentition on both sides
- End defect on one side
- Included defect in the dentition in the lateral region
- Included defect in the anterior region
Classes 1,2,3 have subclasses. A dentition defect is classified as a lower class if there are several defects of different locations in the same dentition.
There are many more types of dentition defects, but we will present another option proposed by E.I. Gavrilov; its classification is also often used, although a little more complex. It distinguishes as many as 7 classes:
- End defect on one side
- End defects on both sides
- Unilateral included defect of the lateral dentition
- Bilateral included defects of the lateral dentition
- Included defect of the anterior dentition
- Combined defects
- Single preserved tooth
It should be noted that all of the above classifications do not take into account a number of important factors, such as, for example, the condition of the periodontium, the ratio of the dentition of the upper and lower jaws as a whole. And many other important nuances. Therefore, just determining which class of defect a particular clinical case belongs to does not guarantee the success of treatment (for example, metal-ceramic prosthetics). Only the use of complex diagnostics and comprehensive analysis of the problem can provide confidence in the accuracy of planning and implementation of successful treatment.
Diagnostics is the first and key step in correcting dental defects. Do you want to know why it’s impossible to do without diagnostics?
In our clinic, diagnosis and treatment planning are at the forefront of any problem. Our specialists will help you not only understand what exactly your dental problem is. And they will not only tell you how to solve it correctly, but also provide treatment (dental prosthetics) at the highest level. We'll be happy to help!
During a direct examination by a specialist, you will be able to find out your exact diagnosis, as well as receive a referral for diagnosis or a treatment plan.
Sergei Vladimirovich Yashin
author of the article
Dentist-orthodontist, maxillofacial orthopedist
More than 7 years of experience
Types of dental deformities
Teeth can move from their normal position in different ways. Depending on the type of displacement, types of dental deformations are distinguished:
- Rotation of a tooth relative to its axis.
- Tilt towards the palate, cheek, tongue.
- Vertical displacement of teeth, leading to their lengthening.
- The distal displacement of one unit back in relation to the rest of the dentition.
- Mesial displacement is the opposite of distal displacement, since the deformed tooth moves forward.
- Crowding is characteristic of an underdeveloped small jaw. There is not enough space for normal development of the dentition. The teeth move in different directions, overlapping each other.
- Gaps and crevices in the dentition develop if the jaw size is large. Visible gaps (diastemas, tremata) form between adjacent dental units.
In complex cases, a combined displacement can be observed, combining different anomalies. Visually, such defects look like uneven teeth.
Erosion
Looks like areas of damaged enamel with a changed shade. In the affected areas, during erosion, hard tissues soften, gradually collapse, and a cavity is formed that reaches the dentin. At this stage, the tooth begins to hurt, react to any irritants, and the defect itself becomes clearly visible. Erosion has several possible causes:
- frequent consumption of sour or sweet foods;
- brushing teeth with hard brushes or pastes with an abrasive effect;
- low calcium content in hard tissues (due to metabolic disorders, pregnancy, certain diseases).
Erosion looks like a spot with a smooth, non-shiny surface. It is treated by performing remineralization and tooth restoration. It is important to find and eliminate the cause of the defect. If this is not done, erosion will appear in new places.
Diagnosis of dental deformations
Dental deformities are not an independent diagnosis. Treating them only with traditional methods used to correct the bite is not always effective. If the cause that caused the deformation of the dentofacial apparatus is not identified and eliminated, there is a risk of relapse.
To make a diagnosis and select treatment options for dental deformation, doctors at our clinic use:
- Visual examination of the oral cavity. The doctor will definitely ask you when the problem began. This will help determine the causes of the development of malocclusion.
- Paraclinical studies. After a visual examination and medical history, you will be prescribed tests: x-rays of the teeth and alveolar process, x-rays of the temporomandibular joint, tomography, etc.
Examination of the dentition gives the dentist a lot of information about the bite. With its help, you can determine the nature of the deformation, the condition of the periodontium, and roots. Instrumental diagnostic methods are used to diagnose functional and morphological disorders.
With the help of examination and questioning, you can obtain other data on the condition of the dentofacial apparatus:
- Position of teeth in the jaw. The position of the dentition is assessed in relation to the sagittal plane, focusing on the line between the incisors. If this line is displaced, a more precise occlusion study is necessary. The doctor determines the size of the incisal overlap, the position of individual units, and the nature of their occlusal surface.
- Features of the movement of the lower jaw during opening and closing of the mouth. Zigzag movement of the jaw may indicate pathologies of the TMJ and masticatory muscles.
Impaired closure of teeth and their rotation around their axis. Movement of molars and premolars is easily diagnosed during examination.
Instrumental diagnosis of dental anomalies allows an accurate diagnosis.
Malocclusion
When the teeth close completely in central occlusion (the upper and lower dentitions are tightly connected), they form a bite. Since the dentition in central occlusion can close in different ways, there are different types of occlusion.
The correct bite is the following position of the dentition: the incisors of the lower jaw contact the cutting surface with the tubercles of the incisors of the upper jaw. In this case, the overlap of the lower incisors with the upper ones is approximately a third of the size of the lower incisors. But the bite is individual - its type depends on the size of the teeth and their shape, the number of teeth in the oral cavity, and the size of the jaw bones.
If the patient begins to develop defects in the dentition, the bite may be affected. The main types of malocclusion are as follows:
- open bite - when the dentitions close, a vertical gap is found between the teeth;
- crossbite - a violation of central occlusion, in which there is also asymmetry of the face, limited lateral movements of the lower jaw, decreased chewing function and overload of supporting dental tissues;
- deepest bite - with this type of bite, the upper incisors overlap the lower incisors by more than a third, up to complete overlap.
An incorrect bite seriously increases the load on your teeth when eating food. Over time, teeth with an incorrect bite become mobile, the necks of the teeth become exposed, pain appears in the masticatory muscles and even headaches. Therefore, even if an outward malocclusion does not bother you, it still needs to be treated to avoid health problems in the future.
Treatment
Treatment methods for dental deformities are chosen depending on the type of pathology. Most deformities not associated with the loss of antagonist teeth develop in childhood. Therefore, the problem needs to be resolved as early as possible. In orthodontics they use:
- Plates. Can be used immediately after baby teeth are replaced by permanent teeth. The plate puts pressure on the dentition, as a result it is aligned. Installation of plates is indicated for patients aged 7-12 years. At this time, the child’s bones are growing rapidly, so the technique will be effective.
- Trainers. They can be used in early childhood. The trainer is a silicone structure that resembles a mouth guard. They are worn for several hours. The elastic trainer protects the dentition from excessive pressure from the tongue and cheeks and prevents teeth from moving.
- Braces. Can be installed on children over 12 years of age. The orthodontist determines the need to use braces based on the results of the study.
These are the most common options for orthodontic treatment of dental deformities. Specialists at the Zuub.rf dental clinic believe that the approach to eliminating this problem should be comprehensive. It is important not only to visually straighten the dentition and correct the bite, but also to eliminate the cause that led to the development of the anomaly.
Hyperesthesia
This is a condition in which the enamel thins and becomes overly sensitive. Sometimes this can cause the shade of the crown to change, but more often hyperesthesia is manifested by acute aching pain when the teeth come into contact with irritants. The reaction can occur to drinks that are too cold or hot, sour or sweet. Hyperesthesia can have several causes, including too aggressive whitening, poor daily hygiene, regular damage to the enamel when brushing your teeth or due to contact with sour or sweet foods and drinks. It also occurs with calcium deficiency, malocclusion (if occlusion is disturbed) and as a complication of bruxism (teeth grinding during sleep). To treat hyperesthesia, you need to eliminate the cause of thinning enamel (for example, adjusting your daily dental care, correcting your bite, or using mouth guards for bruxism). To remove high sensitivity, remotherapy is performed. To do this, the teeth are coated with a remineralizing composition and fluoride varnish. While the enamel remains highly sensitive, it is better to rinse your mouth with clean water after each meal.
Diagnostics
To successfully treat patients, a thorough examination must be performed. When initial signs appear, patients should consult a dentist. He will examine the oral cavity, assess the condition of the gums and chewing organs. If necessary, the patient will be referred for additional studies. According to indications, instrumental diagnostics are prescribed. If consultation with an endocrinologist, therapist, or gastroenterologist is needed, the patient is referred to these specialists. Consulting an orthodontist is important for drawing up a correction and prosthetic plan.
As a rule, the pathology has a specific severity, so it is diagnosed during a visual initial examination. Establishing provoking factors most often requires additional diagnostic procedures. In order to make a final diagnosis, as well as determine therapeutic methods, doctors may refer the patient for radiography. It will allow you to obtain complete information and create the correct treatment plan.
Fluorosis
A rare disease that occurs when too much fluoride enters the body. It accumulates and can provoke changes in the structure of hard tissues and the appearance of non-carious defects. With fluorosis, colored spots or stripes appear on the enamel. Hard tissues may gradually deteriorate. In this case, deep, extensive defects are formed.
A person can receive an excess amount of fluoride in several cases: with water, when working in hazardous industries and (very rarely) when taking certain medications. During treatment, the cause of excess fluoride is eliminated (for example, replacing water with bottled water), and then teeth are restored, removing defects.
Necrosis
This is the death of hard tissue cells, due to which multiple defects appear on the surface of the crowns, as well as on the tooth root. The structure of the cells changes, and destruction can affect not only dentin, but also the pulp. Necrosis is rare and is usually not directly related to the condition of the teeth. It can be caused by severe toxin poisoning, hormonal imbalance, or severe systemic diseases. Treatment at the dentist is symptomatic: restoration of hard tissues, remineralization, prosthetics for complete tooth destruction. The main therapy must be related to the disease that caused the necrosis, and dental treatment only complements it.
You have questions?
We will call you back within 30 seconds
+7
Anomalies of dental development - symptoms and treatment
Treatment depends on the type of anomaly and may include tooth extraction, prosthetics with crowns and veneers, surgical and therapeutic intervention.
Supernumerary teeth must be removed. If the crown or root part of adjacent teeth is abnormal or destroyed due to a pathological process, then after a thorough examination the corresponding complete tooth is removed, and the supernumerary one is moved into the dentition. Supernumerary teeth most often have irregular shape, size or structure, so treatment is often completed with restoration with composite material or the creation of an artificial crown or veneer.
for patients with hypodentia and edentia . Partial absence of teeth, as a rule, is combined with a violation of the position of adjacent teeth and antagonist teeth, as well as with anomalies in the shape and size of the dental arches. Therapy will consist of orthodontic correction followed by prosthetics and implantation [7]. Patients with true primary edentia are very rare; they should wear complete removable dentures from an early age. Children often respond well to prosthetics and quickly adapt to them. Due to dynamic age-related changes occurring in the dental system, all removable dentures are replaced with new ones every 1.5-2 years. When making dentures, the doctor and technician take into account the morphological and functional characteristics of the dental system.
Treatment of anomalies in tooth size (macro- and microdentia) is usually orthopedic. If macrodentia and microdentia are combined with anomalies in the shape and size of the dentition, malocclusion, then preliminary orthodontic preparation will be required. It consists in the correct placement of teeth and allows you to subsequently qualitatively restore the desired tooth anatomy with crowns or veneers. In case of mild pathology with a small difference in the height or width of the teeth and their normal relationship with the size of the jaws and the type of face, orthodontic treatment can be limited.
Treatment of patients with abnormal tooth shapes involves performing composite restorations and making crowns or veneers that restore the anatomical shape. For concomitant pathologies that require correction of the bite, shape and size of the dental arches, orthodontic preparation will be required.
Treatment of anomalies in the structure of hard dental tissues (hypoplasia, hyperplasia, hypercementosis, amelogenesis imperfecta, medicinal and toxic effects on dental tissues, etc.) is complex and includes therapeutic, orthopedic and orthodontic care.
Treatment of teething anomalies . Early eruption of primary teeth usually does not require orthodontic intervention. If there is a violation, it may be necessary to switch to artificial nutrition instead of breastfeeding. Early eruption of permanent teeth is often caused by untimely loss of baby teeth. It often requires correction of the position of adjacent teeth and antagonist teeth to prevent complications. If the permanent tooth has already erupted, but the baby tooth has not yet fallen out, then the latter is removed, and the direction of eruption of the permanent tooth is corrected, if necessary.
For late eruption of primary teeth, gum massage will be helpful. Delayed eruption of a permanent tooth is usually corrected by an orthodontist. To do this, orthodontic preparation is carried out on the brace system: a place is created for the impacted tooth and a support is prepared for its traction. If it is necessary to open or remove an impacted tooth, the treatment is carried out by a surgeon [1].
Anomalies in the position of teeth are corrected using prosthetics with veneers and crowns, therapeutic restoration and orthodontic treatment with removable (in childhood) and non-removable devices: aligners and brace systems.