Gavrilov’s classification is a clear system of dentition defects with an accessible structure. This combination of elements has proven its practicality in the technique of dental prosthetics.
“A feature of Gavrilov’s classification is the separation of jaws with single preserved teeth into a special group”
A dental arch defect is considered to be a violation of the integrity of a row in which from one to 13 teeth are missing. Three types of defects are identified, in ascending order:
- small defects are characterized by the absence of up to three teeth in a row;
- medium defects - loss of three to six teeth in a row;
- A shortage of more than six pieces is considered large;
Included is a gap in a row of preserved teeth localized on both sides.
End – absence of teeth in the arch, limited only on one side. Both species are found on both the lower and upper jaws.
Why is it necessary to systematize defects in dental arches?
There are a great variety of different combinations of dental defects. For example, if you try to create a mathematical model of these combinations, including all available characteristics and taking into account the combination of various characteristics. As a result, we get at least 4*109 options, each of which has the right to exist. Such a number of variations clearly shows the need to develop generalized classifications. This is more convenient in practical use and allows doctors from different countries to understand each other.
How to classify if there are several defects at the same time
Classification of dentition defects according to Kennedy can cause certain difficulties if, after a visual examination of the patient’s oral cavity, several types of edentia are found on one jaw.
In such a situation, E. Kennedy focuses on the fact that in the presence of 2-3 defects that belong to different classes, the dental pathology of the dental arch must be assigned to the smallest class in its order. Based on this, further selection of orthopedic treatment methods is carried out, and options for using prostheses of one modification or another are considered.
Dr. Kennedy's classification of dentition defects is a practical method for determining the various types of edentulism in the upper and lower jaw. Using this classifier, a dentist is able to quickly visually diagnose the condition of the dental arch of a patient who is missing a large number of teeth.
The structure of the Kennedy dentition defects classifier contains 4 classes, the first 3 of which are divided into additional subclasses. Edentia of the molars of the chewing group, defects of the anterior and lateral sections are distinguished. Classification subclasses include mixed types of edentia, when a certain number of teeth are simultaneously absent in different parts of the jaw apparatus.
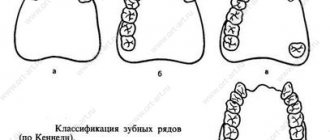
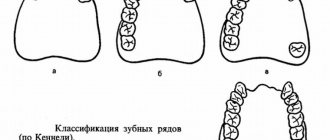
Classification of dentition defects according to Gavrilov
While developing his system of characteristics for dental prosthetics, Professor Gavrilov identified jaws with preserved free-standing teeth as a separate category. This decision is completely justified, since the manufacture of dentures for this type of jaw has its own characteristics.
Dental arches with defects are divided into four classes:
- absence of teeth at the ends of the jaws (end defects) on one or both sides of the jaw;
- defects limited by teeth on both sides (included), anterior and lateral one and two-sided;
- the presence of the first and second classes in various combinations - combined defects;
- dental arches with free-standing teeth.
| One-sided end flaw | Double end flaw |
Additionally, it is proposed to subdivide the dentition into 6 types.
Differences in the classification of dental defects according to Gavrilov
Two classifications are widely used, and.
Kennedy's system of signs has four types:
- terminal defects on both sides of the jaw;
- the same thing, but only on one side;
- included defects in the side area of the rows;
- the same as in the third point, but in the anterior section;
Betelman identifies two categories. The first includes dentition with several flaws, on one or both sides, but there must be at least one “end” defect. The second category is any types and combinations of “included” defects.
There are some challenges to using Dr. Kennedy's system. When diagnosing various combinations that do not fall into its classification, it is proposed to lower the gradation of the class. This can lead to some confusion about the diagnosis.
As can be seen from the three above systems, the classification of dentition according to Gavrilov seems to be the most specific.
In conclusion, it should be noted that none of the systems considered does not provide an accurate picture in relation to a single clinical case. A large number of factors influencing incomplete tooth loss do not allow us to fit them into such a narrow framework
The doctor plans orthopedic treatment individually for each patient, taking into account the number and location of missing teeth, periodontal condition and level of health. But there are still general principles for choosing a prosthesis design depending on the extent and location of the defect. For recording in the chart and professional communication between dentists, it is more convenient to use a symbol of the clinical situation, rather than its full description. The classification of dental defects simplifies the algorithm for choosing a treatment plan and filling out documentation.
Gaps in the dentition
A dental arch defect is considered to be a violation of the integrity of a row in which from one to 13 teeth are missing. Three types of defects are identified, in ascending order:
- small defects are characterized by the absence of up to three teeth in a row;
- medium defects - loss of three to six teeth in a row;
- A shortage of more than six pieces is considered large;
Included is a gap in a row of preserved teeth localized on both sides.
End – absence of teeth in the arch, limited only on one side. Both species are found on both the lower and upper jaws.
Which classification is better?
Classics of orthopedic dentistry - Kennedy classification. In it, dentition defects are divided into 4 classes: one- and two-sided end defects, included in the lateral and frontal areas. At the same time, the absence of several teeth in the lateral area on one side and on both sides must be classified as one class, which in practice is not always convenient. Therefore, some dentists in the clinic use a more detailed classification of Gavrilov. The classes in these systems may not match in number, so when formulating a diagnosis, the doctor must indicate which classification he uses, according to Gavrilov or Kennedy.
Class I – chewing teeth are absent on both sides, the dentition is shortened and ends at the 5th 6th tooth on each side;
Class II – shortening of the dental arch on one side, molars missing on the right or left;
Class III – several teeth are missing in the lateral area, but the trailing ones are preserved;
Class IV – absence of incisors or canines in the anterior part of the jaw.
If there are several isolated defects, a lower class is assigned. For example, if two teeth are missing in the front area and three molars on the right, the defect is classified as first class. In this regard, Kennedy's classification is not entirely convenient. One group includes fundamentally different clinical situations, for which the prosthetic plan will be different.
Class 1 – absence of chewing teeth on the right or left;
Class 2 – loss of distal support of the dentition on both sides;
Class 3 – several chewing teeth are missing and there are closing teeth on one side;
Class 4 – absence of several molars with preservation of distal supports on both sides;
Class 5 – absence of several incisors and/or canines;
Class 6 – combined defects of the dentition;
7th grade – one tooth is retained on the jaw.
The Gavrilov classification is more detailed in comparison with the Kennedy taxonomy and better reflects the clinical situation, therefore, when making a diagnosis, it is easier to plan treatment using it.
Kennedy classification
Class I – chewing teeth are absent on both sides, the dentition is shortened and ends at the 5th 6th tooth on each side;
Class II – shortening of the dental arch on one side, molars missing on the right or left;
Class III – several teeth are missing in the lateral area, but the trailing ones are preserved;
Class IV – absence of incisors or canines in the anterior part of the jaw.
If there are several isolated defects, a lower class is assigned. For example, if two teeth are missing in the front area and three molars on the right, the defect is classified as first class. In this regard, Kennedy's classification is not entirely convenient. One group includes fundamentally different clinical situations, for which the prosthetic plan will be different.
According to Kennedy and Gavrilov
II class according to Kennedy – 1 according to Gavrilov
Since there is no distal support, it is impossible to make a permanent bridge, there is simply nothing to fix it to. Previously proposed cantilever structures with an overhanging artificial crown did not stand the test of time. They do not last long and, in addition, lead to loosening and falling out of the support.
The following orthopedic treatment options are possible:
- partial plate removable denture is not fixed well enough and tips over during chewing, since the load falls on one side of the plate;
- The clasp prosthesis, due to the presence of cast clasps and a metal arch, tilts to a lesser extent and acts less aggressively on the supporting teeth;
- prosthetics on implants according to the principle of one tooth - one implant involves the manufacture of a non-removable structure. In this case, chewing efficiency is completely restored and there is no additional stress on the remaining teeth. In the absence of special contraindications, this is the method of choice.
I class according to Kennedy – 2 according to Gavrilov
The same prosthetic options are used as in the previous case. Bilateral end defects differ in that in this case the fixation and function of removable dentures is better due to the uniform distribution of the load on both sides. When choosing a fixed structure, a clasp denture is preferable, especially in the upper jaw. The presence of a metal arc allows you to reduce the size of the plate and leave the sky open.
Fixed prosthetics are possible with the use of implants. If the teeth have been lost for a long time and no treatment has been carried out, the bone tissue may not be enough, but in this case it can be increased using a special operation. With good hygienic skills and the absence of contraindications, the effectiveness of prosthetics on implants in this case is superior to that of removable prosthetics.
III class according to Kennedy – 3 according to Gavrilov
It is possible to restore the defect using both removable and non-removable structures:
- A bridge supported by teeth that limit the defect is a budget option. The advantage is that the design is non-removable, the disadvantage is the increased load on the supporting teeth. Periodontal diseases and mobility of remaining teeth can significantly narrow the indications for such treatment.
- removable clasp denture is a viable prosthetic option, but not entirely comfortable. Firstly, the structure is removable, and secondly, if there is a one-sided defect, the overturning effect will work.
- installation of implants is again leading in terms of comfort and physiology. There is no load on the supporting teeth, there is no need to grind them down to remove healthy tissue, and the chewing function is completely restored.
III class according to Kennedy – 4 according to Gavrilov
The options are the same, but clasp dentures in terms of ease of wear and restoration of function are catching up with fixed structures due to the bilateral uniform distribution of the load.
IV class according to Kennedy – 5 class according to Gavrilov
Removable and bridge dentures may well restore the function of lost teeth, but in order for their fixation to be adequate, it is necessary to use clasps that will be clearly visible on the teeth. But in the anterior section, aesthetics are needed. Bridges, with sufficiently strong support, are functionally satisfactory, but can also compromise aesthetics, especially with atrophy of the alveolar process, when a significant gap forms between the neck of the artificial tooth and the gum.
Implants help completely restore the chewing efficiency and aesthetics of the front teeth. This is the only localization in which installation of an implant simultaneously with tooth extraction is preferable. This creates optimal conditions for healing and prevents loss of gums and bone tissue. The aesthetic result of such structures is beyond competition.
6th grade according to Gavrilov
For combined defects, planning is strictly individual. This option is not reflected in Kennedy's classification.
7th grade according to Gavrilov
This type of dentition defects in the Kennedy classification is classified as bilateral end, while the clinical manifestations and treatment plan in these two cases can differ radically. It was previously proposed to use single teeth as a support for fixing a removable denture, especially in the lower jaw, where the conditions for this, to put it mildly, leave much to be desired. With the advent of implantation, the need to save the last tooth by hook or by crook has disappeared. Prosthetics for single standing teeth, as well as for completely toothless jaws, are carried out using implants.
Changes in the sequence of the dentition may involve disturbances in the continuity and unity of the teeth in the upper or lower jaw, and the reasons for this phenomenon can be completely different. These include injuries, bruises, infectious diseases of the oral cavity, lack of proper treatment for caries, which results in complications.
End defects of the dentition on both sides
Bilateral terminal defects of the jaw apparatus are a pathological condition of the upper or lower dental arch, in which the molars of the chewing group are completely or partially absent. The complexity of this type of edentulism lies in the fact that in most cases the doctor cannot use traditional orthopedic dentures due to the insufficient number of teeth that are used as support for bridges.
The solution to this problem is the installation of removable dentures of various types and modifications. Orthopedic treatment of patients with bilateral terminal defects of the dentition largely depends on the complexity of the clinical case, the general condition of the patient’s oral cavity and jaw apparatus.
1 subclass
Kennedy's classification of dentition defects with bilateral terminal edentia includes the presence of 1 subclass.
In this case, a patient with a similar diagnosis is missing not only the 6th, 7th, 8th chewing molars of the upper or lower jaw, but also edentia of the 1st and 2nd teeth.
2 subclass
End defects of the jaw apparatus on both sides of subclass 2 are characterized by the absence of chewing molars, as well as the loss of 1, 2 teeth on the right and one 4 tooth on the left side.
3 subclass
The third subclass of bilateral terminal adentia is expressed by the absence of 1, 2, 4 teeth on the right and 4 molars on the left side. At the same time, the patient’s 6, 7, 8 teeth were also completely removed.
Methods for eliminating end adentia of the dentition on both sides
For orthopedic treatment of defective teeth in the chewing group, which are missing on both the right and left sides, various types of prosthetics are used. The selection of a specific therapeutic technique is carried out using a classifier developed by Dr. Kennedy.
Prosthetics using a cantilever bridge
The classification of dentition defects according to Dr. Kennedy is a visual aid for practicing orthopedic doctors, who have the opportunity to conduct a quick visual diagnosis of patients with signs of edentia of varying complexity.
In the presence of a bilateral terminal defect of the jaw apparatus, the use of a cantilever bridge is justified as the main method of prosthetics for the chewing group of teeth in the upper and lower jaw. The use of this method of eliminating adentia is advisable if 2-3 molars located next to the end defect require correction using crowns.
The disadvantage of eliminating bilateral end adentia using a cantilever bridge is that its installation requires grinding of adjacent teeth. These molars act as a support for attaching the orthopedic structure. Dentists assessing this dentition defect using the Kennedy classifier use the cantilever bridge prosthetic method only in extreme cases.
This is associated with a high risk of developing associated complications that appear during the first 10 years, namely:
- pain under the crowns of ground teeth;
- destruction of healthy molars located under the bridge;
- curvature of the teeth that serve as supporting teeth to hold the cantilever bridge.
The effectiveness of prosthetics for bilateral end defects of the dentition using a cantilever bridge depends on the qualifications of the dentist, as well as the quality of the work performed. The advantage of this orthopedic technique is the rapid production of prostheses, ease of installation and affordable cost.
Prosthetics with removable dentures
Elimination of the end defect of the dentition of the upper or lower jaw, which affected both sides at once, is also performed using a standard removable bridge. This prosthesis is an imitation of chewing teeth. A removable bridge from the 5th, 6th, 7th right and left sides of the upper or lower jaw is connected by a single metal frame, which is fixed around the surface of healthy teeth using special fasteners.
The connecting elements of the prosthesis are attached to the root part of the molar, which completely eliminates the presence of an aesthetic defect. If necessary, a person can independently remove the installed prosthesis, carry out all hygienic procedures, and then re-attach it to the surface of the jaw apparatus.
Application of implants
Using the implantation method, it is possible to eliminate bilateral end pathology of the dental arch, even in the complete absence of molars of the chewing group. To do this, an implant is installed in the jaw bone tissue with signs of edentia, which will serve as an abutment tooth.
After completion of all surgical procedures and the patient’s recovery after implantation of the metal structure, a permanent prosthesis is installed. In this case, the implant is an integral part of the cantilever bridge, the second edge of which is attached to healthy, ground teeth with a crown on.
Classification of dentition defects according to Kennedy
There are several ways to describe this pathology. The most common is the Kennedy classification. It is based on the following defects:
- first group - the dentition is limited on both sides by the 5th or 6th tooth, with no chewing crowns;
- second group - the dentition is shortened due to the absence of molars on one side or the other;
- third group - the chewing crown is preserved, but there are no teeth in the lateral zone;
- fourth group - the structure of the anterior part of the jaw is disturbed, in particular, there are no fangs or incisors.
If the Kennedy classification is used for diagnosis, orthopedics implies complicated treatment, since if there are several anomalies at once, then the disease is assigned a lower group. Because of this, the prosthetic plan also changes. Different clinical cases may belong to the same group.
Kennedy classification of defects
Kennedy's classification contains 4 main groups:
- Kennedy class 1 : bilateral terminal defects located posterior to the remaining natural teeth. The class indicates that there are no chewing teeth in the distal portions of the dentition.
- Kennedy class 2 : unilateral dental defect located posterior to the remaining natural teeth. The patient has no chewing teeth on only one side of the dentition.
- Kennedy class 3 : included defect of natural teeth in the anterior or posterior regions. There is no end defect due to the presence of supporting chewing teeth on one side of the jaw. This class is most often observed in patients.
- Kennedy class 4 : included defect of the frontal area. This class is quite rare, but can be observed in patients with periodontal diseases, or in patients after trauma to the front teeth.
| Kennedy class 1: bilateral end defects | Kennedy class 2: unilateral end defects |
| Kennedy class 3: included defect in the lateral region | Kennedy class 4: included anterior defect |
In 1954, Kennedy's classification was supplemented (modified) by Dr. Applegate, who added 8 rules:
- The classification should reflect the real picture in the dentition and not precede tooth extraction.
- If a wisdom tooth is missing from the dentition and will not be replaced, then it is not taken into account in the classification.
- The third molar is taken into account if it is used as an abutment tooth
- If the second molars of one jaw are missing and they will not be replaced, then they are ignored in the classification
- Distal defects always serve as the basis for choosing the correct class
- Additional dental defects are called subclasses and are recorded separately
- Only the number of defects is taken into account, their length does not matter
- Only one, Kennedy grade 4 has no subclasses! All defects that are located distal to the frontal area determine the class of dentition defect.
Causes of dental defects
There are several reasons that lead to the problem (to eliminate them, it is necessary to classify the pathology as a specific group, which is why the Kennedy classification exists):
- Congenital anomalies, in particular edentia (lack of teeth) due to mother's illness during pregnancy, due to which the rudiments of teeth may be absent, there may also be errors in the structure of the enamel, which is inherited.
- Having bad habits. In children, using a pacifier and artificial feeding, sucking fingers; in adults, the habit of cracking nuts, such as pistachios, can lead to tooth loss.
- Caries if left untreated. Regular visits to the dentist will help keep your teeth intact.
- Inflammatory processes. If purulent inflammation occurs, the tooth must be removed immediately. Periodontitis, cysts, periodontitis and other dental diseases can lead to this.
- Mechanical injuries, which is especially important at the age of 6-9 years. During this period, the baby teeth are replaced by molars, and a strong blow can damage the root.
- Children's diseases, such as rickets, pneumonia, acute respiratory diseases that appear during the formation of teeth. They have a negative impact on the structure of the central incisors.
- The presence of a neoplasm in the periodontium. If it is detected, then immediate tooth extraction is necessary. Neoplasms can occur as a result of disruption of the thyroid gland, gastrointestinal tract, and also due to a lack of vitamins.
Symptoms of defects
The Kennedy classification of defects indicates that the problem arises as a result of tooth loss or development. Signs depend on many factors:
- the exact location may be the lateral or front teeth on the lower or upper jaw);
- flaw parameters;
- type of defect (can be included or terminal);
- bite structures;
- patient's age;
- condition of the gums and existing teeth;
- time from the moment of tooth loss to the start of treatment;
- reasons for the defect.
To identify a defect, you need to come to an appointment with a dentist, who will conduct an examination and determine the problem. The main complaints from patients that force people to go to the doctor are:
- malocclusion;
- inability to fully chew food;
- jaw bone deformation;
- in some cases, diction problems.
Elimination of the defect depends on the group of the disease, for which a certain scheme must be used, and the Kennedy classification is most often used. Before prosthetics or implantation, the dentist must carry out professional teeth cleaning, during which they eliminate caries and eliminate any inflammatory processes.
Kennedy classification with subclasses
Kennedy classification with subclasses
Kennedy's classification of dental defects is used only in prosthetic dentistry, as is the later Betelmann classification. To determine the destruction of the coronal part of a separate tooth, the Milikevich IROPD classification is used; dental therapists in clinical practice use Black’s classification to correctly detail carious processes.
Prevention methods
An adult can independently take measures to prevent the occurrence of defects, which can be diagnosed using the Kennedy classification. The main enemy in this situation is caries, so adequate oral hygiene and regular visits to the dentist are necessary. This also applies to children. Parents may neglect the oral hygiene of a child with baby teeth because they think they will fall out anyway and don't need care. But that's not true. Also, if detected, they must be treated promptly. Ignoring any problems in the oral cavity can aggravate the situation and lead to tooth loss.
This disease is easily recognized by the absence of one or more teeth, which causes discomfort when chewing and talking. Ignoring such violations can negatively affect healthy teeth and lead to a decrease in the volume of bone tissue in the jaw.
It is very important to promptly seek help from a dentist or orthodontist who can provide adequate treatment.
Types of dentition defects - classifications according to Kennedy, according to Gavrilov, according to Betelman
In the most general terms, the dental disease in question can be classified as follows:
- Errors in the structure of the front teeth. This often applies to canines and incisors.
- Defects in the structure of the teeth that are located behind the canines.
- Defects associated with the outermost crowns in the dentition.
- Disadvantages that are present in the anterior + posterior part of the arch.
The most common are the following groups of classifications:
According to Kennedy
Based on the following defects:
- Group
I. _
The length of the dentition on both sides is limited to the 5th or 6th tooth. There are no chewing crowns. - II .
The length of the dental arch is reduced due to the absence of molars on the left/right side. - III group
.
The trailing crowns at the end of the row are preserved, but several teeth are missing in the lateral area. - IV group
.
The front part of the jaw is subject to deformation: there are no fangs/incisors here.
Organizing treatment with this type of classification is not very convenient: if there are several anomalies at once, the disease is assigned a lower group.
This has an effect on the prosthetic plan: completely different clinical cases may belong to an identical group.
According to Gavrilov
This division of defects is quite detailed: it will be easier for the appropriate specialist to decide on the treatment method.
- I class
.
There are flaws at the end of the dental arch: on the right or left. - II class
.
The distal support on the upper/lower jaw is lost on both sides. - III class
.
In the lateral part of the dentition there are no several chewing teeth, but the trailing crown is present. - IV class
.
The distal supports on both sides are preserved, but there are flaws in the lateral sections of the dentition. - V class
.
Several teeth are missing in front of the arch. - VI class
.
There are defects of a combined nature. - VII class
.
There is only one tooth left on the jaw.
According to Betelman
There are 2 classes, each of which has 2 subclasses.
I
class.
Characterized by the presence of the so-called.
terminal defects
, in which chewing teeth, starting from the 5th or 6th, are absent.
Such flaws can be on one side of the arch ( I subclass
) or on both sides (
II subclass
).
II
class
.
Provides for the presence of included defects when there are no crowns in any place in the dental arch.
- I subclass
.
It is diagnosed if there are one or more included defects, and the number of missing teeth from one defect does not exceed three. - II subclass
.
Characterized by the presence of one or more included defects, and at least one defect is missing more than three teeth.
Classification according to Gavrilov
Class 1 – absence of chewing teeth on the right or left;
Class 2 – loss of distal support of the dentition on both sides;
Class 3 – several chewing teeth are missing and there are closing teeth on one side;
Class 4 – absence of several molars with preservation of distal supports on both sides;
Class 5 – absence of several incisors and/or canines;
Class 6 – combined defects of the dentition;
7th grade – one tooth is retained on the jaw.
The Gavrilov classification is more detailed in comparison with the Kennedy taxonomy and better reflects the clinical situation, therefore, when making a diagnosis, it is easier to plan treatment using it.
Causes of dental defects – what role does heredity or poor oral hygiene play?
Various factors can provoke the disease in question:
- Congenital anomalies
.
This, first of all, includes, which can develop against the background of a mother’s illness during pregnancy. The absence of tooth buds, supernumerary teeth, diastema, and errors in the enamel structure can also be inherited. - Bad habits
.
Long-term use of a pacifier, artificial feeding, and finger sucking negatively affect the formation of a bite. Those who like to crack nuts and pistachios should remember the danger of splitting the crown and damaging the root. - Caries
.
In advanced stages of this pathology, patients can lose several teeth at once. Therefore, oral hygiene, regular visits to the dentist, and timely treatment of carious teeth play an important role in keeping the dentition intact. - Septic phenomena that were formed under the influence of purulent inflammation
.
In case of such reactions, the tooth should be removed immediately, and periodontitis, cysts and some other dental ailments can lead to a similar result. - Injuries
.
Loss of teeth due to fights or falls is especially important for boys aged 6-9 years. During this period, children undergo a change of teeth: a strong blow can cause damage to the root, which will stop its development in the future. - Some childhood diseases (rickets, pneumonia, acute respiratory viral infections)
that are diagnosed at the stage of tooth formation. Such pathologies negatively affect the structure of the central incisors. - Neoplasms in the periodontium
that require tooth extraction. They can arise due to errors in the functioning of the thyroid gland, gastrointestinal tract, heart and respiratory system, and with hypovitaminosis.
Symptoms of dental defects - methods for diagnosing pathology
The manifestations of this pathology will depend on several components:
- The exact location of the defect: lower/upper jaw, lateral/front teeth.
- Flaw parameters.
- Type of defect (on, end).
- Bite structure.
- Patient's age.
- General condition of gums and teeth.
- The amount of time from the moment of tooth loss to the start of treatment.
- Cause of tooth loss/damage.
To identify this disease, instrumental examination is often not required. All you need to do is come to an appointment with a dentist, who during the examination will determine the presence of a defect in the dentition.
The main complaints from the patient will be as follows:
- Errors in bite.
- Inability to chew food normally.
- Deformation of the bone tissue of the jaw.
- Impaired diction (not always).
At the end of the history taking, the dentist may order an x-ray. This will be useful if you need to establish the exact causes of the defect; for a detailed study of the extent of root/bone damage.
Clinical manifestations of dentition defects
There is a violation of the continuity of the dentition, which leads to overload of certain groups of teeth, disruption of chewing and speech functions, and disruption of the functioning of the temporomandibular joint. In the absence of treatment for defects in the dentition, a secondary deformation of the bite and disturbances in the activity of the masticatory muscles are formed. In addition, the absence of front teeth negatively affects the appearance.
Over time, two groups of teeth are formed: those that have retained their functions and those that have lost them. As a result of the fact that the load is distributed unevenly, other dental pathologies occur - displacement of the dentition and deformation of the occlusal surfaces occur. There are two types of dentition defects – included and terminal. When defects are included, the dentition on both sides of the defect is preserved. With end defects, the defect is limited only on the front side.
The main manifestation of a defect in the dentition is a violation of their continuity, which entails the following consequences:
- overload of some groups of teeth;
- speech disorder;
- violation of chewing functions;
- improper functioning of the temporomandibular joint.
If medical care is not received, a secondary bite deformation is formed, and the tone of the masticatory muscles is disrupted.
Over time, two groups of teeth are distinguished: the first - with preserved function, the second - with lost. The load during chewing is distributed even more unevenly, which leads to deformation of the occlusal surfaces, displacement of the dentition, periodontal disease and other diseases.
The absence of front teeth affects the aesthetic appearance and causes psychological discomfort when communicating and smiling.
Treatment methods for dental defects – restoration and straightening
Based on the class/group of the disease, treatment will also vary:
- In the absence of distal support, the ideal solution would be to install implants (each for one tooth). This will help protect healthy teeth from excessive stress and will have a positive effect on chewing abilities. If the patient has contraindications to this procedure, or does not have enough funds to install implants, doctors opt for a bulge prosthesis.
- If there are no lateral chewing teeth, but there are closing crowns, several types of dental restoration can be used:
- Fixed bridge supported by healthy crowns. The negative point is increased pressure on the supporting teeth. However, this method of treatment is the most optimal in terms of money.
- Use of a removable bulge denture. Not the most comfortable design for the patient, and if a one-sided flaw is being repaired, a tipping effect should be expected.
- Restoration through implantation. The condition of the jaw bone is taken into account here. When it atrophies, it is necessary to first build it up.
- Extensive defects in the dental arch are best restored with nylon dentures. They do not cause allergies, are not noticeable during conversation, and only need to be removed for cleaning.
- It is important to fill the absence of front teeth with ceramic dentures.
- Complex defects are eliminated individually. Here the condition of the jaw, the patient’s financial capabilities, and the presence of concomitant diseases will be taken into account.
Included defect in the dentition in the lateral region
Kennedy's classification of dentition defects contains class 3, which is called included edentulous molars in the lateral region. In its characteristics, this type of pathology resembles a unilateral end defect, but is distinguished by the presence of a greater number of complications with the simultaneous loss of several incisors in different areas of the upper or lower jaw. In this case, the mandatory qualifying criterion is that the person is missing the 5th and 6th teeth on the right.
1 subclass
The included dental arch defect in the lateral section of subclass 1 is characterized by edentia of the 5th and 6th teeth on the right and the 6th molar on the left side.
This type of dental pathology is considered simpler in terms of the selection of orthopedic methods for prosthetics of the upper and lower jaw.
2 subclass
The second subclass of included dentition defect in the lateral region is characterized by the complete destruction of 6, 5, 1 and 2 teeth on the right, as well as the loss of the 6th molar on the left side. This type of dental pathology not only leads to disruption of the function of chewing teeth, but also deprives a person of the ability to bite off rough food.
3 subclass
The included dentition defect in the lateral section of subclass 3 is the simultaneous loss of several teeth from the chewing group, as well as molars located in the smile zone. In the presence of such a clinical case, the patient is immediately missing 1, 2, 5 and 6 teeth on the right, as well as 1, 4 and 6 molars on the left side. This defect can be found on the lower or upper jaw.
Methods for eliminating an included defect of the jaw apparatus in the lateral region
Orthopedic treatment of an included defect in the dental arch in the lateral region is aimed at restoring the chewing function of the right or left jaw, depending on which side the adentia is localized.
Installation of a unilateral prosthesis with complex milling and attachment
This method of prosthetics involves replacing areas of the jaw apparatus that lack dentition with a metal-ceramic bridge that imitates the natural color of molars. The edges of the prosthesis are fixed in the area of the root part of healthy teeth, which are located along the edges of the dental defect.
Depending on the general condition of the supporting molars, they can be additionally strengthened with inlays that prevent deformation and destruction of the lateral teeth. This prosthesis must be removed once a day for hygiene procedures. For example, during evening brushing of teeth. After this, the one-sided prosthesis is again installed inside the oral cavity.
Implantation
The implantation procedure is used if the patient has several subclass lateral defects of the dentition, when it is not possible to perform prosthetics of the jaw apparatus using a bridge. In such a situation, it may be necessary to implant one or several implants at once, which will subsequently serve as a lateral support for the installation of a monolithic prosthesis.
The implantation procedure involves carrying out a full-fledged surgical operation to implant a metal structure inside the bone tissue of the patient’s upper or lower jaw. After the titanium rod has been implanted, an implant crown is fixed on its upper edge, which completely imitates a natural human tooth.
The main disadvantage of this procedure is that there is always a risk of developing an acute immune reaction of the body with rejection of a foreign object in the form of a metal structure. The average cost of installing 1 implant is around $700. The implantation procedure itself extends over a long period of time, taking from 3 to 6 months. depending on the complexity of the lateral defect of the dentition.
Patients who have undergone prosthetics using implantation must ensure that there is no hypothermia of the jaw bones and do not allow plaque to form on the surface of the implant crowns. Participation in fights and engaging in contact martial arts is strictly prohibited.
Measures to prevent dental defects
- The main enemy of this pathology is carious teeth. The best remedy in this case is adequate oral hygiene.
- This also applies to children whose first teeth have erupted. Parents should take care to purchase a special toothbrush with soft bristles.
- For any injuries that affect the condition of baby teeth, you should immediately contact a pediatric dentist.
- Adults should not ignore annual visits to the dentist - even if there are no complaints. Professional teeth cleaning can only be done in the office of a specialist.
- Malocclusion and supernumerary teeth also need to be treated on time. Ignoring these defects will only make the situation worse over time.
The classification of the patient's dental defects is carried out by the dentist to select treatment. The number of missing teeth, the health of the remaining units, and the condition of the periodontium are taken into account.
Expert opinion
Biryukov Andrey Anatolievich
doctor implantologist orthopedic surgeon Graduated from Crimean Medical University. Institute in 1991. Specialization in therapeutic, surgical and orthopedic dentistry including implantology and implant prosthetics.
I believe that you can still save a lot on visits to the dentist. Of course I'm talking about dental care. After all, if you carefully care for them, then treatment may indeed not come to pass - it won’t be necessary. Microcracks and small caries on teeth can be removed with regular toothpaste. How? The so-called filling paste. For myself, I highlight Denta Seal. Try it too.
There are laws that allow you to select a prosthesis taking into account the extent and location of the disorder. The classification facilitates communication between dental specialists and simplifies documentation.
When is classification needed?
Any of the classification methods makes it easier for the orthodontist to study partial tooth loss, simplifies documentation, and allows doctors to identify the problem during work. However, the widespread classification is not able to provide guidance on the choice of design and cannot reflect a specific picture of disorders, type of occlusion, or tissue health.
Thanks to systematization, the definition of a defect is accelerated, clarified, and the choice of treatment direction is clarified. If you do not take into account the nature of the pathology, you can harm the functionality of your teeth with improper prosthetics.
Then the loads are distributed unevenly, tissues and teeth are overloaded, causing complications. To exclude the development of events, orthodontists systematized pathologies, dividing them into classes and subclasses.
Parameters that allow you to assign a defect to a specific group:
- defects in the structure of the jaw units coming after the canines;
- anomalies in the structure of incisors and canines;
- pathology of the posterior or anterior part of the arch;
- problems with the outermost teeth of the row.
The most common types of systematization are according to Betelman, Kennedy, Gavrilov. Named after the names of the inventors. Not very popular methods - according to Zhulev, Eichner, Oksman.
The need for classification
Any of the classification methods makes it easier for the orthodontist to study partial tooth loss, simplifies documentation, and allows doctors to identify the problem during work.
However, the widespread classification is not able to provide guidance on the choice of design and cannot reflect a specific picture of disorders, type of occlusion, or tissue health. Thanks to systematization, the definition of a defect is accelerated, clarified, and the choice of treatment direction is clarified. If you do not take into account the nature of the pathology, you can harm the functionality of your teeth with improper prosthetics.
Then the loads are distributed unevenly, tissues and teeth are overloaded, causing complications. To exclude the development of events, orthodontists systematized pathologies, dividing them into classes and subclasses.
Parameters that allow you to assign a defect to a specific group:
- defects in the structure of the jaw units coming after the canines,
- structural anomalies of incisors, canines,
- pathology of the posterior or anterior part of the arch,
- problems with the outermost teeth of the row.
In the 19th century, dentists wanted to develop certain approaches to studying the main types of dental deficiencies and finding the correct and effective types of treatment.
The classification selects the right type of therapy, and also quickly and accurately determines the type of defect. This task is important and complex due to the fact that if the nature of the deviation is ignored, the correct functioning of the dentition after prosthetics can be disrupted.
Often a situation arises where improper orthodontic treatment leads to stress on the dentition and its uneven distribution. Thus, the soft supporting tissues are overloaded and new problems arise.
In order to achieve maximum effect from therapy, dentists have created and classified orthodontic deviations according to classes and subclasses.
Today, the following classifications of dentition defects are applicable in dentistry:
- Gavrilov;
- Kennedy;
- Betelman.
Since the 19th century, many dentists have been puzzled by the issue of creating a certain classification of all the main types of dentition defects in order to develop universal approaches to their study and the selection of correct and effective methods of therapy.
Classification allows you to quickly and more accurately determine the type of defect present and select the optimal way to treat it, for example, the most suitable prosthesis option in a particular case.
This is a very difficult and important task, since if you do not take into account the nature of the deviation, you can, for example, disrupt the normal functioning of the dentition after prosthetics.
It often happens that after poor quality teeth, the load on the teeth is distributed unevenly and they, as well as the supporting soft tissues nearby, are constantly overloaded, which can cause other problems.
To avoid complications and achieve maximum treatment efficiency, prominent dentists have developed and systematized all orthodontic pathologies into classes and subclasses.
The classifications of dentition defects according to Kennedy, Betelman and Gavrilov are most often used in modern dentistry. Systematizations according to Eichner, Zhulev, Oksman and some other doctors are also popular.
Choosing a dental prosthesis is not an easy task - it can make your eyes run wild...
Kennedy classification
American dentist Edward Kennedy was a revolutionary in performing operations designed to eliminate malocclusion. The accumulated experience allowed him in 1921 to develop a classification of the anomalies encountered, identifying 4 classes and 3 subclasses:
- 1 class. Absence of chewing teeth on both sides of the arch. Subclasses distinguish 3 options for the development of the situation. The first - in addition to the absence of molars, one more tooth is missing. Second – molars and teeth are missing in 2 places. The third – apart from the molars, there are no teeth in 3 different places. The main method of treating anomalies of this group is devices with labile fastening;
- 2nd grade. Unilateral defect, loss of distal support. There are 3 subclasses, similar to the previous one. Correction of such defects is carried out with prostheses with palatal fixation (on the side of healthy teeth) and a device with labile fastening (on the area with the defect);
- 3rd grade. Unilateral problem, presence of distal support. The subclasses are the same as above. The optimal prosthesis is a bridge-like removable structure, which is secured with clasps;
- 4th grade. These include clinical situations where the patient does not have front teeth. The problem is eliminated by installing a prosthesis with support clasps.
Subclasses
All of the classes described above, except the last one, also have subclasses that are the same for the three groups:
- the dental unit, in addition to the main one, is missing in one more place;
- no teeth in 2 more places, with the exception of the sides;
- absence of units additional three places, except for the main chewing units located on the sides.
6 effective methods for correcting deep bites
If the dental arch has several defects that belong to different classes, then it is classified into a smaller group. For example, when disorders of the second and third classes are diagnosed in the dentition, the second class is assigned to the arch defect.
There are also many other classifications in dental practice that are less common and not as popular as the Kennedy method. This is explained by the fact that the system he proposed fulfills its main task well, which is to select a more optimal orthodontic design for the treatment of the most common defects of the dentofacial apparatus.
The use of such techniques allows dentists to significantly simplify their work and the life of the patient. In addition, thanks to this method, it becomes possible to choose the most suitable and effective option for attaching the prosthesis used, which allows you to take into account the anatomical features of each patient individually as accurately as possible.
Gavrilov system
E.I. Gavrilov is a Doctor of Medical Sciences, a prominent scientific figure of the Soviet Union. His goal was not only to restore aesthetics to the dentition, but also to restore functionality and distribute the load over all areas of the jaw. The systematization developed by Gavrilov defines a detailed description of the problem, which helps the doctor determine a treatment regimen. The scientist systematized the problems into 7 groups.
Do you feel nervous before visiting the dentist?
Not really
I class. This includes defects on the right and left sides of the end of the dental arch.
Treatment options:
- clasp denture with cast clasps gently acts on the teeth that serve as support;
- removable partial plate denture. There are disadvantages - weak fixation, the likelihood of tipping over while eating due to one-sided load;
- prosthetics with implants - a fixed prosthesis that restores the functionality of the jaws without stress. If there are no contraindications, then this option is considered the best.
II class. This group includes defects when the distal support of one of the jaws is lost. Prosthetic options are selected similarly to the conditions. The bilateral presence of problems at the ends of the jaws ensures fixation of the removable denture, the load is evenly distributed along the row. When choosing designs, they choose a clasp denture when it comes to problems of the upper jaw. Thanks to the metal arc, it is possible to reduce the dimensions of the plate, and the sky remains open.
For conditions belonging to this group, you can choose fixed prosthetics. This method of restoring the functionality of the jaw is acceptable when installing implants. For situations where teeth have long been lost and there has been no treatment, bone deficiency becomes a sign. Technologies make it possible to carry out an operation to increase it. If there are no contraindications and hygiene skills are satisfactory, then prosthetics with implants will be an effective solution to the problem than removable structures.
III class. This group includes defects accompanied by the absence of molars, provided that the extreme molar is preserved.
The dentition can be restored with removable, fixed dentures of the following types:
- removable clasp prosthesis. A good option, but not comfortable. The disadvantages are due to the fact that the structure is removable, and with a one-sided effect it overturns;
- a bridge-like structure, one of the supports of which is fixed on the chewing tooth. This is an inexpensive prosthetic option. The advantages of the method include the reliability of fixation, the disadvantages are the load on the supports. Contraindications to choosing a bridge include periodontal disease and mobility of dental units;
- Implantation occupies a leading position. This method provides maximum comfort and physiology identical to natural. The load on the supporting teeth is eliminated, healthy tissues do not need to be ground down, but chewing and aesthetic functions are completely restored.
IV class. This group includes conditions when the side sections have flaws, but the distal supports are preserved. Options for eliminating the problem are similar to those indicated above, but clasp dentures no longer have any disadvantages, since here the load is evenly distributed over all teeth.
V class. Includes conditions in which several units are missing from the front of the soul. Bridges and removable dentures will help restore the dentition. To ensure reliable fixation, clasps are used. Such fastenings are noticeable on the teeth, so the aesthetics will not be up to par. Considering that we are talking about teeth involved in a smile, this method of treatment should not be preferred. Bridges, if they have strong supports, provide excellent functionality, but they look unsightly, especially if there is a gap between the gum and the neck of the artificial crown.
Unlike previous treatment methods, implants have virtually no disadvantages (except for price). They are able to restore lost aesthetics and chewing function. One-stage implantation becomes preferable, in which the tooth is removed and an artificial root is immediately installed in its place. This allows you to preserve the shape of the gums, the amount of jaw bone tissue, and creates optimal conditions for wound healing. The result obtained in terms of aesthetic indicators has no equal.
VI grade. This includes combined defects. Planning is carried out taking into account the identified problems.
VII class. The last group includes all pathologies in which there is only one tooth left in the mouth.
Systematization according to Gavrilov is used by orthodontists; it allows choosing the optimal design for prosthetics in a wide variety of conditions. Then single teeth were used as support for removable dentures. This practice was widespread in relation to problems of the lower jaw.
Thanks to implantation, there is no longer a need to save a tooth if there is little reason to do so. Implants can become a support for various orthodontic structures in the presence of single teeth or complete edentia.
End defect on one side
Kennedy's classification of dentition defects includes unilateral terminal edentia of the jaw apparatus. In such a clinical case, a patient in need of dental care is missing teeth 7 and 6 on the right side of the upper or lower jaw. This is a classic version of this pathology, which is also further classified into subclasses. The latter type of dental defects is complicated by edentulism in other areas of the masticatory apparatus.
1 subclass
The first subclass of unilateral end defect is characterized by the standard absence of 7 and 6 teeth on the right side of the upper or lower jaw, as well as the loss of 5 and 6 molars on the left side. In this case, complete and partial dentition is observed. In conditions of maintaining the integrity of the crown of the 7th tooth on the left, the task of prosthetics for the left-sided defect of the dental arch is significantly simplified.
2 subclass
A unilateral terminal defect of subclass 2 is expressed by the complete absence of 7 and 6 teeth on the right side of the upper or lower jaw, as well as edentulous 6, 5, 2 and 1 molars on the left side.
Classification of dentition defects according to Kennedy.
The complexity of this dental defect is that its elimination may require the installation of 2 dentures on the left side of the upper or lower jaw, as well as the fixation of 1 right-sided bridge.
3 subclass
The third subclass of unilateral end pathology of the dental arch is characterized by the loss of 7, 6 and 4 teeth on the right side of the upper or lower jaw, as well as the destruction of 1, 2, 5 and 6 molars on the left side. The complexity of this dental adentia lies in the need to fix orthopedic prostheses by turning the crowns of healthy teeth with their further use as a support for installed bridges.
Methods for eliminating end defects on one side
The table below presents the main methods for eliminating unilateral end defects using orthopedic techniques.
| Methods for eliminating one-sided end defects | Description of the orthopedic method |
| Partially removable denture | This method of eliminating a unilateral end defect involves installing a partially removable prosthesis made of acetalic-like plastic. The bridge is fixed using plastic clasps. The advantage of using this prosthesis is that there are no metal elements inside the human oral cavity that can cause a feeling of discomfort. |
| Removable metal prosthesis | This method of getting rid of unilateral edentulous dental arch is a classic option for prosthetics of lateral teeth. The orthopedic structure is made of fire-resistant titanium, and its fastening is carried out using cast clasps. The finished prosthesis is distinguished by its rigid structure and long service life. |
Elimination of a unilateral end defect of the dental arch requires the dentist to have a high level of qualifications, excellent knowledge in the field of parallelometry, accuracy, and attentiveness during dental work.
Betelmann classification
Betelman developed a type of systematization that allows you to select a denture for dental problems. Its classification involves dividing deviations into 2 classes, each with 2 subclasses.
I class. They include conditions when end defects are detected (no molars, starting from the 5th or 6th unit to the end of the jaw). If the problems are localized on one side of the arch, they are classified as subclass I, if on both sides - to subclass II.
II class. This group of dental problems includes the absence of crowns anywhere in the dental arch. There are 2 subclasses:
- Conditions in which 1 or more included defects are detected, with one problem area including up to 3 missing units.
- The presence of 1 or more included defects, and the defect includes more than 3 missing units.
Included defect in the anterior region
An included defect in the anterior part of the dentition of the upper or lower jaw is a type of edentia, which is classified according to the method of orthopedist E. Kennedy as follows:
- the integrity of only 3, 4, 5, 6, 7 teeth of the chewing group on the right side is preserved;
- only molars 3, 4, 5, 6, 7 are present on the left side;
- 1 and 2 teeth are completely missing on the right and left sides.
A distinctive feature of included adentia in the anterior part of the dental arch is that areas of the jaw apparatus with signs of the absence of molars are located in the smile zone. A person with such a dental pathology is deprived of the opportunity to fully bite off rough food; over time, malocclusion occurs, and the reproduction of vowels and consonants occurs.
Methods for eliminating an included defect in the anterior section
The choice of method for eliminating included adentia in the anterior part of the dental arch of the upper and lower jaw depends on the total number of missing incisors. In such a situation, a bridge-like prosthesis is made, the edges of which are placed on top of the lateral molars. In this case, the supporting teeth are ground by a dentist and contribute to reliable fixation of the prosthesis, simulating the front incisors.
Patients with complicated mixed defects need the production of a volumetric bridge, the structure of which is attached to the posterior lateral teeth, and the missing incisors are located on its metal base. Additional attachments are created on other molars of the oral cavity, the structure of which is not damaged by dental diseases. Depending on the complexity of the metal structure, its main part may come into contact with the surface of the mucous membrane of the hard palate.
Zhulev classification
E.N. Zhulev is a professor, representative of the Medical Academy of N. Novgorod. Zhulev will present a systematization of dental problems in 1989. The essence comes down to the distribution of pathologies into 5 groups (classes):
- Pits, depressions, cavities in fissures.
- Pits on the incisors, cavities in the fissures.
- Cavities on the surface of the incisors and lateral teeth.
- Cavities in the gingival, cervical area.
- Combined anomalies, including the symptoms indicated above.
In addition to those listed, there are well-known systematizations of dentition defects, but they are used less frequently.