Causes of denticles
The exact reasons have not yet been established, since this dental phenomenon has not yet been fully studied. It is assumed that the appearance of denticles can be accompanied by various injuries to the dentition, functional inactivity of the tooth, and injuries received during its preparation.
The following factors can provoke the development of mineralized deposits:
- inflammatory processes in the pulp;
- poor quality dental treatment;
- impaired metabolism in the pulp and periodontal tissues;
- age-related changes in tooth and gum tissues;
- endocrine diseases.
Often, the development of denticles is promoted by hormonal disorders, diabetes mellitus, hypertension, severe infectious diseases and lack of minerals.
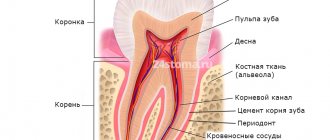
The structure of the dental pulp –
Speaking about the structure of the dental pulp, we will first analyze its structural elements - after which we will move on to a description of its layers, which you could see in Fig. 2. You can see the appearance of the pulp removed from the tooth (wound on a pulp extractor) in the photo below.
Video of tooth pulp removal (pulpectomy) –
1) Structural elements of pulp –
The pulp consists of loose fibrous connective tissue (with a large number of nerve endings, blood and lymphatic vessels). Accordingly, its structure will consist of collagen fibers, the main amorphous substance, as well as a large number of various cellular elements. The total collagen content is from 25 to 30% of the dry mass of the dental pulp, and it is mainly collagen types I and III. In the coronal part of the pulp, collagen fibers are located more loosely, but in its root part they form denser clusters.
As for the main amorphous substance located between the collagen fibers, it consists of water, glycosaminoglycans, as well as glycoproteins and proteoglycans. The intercellular substance has a high ability to diffusion, which allows nutrients from the blood to enter the cellular elements, and metabolic products to be excreted into the venous circulatory system. There is also a wide variety of cellular elements in the pulp - primarily odontoblasts and fibroblasts (fibroblasts are responsible for the formation of intercellular substance and the synthesis of collagen fibrils), as well as dendritic cells, macrophages, lymphocytes, mast cells, etc.
Cellular elements of the pulp -
| Cells | Odontoblasts – form dentin and provide its trophism. Neighboring odontoblasts are interconnected by intercellular connections, which allows the layer of odontoblasts to also perform a barrier function (regulating the movement of molecules and ions between the pulp and predentin). Some authors call these cells “dentinoblasts.” |
| Fibroblasts are the most numerous cells in the pulp (their number decreases with age). Their function is to produce and maintain the composition of the intercellular substance of the pulp, as well as to absorb and digest the components of the intercellular substance. | |
| Macrophages - participate in the renewal of the cellular composition of the pulp, capturing and digesting dead cells and components of the intercellular substance. They phagocytose microorganisms and participate in the development of immune reactions as antigen-presenting effector cells. | |
| Dendritic cells – they are antigen-presenting cells whose function is to absorb various antigens, process them and present them to lymphocytes. They also induce the proliferation of T lymphocytes. The content of dendritic cells increases as the pulp matures, as well as with antigenic stimulation. | |
| T-lymphocytes are contained in the pulp in small quantities, but during inflammation their number increases sharply (of all types of this population of lymphocytes, T-suppressors predominate in the pulp). B-lymphocytes are not normally found in the pulp, and appear only when it is inflamed (they synthesize IgG immunoglobulins and provide humoral immune responses). | |
| Mast cells – they are located around blood vessels; are characterized by the presence in the cytoplasm of a large number of granules with biologically active substances (histamine, heparin, eosinophilic chemotactic factor, etc.). The release of these components causes an increase in vascular permeability. | |
| Poorly differentiated cells - can give rise to odontoblasts and fibroblasts. The content of these cells decreases markedly with age. | |
| Fibers and glycoproteins | Type I and III collagen fibers, reticular fibers, fibronectin. |
| Basic intercellular substance | Glycosaminoglycans, chondroitin, proteoglycan. |
Features of the disease
The denticles themselves do not cause discomfort unless they compress the nerve endings of the pulp. Due to their small size, they can be almost invisible. Sometimes, during development, denticles fuse with each other, then they can be detected on an x-ray. If left untreated, denticles grow uncontrollably and fill the entire pulp chamber, making further dental treatment impossible. Due to such fused formations, root canal treatment becomes problematic, and in such cases the patient is recommended to have the tooth removed.
Features of the course, diagnosis and treatment
The disease is characterized by long-term, sluggish development and the absence of clinical manifestations in the anamnesis. During a dental examination, a change in the coloration of the crown of the tooth may be observed. As the inflammatory process develops, paroxysmal pain appears, more pronounced at night. Mostly, the patient can accurately identify the causative tooth.
Clinical manifestations
In most cases, the formation of denticles is not accompanied by clinical manifestations; they are discovered accidentally during an X-ray examination of the teeth, which is carried out in connection with the treatment of other dental diseases. Painful sensations occur if the nerve bundle is compressed by denticles or petrification, when formations are displaced, as well as during the development of the inflammatory process.
Radiologically, the formations look like multiple or single dense shadows, having a round or irregular shape, located inside the cavity of the tooth and its canals.
Diagnostic features
The clinical manifestations of concremental pulpitis are quite similar to the symptoms of trigeminal neuralgia, so the disease is differentiated from it. The table shows the main differences:
| № | Characteristic | Concrete pulpitis | Neuralgia |
| 1. | Pain | Increasing attack of dull pain | Sudden onset of acute pain |
| 2. | Time of attack | Mostly nocturnal | Any time of day |
| 3. | Novik's test | Pain occurs with sudden changes in position | Negative |
| 4. | Percussion | Sharp pain when tapping on the crown of a tooth | Absent |
| 5. | Causal tooth | Determined | Not determined |
| 6. | X-ray result | Dense formations in the tooth cavity are clearly visible | No tissue changes |
| 7. | Development | The disease develops slowly, in which the intensity and number of attacks constantly increases | Painful attacks are constant and do not change intensity. |
| 8. | Manifestations from the autonomic nervous system | No | Eat |
Treatment method
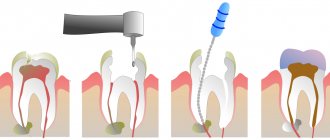
The main stages of treatment for concremental pulpitis are the same as for other types of inflammatory nerve diseases. Thanks to modern techniques and materials, all stages of therapy in most cases take one visit. The general treatment plan for pulpitis is as follows:
- anesthesia;
- preparation of carious cavity and canals;
- instrumental and medicinal treatment;
- obturation (filling with filling material);
- filling a carious cavity.
The differences lie in the complexity of preparing and filling obliterated (deposit-filled) canals with filling material. To pass them through, a special ultrasound device is usually used, but for large stones this does not always lead to a positive result.
The prognosis is favorable; in the absence of a tendency to excessive growth, denticles do not cause problems for the doctor and the patient. Treatment is most often carried out in full, and inflammatory symptoms completely disappear and do not recur.
To avoid the development of complications during treatment, it is necessary to promptly contact the dentist and conduct an examination of the dental system. There is no way to prevent the formation of denticles and petrification, but you can reduce the risk of their occurrence. To do this, it is necessary to treat inflammatory dental diseases in a timely manner, preventing the formation of foci of pulp necrosis, which subsequently mineralize.
Classification of denticles
Depending on their location, denticles are:
- Free (most often found directly in the pulp tissue, in isolation; if dentin is formed intensively, they grow together with the inner walls of the tooth, becoming parietal denticles);
- Adjacent, or interstitial (initially based at the inner walls of the tooth cavity).
Depending on the structure, denticles are divided into two groups:
True denticles are synthesized directly on the pulp tissue. The formations are similar in structure to dentin and have dentinal tubules. They are localized mainly at the top of the root canal. They are quite rare.
False denticles form independently as a result of necrosis of adjacent tissues. They do not have a dentin-like structure and tubules.
Regardless of the type of denticles, it is necessary to get rid of the problem as soon as it was discovered, since this can negatively affect the condition of the pulp of the diseased tooth.
Denticles
Denticles
Denticles (pulp stones, dentinoids, internal odontomas) are dense mineralized areas of the pulp. The size of the formations can vary from barely noticeable foci to bodies 2-3 mm in diameter, which tend to merge and further fill the pulp chamber and root canals. Denticles occur in patients of all ages, including young children. In studies, mineralized areas of the pulp were found in embryos and in the tooth buds of newborns. According to statistics, this phenomenon occurs in 39.9-53.9% of patients visiting a dentist. Moreover, for children under the age of 16 this figure is significantly lower and amounts to 4.4%. Typically, intact teeth that have a worn chewing surface are affected by the pathological process.
Architectonics of dental pulp layers –
In the coronal part of the pulp, there are several layers that differ in their structure and functions - 1) the outer layer, consisting of odontoblasts, 2) the subodontoblastic layer, which in turn consists of several zones, including the Weil and Rinaggio zones, as well as the Rashkov plexus, 3) central pulp zone. Below we will analyze in detail the structural components of each layer.
Architectonics of dental pulp layers (diagram) –
- The outer layer (peripheral) - consists of several layers of odontoblasts, which are elongated cells with basophilic cytoplasm (24stoma.ru). In “young teeth” the pulp may contain 6-8 layers of odontoblasts, but the older a person gets, the fewer the number of layers will be (at least one layer). Odontoblasts are highly differentiated cells that are specific to the dental pulp.
Long processes (the so-called “Toms fibers”) extend from the odontoblasts, which penetrate the dentinal tubules to the entire depth of the dentin. Odontoblasts and their processes play a very important role in the nutrition of the tooth and the delivery of mineral salts to the dentin and to the enamel-dentin border. In addition, they perform the function of dentin synthesis both during the period of tooth development and throughout a person’s life (we are talking about the synthesis of secondary and tertiary dentin). In the root part of the pulp, a layer of odontoblasts is also present, but it is thinner than in the coronal part of the pulp.Odontoblasts are closely connected to each other by strong intercellular connections, but capillary loops penetrate through their layer, as well as the finest nerve fibers (branches from the Rashkov plexus). These nerve fibers form tree-like branches around the odontoblasts - they are often called the “superodontoblastic nerve plexus”. It is interesting that part of the nerve fibers will end around the odontoblasts, but the other part will be directed along with the processes of the odontoblasts into the dentinal tubules.
- Subodontoblastic layer - morphologically it is usually divided into 2 zones.
The first zone is the more superficially located “light Weil zone” (a layer poor in cell nuclei). This zone mainly consists of collagen fibers, as well as cell processes penetrating from the inner zone of the subodontoblastic layer. This layer contains a large number of capillaries, which form an extensive capillary plexus that nourishes both odontoblasts and the pulp as a whole. Also in this layer there are many myelinated and unmyelinated nerve fibers, forming the so-called Rashkov nerve plexus. The deeper zone of the subodontoblastic layer is the Rinagio zone (a zone rich in cellular elements). This zone consists of a large number of diverse cellular elements, for example, poorly differentiated cells are located here, which can give rise to odontoblasts and fibroblasts. In addition, fibroblasts themselves, lymphocytes, as well as capillaries and nerve fibers are located in this layer.
- The central zone of the pulp is a loose fibrous connective tissue rich in cells (primarily fibroblasts and macrophages). Also contains larger blood and lymphatic vessels, and larger bundles of nerve fibers. In the central zone of the pulp, dendritic cells, lymphocytes, plasma cells, mast cells, and blood granulocytes are constantly present in small quantities.
Summary: below, for convenience, we have arranged the structural elements of the pulp layers - in the form of a single table. Once again, we draw your attention to the fact that the intermediate (subodontoblastic) layer is well developed only in the coronal part of the pulp.
| Peripheral layer | Intermediate layer | Central layer | |
| outer zone (Reil) | inner zone (Rinagio) | ||
| – odontoblasts, – Toms’ processes, – capillary loops, – nerve fibers. | – processes of cells of the inner zone of the intermediate layer, – collagen and reticular fibers, – Rashkov’s nerve plexus. | – fibroblasts, – lymphocytes, – preodontoblasts, – poorly differentiated cells, – capillaries, – myelinated and non-myelinated fibers. | – PBST *, – large blood and lymphatic vessels, – bundles of nerve fibers. |
* PBCT is loose fibrous connective tissue.
Histological specimen (dental pulp and peripulpal dentin) –
Where 1 is dentin (where 1a is calcospherites, 1b is predentin). Where 2 is the dental pulp (where 2a is the peripheral layer consisting of odontoblasts, 2b is a cell-poor zone in the intermediate pulp layer, 2c is a cell-rich zone in the intermediate pulp layer, 2d is the central pulp layer).
Ultramicroscopic structure of odontoblast –
Above you can see what an odontoblast looks like with a branched process, which will be located in dentin and predentin (where 1 is dentin, 2 is predentin, 3 is an odontoblast process located in the dentinal tubule, 4 is the Golgi complex, 5 is the nucleus, 6 is mitochondria, 7 – endoplasmic reticulum.).
Differences between the coronal and root parts of the pulp -
The root part of the pulp has significantly weaker vascularization and innervation compared to the coronal part of the pulp. In addition, the cellular composition of the root part of the pulp is much poorer, and the odontoblast layer, even in the “young pulp,” has only 1-2 rows of cells. Apparently, such differences in structure depend on the characteristics (differences) in the supply of nutrients and calcium salts - in the crown and root parts of the tooth.
In the coronal part, dentin and enamel receive nutrients and calcium salts - almost exclusively from the dental pulp. As for the nutrition of the hard tissues of the tooth root, it occurs not only through the pulp, but also due to the process of diffusion of nutrients from the pericement. Therefore, evolutionarily, a decrease in the importance of root pulp in the nutrition of hard tissues of the tooth root has been formed, and its structure has changed.
| Coronal pulp: | Root pulp: |
|
|
Pulp histology: video
Below in video 1 you can see the histology of tooth tissue in stunning resolution. Video 2 is the best lecture on pulp histology you will ever hear. The video is in English, but if you wish, you can turn on subtitles and select translation from English into Russian in the settings.
Features of the structure of the pulp of temporary teeth -
The structure of the pulp in baby teeth differs little from permanent ones. For example, in baby teeth there are fewer differences in the structure of the coronal and root parts of the pulp, and in addition, the pulp in baby teeth is more abundantly supplied with blood. There are also slight differences in the composition of cellular elements and the number of collagen fibers (Fig. 3).