Tooth extrusion – what is this procedure? The essence of the method and indications for its use
Tooth extrusion is a separate dental procedure. Nowadays it is performed quite rarely, but in some clinical cases it is precisely this that makes it possible to preserve the root in case of severe destruction of the visible part of the tooth and subsequently, based on it, restore the crown using modern methods of restoration and prosthetics. Extrusion was first introduced to the world in 1973. The author of the technique was Dr. GS Heithersay, who proposed this procedure as an alternative to removing roots with fractures1. Read more about the essence of this method and how such treatment is carried out further in this article.
What is the essence of the procedure
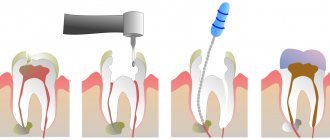
Tooth extrusion is the procedure of pulling a tooth or remaining root out of the gum in a vertical direction. According to this definition, extrusion allows a slight elevation of the root and creates more suitable conditions for a reliable and durable crown restoration. As part of this procedure, the tooth is usually pulled out by 3-4 mm. But to carry it out, it is important that at least the dentinal rim is preserved. Its thickness must be at least 1 mm, and its height must be at least 2 mm. If there is no such rim, the specialist may try to pull it out from under the gum.
Tooth extrusion is a procedure for pulling out a tooth or remaining root from the gum.
This procedure in some cases allows you to avoid root removal and subsequently restore the crown on it. However, if the root is damaged, its complete extraction followed by replacement with an implant will be the best solution. By the way, extrusion promotes the formation of bone tissue, so the procedure can also be performed as an alternative to artificial expansion of the jawbone for subsequent installation of implants.
Skeletal support devices in orthodontics
Moving abnormally located teeth is impossible without ensuring stability of the support. However, in a constantly changing dental system, it is almost impossible to achieve absolute stability, in which reactive forces will not lead to displacement of the selected intraoral support.
The requirements for skeletal (cortical) support in orthodontics are formulated:
- Biocompatibility with oral tissues.
- Easy to install, use and then remove.
- Initial stability.
- Possibility of loading immediately after installation.
- Stability when applying orthodontic forces.
- Small sizes.
- Compatible with orthodontic technology.
Previously, stable support was provided only by the use of extraoral devices - a mask, a facebow with a cervical traction, which required significant cooperation on the part of the patient, continuous wearing, created discomfort for the patient and difficulties in the work of the orthodontist, who was not confident in the patient’s compliance with the recommendations at home.
For several decades, scientists and clinicians have been researching the possibility of using dental implants as a support. However, classic implants can only be installed in the area of missing teeth or in the retromolar area. All this narrows the indications for their use. Nevertheless, the experience and knowledge gained during these studies led to the creation and successful use of microscrews, which have gone through their evolutionary path and are currently used quite widely in orthodontic clinics.
Table No. 1. Evolution of skeletal support devices for orthodontic clinics
Original devices | Direction of change | Modern designs |
| 1. Osseointegrable implants 2. Fixation devices for the maxillofacial area | 1. “Partially (conditionally) integrable” constructions 2. Optimization of screw or plate design | 1. Orthodontic microimplants 2. Mini plates 3. Palatal orthodontic implants |
When talking about orthodontic bone support, many terms are used, such as skeletal support system (SAS), miniscrews, miniimplants, microimplants, temporary orthodontic anchorage devices (TAD). Implantology uses the term “mini-implants” to define the type of temporary implant for a temporary orthopedic structure. The diameter of a simple mini-implant is smaller than a dental one, but larger than an orthodontic one.
The term “skeletal support” includes all types of intraoral support - orthopedic implant, onplant, etc. All orthodontic implants are screw implants, so the term “microscrew implant” is not used. The preferred term for orthodontic screws is microimplant.
In addition, there are onplants - disc-shaped subperiosteal implants coated with hydroxyapatite. They reach 10 mm in diameter of the support platform and 3 mm in height, and are installed under local anesthesia on the distal areas of the hard palate.
Since the appearance of the first microimplant, in the course of studying methods of its use, the number of its varieties has significantly increased, providing for different localization and method of installation, having different designs and materials of manufacture. The most widely used are intraosseous orthodontic microimplants (Fig. 1, 2).
Rice. 1. Significant extrusion d 26.
Rice. 2. Condition after 6 months. application of OMI and intrusion d 26.
There are two types of implants based on the installation method: self-tapping and self-tapping screws. There is no consensus in the literature about which designs are optimal.
In most cases, to install a microimplant, it is enough to use local application or infiltration anesthesia. To install a self-tapping screw, it is necessary to first form a mucosal flap and prepare the bone tissue in the place where it will be installed. The screw cuts its own threads and ensures stability.
This method requires drilling a pilot canal, qualified actions of a dental surgeon, and the availability of appropriate technical support and instruments. Self-tapping screws do not require any bone preparation. Cortical bone perforation and pilot canal creation are more often required in the mandible.
To reduce trauma to the mucous membrane, it is recommended to cut it with a punch. Surgical access through soft tissue and (or) the formation of a mucoperiosteal flap is required in the area of the mobile mucous membrane to avoid injury to it.
Most implants are made of titanium and its alloys; this material has the best combination of characteristics: elasticity, fracture resistance, wear resistance, machinability and, most importantly, bioinertness. There are other options for materials, which may include gold alloys, cobalt-chromium-molybdenum compounds (vitalium), glassy carbon, a combination of ceramics with aluminum oxide, and nickel-chrome-vanadium alloys.
The use of steels makes it possible to produce microimplants with the most aggressive threads, which increases the level of primary stabilization. However, the lack of integration with bone tissue reduces the duration of operation of such microimplants.
According to the manufacturing method, microimplants can be solid or composite (soldered), the latter are less reliable and are susceptible to fracture and cracks. Manufacturers offer about 50 types of microimplants with different head designs (Fig. 3, 4).
Rice. 3. OMI Vektor Tas.
Rice. 4. OMI “Konmet”.
The main developments are in the field of the effect of implants of various designs on the surrounding bone tissue. This is greatly influenced by the quality of the surface, as well as the diameter, shape of the screw and the cutting method. The cylindrical microscrew guarantees tight retention in the bone and resistance to stress; The conical shape of the screw thread provides close contact with surrounding tissue and promotes primary stability.
The combination of these parameters is considered the most effective. The length of microimplants is from 5 to 12 mm, the diameter is from 0.9 to 2.7 mm, and the choice of one or another microscrew depends on the topography of the application site.
The use of orthodontic microimplants (OMI) as a support is possible in two options. Direct support refers to cases where the load directly falls on the AMI when moving or correcting the position of a tooth or group of teeth. With indirect support, the OMI stabilizes the segment of the orthodontic system that interacts with the active elements of the tooth being moved.
Combination with all active elements used in orthodontics, such as round, tetrahedral arches, springs and elastics, modification and addition of other orthodontic devices, and joint use with lingual brace systems allow successful orthodontic treatment in difficult clinical situations (Fig. 5-8 ).
Rice. 5. Application of low vector distal traction.
Rice. 6. OMI “Konmet”, example of mesialization d 47.
Rice. 7. OPTG before mesialization d 47.
Rice. 8. OPTG after mesialization d 47.
More often, skeletal support devices are needed when solving complex orthodontic problems that require particularly reliable support: this is the sagittal and vertical vector of movement in the dental arch of individual groups of teeth (distalization, mesialization, intrusion and extrusion, alignment of dystopic teeth or correction of individual teeth before prosthetics).
The use of OMI is possible during distalization of molars. Works are discussed that illustrate the reduction in the need for tooth extraction when devices based on bone structures are included in the orthodontic treatment plan.
The use of microimplants is justified in the complex treatment of patients with skeletal forms of dentoalveolar anomalies, as an effective support at the presurgical stage, intermaxillary fixation at the surgical and postoperative stages. The use of microimplants has determined the possibility of expanding the indications for orthodontic correction in patients with damage to the supporting tissues of the teeth, with a small number of teeth or serious somatic pathology, such as, for example, connective tissue diseases.
So we can say some obvious conclusions:
- First, the use of orthodontic microimplants can reduce the undesirable impact on the dentition when significant forces are applied over a long period of time.
- Secondly, the risk of using skeletal support devices is comparable to the risk of using traditional dental and extraoral devices, and their ease of use for the patient and the doctor indicates the need for a comprehensive study of their effectiveness in various applications of complex treatment of orthodontic patients.
The list of references is in the editorial office.
Indications for extrusion
As mentioned above, this method is indicated for severe destruction and fracture of the crown of the tooth, as well as for a root fracture, but only if the fracture is in the gum. For reference: according to ICD-10, the root fracture is assigned the number S02.5. Among other indications for the use of this method, dental experts highlight retention. This diagnosis is made when the coronal part does not completely erupt or remains in the gum. This situation is especially typical for wisdom teeth.
“They performed extrusion on me. There was a tooth that was constantly being destroyed. The doctors increased it several times, but it became so dark and chipped all the time. When I once again came to the appointment, they again removed all the composite, they cleaned something there for a long time, and then they said that’s all, I can’t build it up anymore. Instead of removing it, they suggested pulling out the root a little. I agreed. The procedure went well and there was no pain. In the end, they installed a crown, and it’s holding up so far.”
Ira, review on the website www.32top.ru
This procedure can be life-saving if the carious cavity is localized below the gingival level. By removing the affected surface, it is possible to prevent the influence of harmful microorganisms on the mucous membrane and its inflammation.
Traction is also prescribed for retention
Another indication, which was already mentioned above, is insufficient thickness and height of the jaw bone to securely fasten the implant. Extrusion of the tooth root allows you to free up some space between it and the alveolus, which will promote the growth of bone tissue cells and connective epithelium.
Indications for the procedure
Extrusion may be required for a root fracture if the fracture line is located in the gum. Impacted units (those that have not erupted or have not completely erupted), as well as elements with a completely destroyed crown, are also pulled out in this way.
In a number of clinical cases, the procedure is advisable for caries localized below the gum level - by bringing the affected part of the root to the surface, the pathogenic effect of bacteria on periodontal tissue will be reduced.
Another indication for this manipulation is the lack of bone tissue for implantation. Stretching the root and creating free space between it and the alveolus will help stimulate the growth of bone tissue cells and connective epithelium.
Contraindications to the use of the method
Like any other dental procedure, extrusion has its contraindications. For example, it can only be carried out if the adjacent soft tissues and teeth are in satisfactory condition, since they will act as supports for fixing the traction structure.
The procedure will not be possible if the roots are too short or severely curved, and the condition of the canals and crown does not allow the installation of at least one of the elements of the corrective system: ligatures, a button or a pin with a hook.
Therefore, before prescribing extrusion, the doctor must assess the condition and length of the roots, their location. If the patient is diagnosed with an occlusion pathology in which there is no free space for traction, the procedure will not be possible. And one more thing: the method is indicated exclusively for pulpless teeth, so the nerves will first have to be removed if this has not been done previously.
For which patients is extrusion contraindicated?
The procedure is carried out only if the periodontal tissues, as well as the teeth located adjacent to the one that needs extrusion, are in good condition. This is important, since it is on them that the pulling structure will rest.
It will not be possible to carry out extrusion if the patient has severely curved roots of the causative tooth, if the condition of the canals and the coronal part does not allow the installation of one of the elements of the traction system (ligatures and buttons, or a pin with a hook).
Before the procedure, the condition and length of the roots must be assessed - if they are too short, then this is a contraindication. Lack of free space due to bite pathologies or improper occlusion is another reason why doctors will not perform this manipulation.
Important! Extrusion is carried out only on pulpless units, so before the procedure the nerve will definitely have to be removed if this has not been done previously.
Methods of carrying out the procedure
There are two main methods of extrusion. Let's look at each type in a little more detail:
- orthodontic is a more gentle method, which is often combined with correction with a brace system. This method is indicated for impacted teeth, but it requires more time and patience to achieve results. Pulling is carried out by installing an appropriate structure,
- surgical is a rather radical method, which is fraught with serious complications if errors are made on the part of the doctor. But if everything is done correctly, the result can be obtained much faster. The method does not require long-term wearing of the traction system. We will talk further about how extrusion is carried out in this case.
In the meantime, it should be noted that after surgical traction, the patient is given a temporary restoration for the period of tissue and ligament restoration. It allows you to quickly restore aesthetics.
How to Treat Disc Extrusion
Sufficiently small defects, up to 0.5 cm, can be cured using traction of the spinal column and performing therapeutic exercises. For extrusion greater than 0.8 cm, the doctor may prescribe a comprehensive treatment, which includes massage, physiotherapy, and acupuncture. It is possible to use exercise therapy in a gentle manner. There is no need for surgery now.
If the protrusion reaches more than 1.2 cm, special treatment methods are required. In order to correctly choose what and how to treat such a patient, it is imperative to conduct an inpatient examination. This is the only way not to make a mistake with the selection of treatment. First, an attempt is made to cure the disease with conservative therapy, however, if there is no improvement in the patient’s condition, surgical intervention may be performed. Surgery is usually done when a patient has cauda equina syndrome. That is, if the patient is in great pain from compression of the nerve endings, the functions of his legs and pelvis are impaired. Such large extrusions pose a great threat: they can lead to paralysis. It is not worth treating such a patient using outpatient methods.
Conservative methods can only get rid of small extrusions
If the extrusion is localized in the lumbar region, a sick person can be treated in different ways. When selecting treatment, you should look at how severe the disease is. When the size of the protrusion is less than or equal to 0.2 cm and the complete absence of cauda equina syndrome, conservative methods are used. If the protrusion is larger than 0.6 cm, surgery is required.
Conventional treatments for the disease
The first step is to stop the inflammatory processes in the tissues. If necessary, then relieve the pain. After this, the back muscles should be strengthened to form a strong muscle corset. In order to achieve this, physiotherapy and therapeutic exercises are prescribed.
If nerve compression occurs, non-steroidal drugs that relieve inflammation are very popular. With their help, you can relieve inflammation and relieve pain without spending a lot of time.
Preparatory stage
Before the procedure, regardless of the chosen method, it is important to undergo a full diagnostic examination to ensure that the patient has no contraindications. You will need to take an X-ray or undergo a computed tomography scan, and a procedure performed by a prof. hygiene to remove plaque and deposits, as well as remove the nerve from the causative tooth if the crown is preserved and depulpation has not been performed previously.
Before the procedure, the patient should undergo a computed tomography scan
How is extrusion performed using the orthodontic method?
In this case, traction is carried out using a special orthodontic system. Its design includes the following components:
- arch or bracket - one of these parts is fixed on elements adjacent to the causative tooth using a composite or special orthodontic rings. If the patient already has braces, the bracket is not installed;
- a screw or a special pin with hooks is attached to the causative tooth, that is, to the remaining crown. If there is not enough hard tissue for this, the pin is fixed in the root canal using dental cement,
- traction – they combine the above-described structural elements and create a force effect.
The photo shows the surgical method.
The system is fixed under local anesthesia, since to install it the doctor has to cut the fibers that connect the gum to the root. This manipulation is called fibrotomy. Due to this, the specialist gives the root mobility in order to speed up the pulling process and prevent it from returning to its original position.
Features of the orthodontic method
Orthodontic tooth extrusion is carried out using a special structure, which consists of the following elements:
- a bracket or arch that is secured to two adjacent units: it is secured using composite materials or orthodontic rings. If the patient is already undergoing basic orthodontic treatment and is wearing braces at the time of extrusion, then installation of a bracket is not required,
- hook pin or screw: These are attached to the tooth that needs traction. The screw is fixed on the remaining crown, but if this is not possible due to lack of tissue, then a pin is used, cemented in the root canal,
- rubber bands, or rods: they connect the first and second elements of the system to each other and exert a force effect.
The installation procedure must be carried out under local anesthesia, since at the end the doctor performs a dissection of the fibers connecting the gum to the root - fibrotomy. This manipulation allows you to achieve root mobility, speed up the process, and also eliminate the possibility of the root returning to its original position.
Duration of treatment
After installing the traction structure, you will need to visit a doctor once a week to monitor the process and tension of the traction (if necessary). On average, a stretch of 1 mm1 occurs per week. Accordingly, to extend the root by 3–4 mm, you need to make 3–4 visits to the clinic, and you will have to wear the device for about a month.
However, after pulling, the treatment process does not end, since the root and the surrounding ligaments need time to recover - on average, this takes about 2 more months. During this period, a temporary restoration is carried out with removal from the bite (to eliminate the chewing load) and splinting.
Recommendations for the treatment period
It is necessary to carry out oral hygiene not only in the morning and evening, but also after meals. It is better to chew on the side of the jaw opposite to the one where the pulling structure is installed. In case of rubbing of the mucous membrane by the system, it is necessary to use orthodontic wax.
How long does treatment last?
After the procedure, the patient will have to visit the orthodontist once a week so that he can monitor the process and adjust the tension of the rods. Usually, in one week, in this way it is possible to extend the root by about 1 mm. Therefore, to stretch it by 3-4 mm, you need to visit the doctor about 3-4 times, and the process itself can take up to a month.
But the treatment does not end there. It will take some time for the root and ligaments to recover. This process usually takes a couple of months. In the meantime, the patient is undergoing a temporary restoration with the removal of the causative element from the bite and its splinting - this is necessary to relieve the chewing load from it.
Orthodontic extrusion for complex smile rehabilitation
Orthodontic extrusion allows for significant process optimization during periodontal or orthopedic treatment of patients. In some cases, orthodontic extrusion even allows one to avoid soft tissue and bone augmentation procedures.
In this article we will describe a case in which orthodontic intervention allowed the formation of the necessary functional and aesthetic contour for further rehabilitation with the help of dental implants in the area of the central incisors of the upper jaw. The entire treatment process included the implementation of the orthodontic and periodontal phases, extraction, installation of implants and fixation of first temporary and then final restorations. Thus, we were able to achieve not only an aesthetically acceptable result, but also stabilize the position of the gums without compromising the quality of the supporting bone tissue, and improving the overall occlusal pattern.
Case review
A 28-year-old female patient sought dental care due to problems with her maxillary central incisors (Figure 1). After falling off a bicycle, she underwent endodontic treatment with further crowns on teeth 8 and 9. Ultimately, she was unhappy with the appearance of her front teeth and wanted rehabilitation with dental implants. During the diagnosis, it was discovered that these teeth were indeed hopeless for therapeutic treatment, however, additional orthodontic intervention was necessary to install implants. In addition, orthodontic treatment would reduce the level of treatment-associated complications and optimize the achievement of the most acceptable aesthetic results. In the same way, the doctor would be able to reduce the total duration of treatment.
Photo 1. View of the patient’s smile before treatment.
General somatic and dental history
The patient’s general somatic history was not burdened, except for the presence of a previous history of smoking. According to the American Society of Anesthesiologists (ASA) classification, it could be classified as class I. At least one study suggests a correlation between smoking and periodontitis, which should be considered during diagnosis. The patient was also very afraid of any dental procedures, especially anesthesia procedures. Subjectively, she noted sensitivity to temperature stimuli and the possibility of a certain migration of the lower jaw to achieve the position of maximum contact between antagonist teeth.
Diagnosis, risk assessment and prognosis
Periodontal assessment: The patient had not previously visited the dentist regularly and showed signs of periodontal disorders. Thus, in the area of some teeth, a slight loss of periodontal attachment was recorded, recession in the area of teeth No. 3, 6, 10, 13–15, 24 and 29; periodontal pocket 4 mm deep around the 18th tooth and bleeding when probing 11 teeth. The patient's previous smoking habit was considered as a potential risk factor.
Risk of periodontal complications: low (American Academy of Periodontology [AAP] II) Prognosis: moderate to good.
Biomechanical assessment: The patient had active caries in the area of teeth 13 and 29. The crowns in the area of 8 and 9 teeth were defective with signs of secondary caries in their area and traces of chipped ceramics (photo 2). Problematic amalgam fillings were noted in areas 2-4 and 13. A structurally compromised condition was typical for teeth 18 and 31, given the too large size of the ceramic inlays fixed on them. In the area of teeth 8 and 9, the radiograph also showed bone loss and the formation of periapical lesions. The roots of teeth 7 and 10 were inclined mesially.
Risk of biomechanical complications: high. Prognosis: poor for carious-affected teeth 8, 9, 18 and 31; satisfactory for teeth 2 - 4 and 13.
Photo 2. X-ray of area 8 and 9 before treatment.
Functional assessment: Signs of wear were noted in the area of the anterior teeth. In the area of teeth 8 and 9, ceramic chipping was recorded. The patient reported having problems with the temporomandibular joint. During the examination, a range of motion study, loading and immobilization tests were performed. In addition, the patient also noted a migration of mandibular positions to achieve a state of maximum contact between the teeth. All this indicated the presence of occlusal dysfunction in the patient.
Risk of functional complications: moderate. Prognosis: satisfactory.
Assessment of maxillofacial parameters: The position of the lip line, even in a relaxed smile, provoked a significant exposure of the gingival profile. With a full smile, the teeth and gums of the upper and lower jaw were completely visualized (Figure 3). The patient was dissatisfied with the appearance of the crowns on teeth 8 and 9, given the signs of chipped ceramics. She was also concerned about signs of crowding in her lower front teeth. In addition, the patient was informed of the sloping smile line from right to left, which was also noticeable when she smiled. However, this violation of aesthetics did not bother her too much.
Risk of maxillofacial complications: high. Prognosis: bad.
Photo 3. External profile view of the patient with a full smile: excessive exposure of the gum area.
Treatment Goals
The main goal of the treatment was to create adequate space and an optimized aesthetic profile for the placement of dental implants in the area of 8 and 9 teeth. Because the roots of the lateral incisors were mesially inclined, the decision was made to correct this condition orthodontically. Considering that after the removal of teeth 8 and 9, a noticeable loss of the bone tissue supporting them is possible, it was planned to carry out orthodontic extrusion of these teeth, which would allow modifying the appearance of the gingival contour in the frontal area. In addition, controlled orthodontic treatment would also normalize the patient's occlusal pattern, reducing the risk of developing occlusal dysfunction.
Sequence of treatment
Stage 1: orthodontic and periodontal treatment.
The patient underwent scaling and root cleaning procedures with further monitoring of the periodontal condition after 2 months. A follow-up visit was also scheduled after 4 months. The crowns of teeth 8 and 9 were removed and replaced with temporary crowns (Luxatemp, DMG America) using universal composite cement (RelyX Unicem, 3M ESPE). The orthodontic stage of treatment (extrusion of teeth 8 and 9) took approximately 12 months (photo 4). During extrusion, the temporary crowns were adjusted to maintain adequate occlusal relationships. At the same time, the inclination of teeth 7 and 10 was corrected to create at least 1.5 mm of bone space between the roots and the planned position of the implants.
Photo 4. Fixation of braces on provisional crowns to ensure extrusion.
Stage 2: extraction and installation of implants
After achieving the required level of extrusion (photos 5-6), a minimally traumatic extraction of teeth 8 and 9 was performed. The orthodontic treatment allowed us to achieve the formation of an ideal alveolar contour (photo 7). The implants used were Astra Tech OsteoSpeed TX 4.0 SX 11 mm (Dentsply Sirona), which were installed with minimal bone augmentation of the socket using a bone graft (Puros Cortico-Cancellous Particulate Allograft, Zimmer Biomet). Thanks to the modified Essix retainer, it was possible to ensure the installation of implants 4 mm below the free edge of the gums. X-ray data indicated excellent quality of bone tissue in the intervention area. The roots of the extracted teeth were shortened and modified to an ovoid shape - they were fixed along with temporary crowns over the implantation area to maintain an adequate level of soft tissue (Figure 8).
Photo 5. Completion of the extrusion process.
Photo 6. Dynamic contouring of the lingual surface of teeth during extrusion.
Photo 7. Minimally invasive removal of teeth 8 and 9.
Photo 8. Modification of provisional structures over the area of installed implants.
Stage 3: temporary and final restorations
After 8 weeks of healing, the temporary structures fixed to the retainer were removed. The mucosa successfully migrated into the areas between the implants and the overhanging crowns (Figure 9). Next, the screw-retained temporary restorations were secured to the implants (Figure 10) for a period of 4 weeks. Thus, it was possible to more accurately modify the aesthetic profile of the gums, after which the doctor began taking impressions. Milled lithium disilicate structures were used as abutments (photo 11), which were covered with lithium disilcate crowns (e.max, Ivoclar Vivadent) (RelyX Unicem).
Photo 9. Migration of the soft tissue area around provisional restorations.
Photo 10. Provisional crowns with screw fixation.
Photo 11. View of lithium disilicate abutments on the model.
Discussion
Despite the result of the preliminary treatment, thanks to the complex intervention, the doctor was able to achieve not only an aesthetically acceptable appearance of the frontal area of the upper jaw, but also normalization of function and occlusal relationships (photo 12), without compromising either the condition of the gums or the quality of the supporting bone tissue. Thanks to a step-by-step protocol for extrusion and augmentation of the sockets, the doctor was able to ensure that the implants were installed in sufficiently dense surrounding bone tissue. The extrusion procedure also allowed the reconstruction of an adequate soft tissue profile and the required papilla height (Figure 13). This rehabilitation protocol also made it possible to reduce the risk of developing biomechanical complications due to the removal of two problematic teeth, however, the patient still needed to at least treat caries in the area of teeth 13 and 29. Additionally, she was prescribed the use of fluoride gel (CTx4, Carifree). At the time of this writing, large questionable restorations were noted in the area of teeth 18 and 31, although all amalgam fillings had been replaced. This also improved the biomechanical prognosis. The risk of functional complications was reduced due to the normalization of occlusal relationships due to orthodontic treatment. Subjectively, the patient noted the disappearance of the symptom of migration of the lower jaw upon reaching the state of maximum contact of the teeth of the upper and lower jaw. As for the aesthetic parameters, they will remain somewhat compromised, given the high position of the upper lip. Implant-supported restorations provided an appropriate external contour while visualizing the health of the surrounding soft tissue.
Photo 12. View of the final restorations.
Photo 13. View of the patient’s smile after treatment.
Conclusion
In conclusion, it is important to note that the implementation of the three stages of the described treatment protocol was ensured through the collaboration of three different specialists in one clinic (periodontologist, orthodontist and orthopedist). Thus, the number of required visits was reduced to a minimum, while increasing the overall effectiveness of treatment. The financial benefits of such a rehabilitation algorithm, which eliminates the need for soft tissue and bone augmentation, should also be taken into account.
Authors: Scott L. Rice, DDS Taylor S. Rice, DDS Nicolas A. Ravon, DDS, MSD
Expert recommendations during treatment
During the period of traction, orthodontic experts recommend increasing your oral care. You should brush your teeth not only in the morning and evening, but also every time after eating. It is also recommended to chew on the opposite side and try to eliminate any mechanical factors that could interfere with the healing process. If the structural elements rub the mucous membrane, you should resort to orthodontic wax.
Orthodontic wax will help protect the mucous membrane from damage
Features of the surgical procedure
This method is most often used in cases where the crown part of the tooth is so damaged that it can no longer be restored in the classical way, or if it is necessary to re-prosthetize / replace the old restoration material. This procedure can also be performed if the patient wants to get results faster and without the need for temporary “aesthetic loss”.
This operation is not classified as complex, but it requires appropriate experience and skill from a specialist. For pulling, the doctor uses a special scalpel, elevator and forceps. You could say he creates a dislocation and then does not completely remove the root, after which he fixes it with sutures.
The photo shows the surgical method of the procedure
Recommendations after surgery
As mentioned above, after the operation the tooth is covered with a temporary restoration. About a week after surgery, the sutures are removed. Over the next 2-3 weeks, the patient must adhere to a special diet - it is recommended to eat only soft, warm food, not too cold or hot. You will also need to strengthen your oral hygiene and treat soft tissues using an antiseptic solution, for example, Chlorhexidine, as prescribed by your doctor.
To treat the mucous membrane, you can use Chlorhexidine
1.5-3 months after the operation, the root acquires sufficient stability, which allows endodontic treatment and prosthetics to begin. Some experts insist that it is better to install a permanent prosthesis only 1-2 years after traction in order to prevent the development of complications. It will take quite a long time for the periodontal ligaments to fully recover.
How is surgical extrusion performed?
It is advisable to perform surgical extrusion of the tooth when there is not enough hard tissue above the gum for subsequent restoration of the crown, or when it is necessary to re-prosthetize or replace an old composite restoration. Another indication for the procedure is the patient’s reluctance to go the “orthodontic” route, where the treatment process takes longer, and throughout this period one has to endure “aesthetic losses.”
“I had a tooth for many years, which doctors at one time successfully expanded with filling materials, but it had already become dark, was chipping, and I had to think about redoing the work. When I came to the appointment, they removed all the composite, cleaned something for a long time, and then generally upset me, saying that my own tissues were not enough for a second restoration. But you can try to surgically pull out the root to fix it. I agreed to such a measure, because it’s better than deleting it.”
Yana, review from 32top.ru
Root pulling surgery is not considered difficult, but it requires careful attention on the part of the doctor. The procedure is performed using a surgical scalpel, elevators and forceps. The specialist creates an artificial dislocation and incomplete removal of the root, and then fixes it on all sides with sutures.
Possible complications
Unlike the orthodontic method, the surgical method does not involve complete immobilization of the tooth (giving it immobility), since there is a risk of developing a pathology such as ankylosis - complete fusion of the root with the jaw bone.
During the process of root pulling, the specialist must be extremely careful: excessive tissue trauma may subsequently contribute to resorption in the area of the tooth neck.
Duration of treatment
Immediately after surgery, the defective tooth is covered with a temporary restoration. Approximately 7 days after surgery, the sutures are removed. This procedure must be performed extremely carefully, since the connection between the tooth and the soft tissues is not yet good enough, and new bone tissue in the space between the raised root and the alveolus has not yet formed.
For 2-3 weeks after surgery, the patient is prescribed a gentle diet (soft, not too hot and not too cold food), and it is also recommended to carry out thorough oral hygiene and antiseptic treatment of damaged tissues with Chlorhexidine in order to promote their rapid healing and do not cause an inflammatory process.
1.5–3 months after surgery, the root becomes stable, and endodontic treatment and installation of permanent dentures can begin.
On a note! Some researchers argue that prosthetics with permanent structures, in order to avoid complications, is best performed only after 1–2 years after tooth-preserving surgery, since only then are the periodontal ligaments finally restored and the soft tissues acquire complete stability.
How impacted elements are pulled out
Extrusion in this case has its own characteristics. It can be carried out in two different ways, but each of them necessarily includes both surgical and orthodontic stages. These are the two methods:
- delayed - first the doctor dissects the gum and exposes the crown. At the next appointment, 2-3 days later, he attaches a special orthodontic button and rods to the impacted element, after which he installs brackets on the adjacent supporting elements (if there are braces, there is no need for brackets),
- one-step – in one visit, the doctor cuts the gum, fixes the orthodontic system and applies sutures.
With the one-step method, the structure is installed immediately.
During rehabilitation, the specialist prescribes antibiotics and antiseptics to the patient. Again, you will have to adhere to a special diet and exclude any traumatic factors. Pulling in this way can last up to 1 year or even longer.
Pulling out impacted teeth
Extrusion of an impacted tooth is a procedure that has its own characteristics. Modern orthodontics makes it possible to avoid removing such an element if it does not pose a potential danger to its neighbors and there is a place for it on the jaw. Traction can be done in two different ways and always involves two stages - surgical and orthodontic.
The first method is delayed. At the first appointment, the doctor cuts the gum and exposes the crown. At the second appointment, which is scheduled 2-3 days after the operation, an orthodontic button and rods are fixed on the impacted element, and a bracket is installed on the supporting adjacent teeth (if you have braces, it is not needed).
The second method is one-step. The specialist performs both surgery and installation of an orthodontic structure in one visit. This method involves a more extensive surgical intervention followed by suturing the wound.
During the rehabilitation period, the patient is prescribed antibiotics and antiseptics, it is recommended to follow a gentle diet and avoid tissue injury. Pulling out an impacted tooth can take 1 year or more.
Advantages and disadvantages of the method
The main advantage of the method is the ability to preserve the root and subsequently carry out prosthetics based on it. Here is a list of other obvious advantages of this procedure:
- the ability to avoid expensive treatment, for example, prosthetic bridges or implantation,
- the ability to extend the life of a living tooth for up to 5-10 years and even more,
- the ability to avoid traumatic surgery to build bone tissue before installing implants.
The main thing is that an experienced, highly qualified doctor undertakes the treatment, since much here depends on the quality and accuracy of the manipulations performed. If a specialist makes mistakes, they can result in resorption and a decrease in root stability, and the development of ankylosis.
Among the disadvantages, patients highlight the duration of treatment and the inconvenience associated with it. Partly, it is the fact that pulling takes quite a long time, during which you have to adhere to strict dietary restrictions and be careful not to accidentally damage the system. But the result of such a correction can be considered the preservation of a living root, the opportunity to avoid more expensive and, by the way, no less lengthy implantation.
1Persii L.S. Orthodontics. Diagnosis and treatment of dental anomalies: a guide for doctors, 2004.
Types of orthodontic tooth movement
Depending on the direction of the acting force, the movement of the teeth can be inclined-rotational (see Fig. 149,150), body (see Fig. 152), which also includes vertical, i.e. dento-alveolar lengthening or shortening (see Fig. 153-156) and rotational (rotation around the longitudinal axis, see Fig. 157).
One of the most common types of orthodontic movement is oblique-rotational. During this movement, the tooth does not move body-wise, when parallelism with its original longitudinal axis is maintained, and the crown with part of the root tilts in the direction of the acting force, while the apical part of the root moves in the opposite direction. Thus, 4 zones of tissue transformations are formed: two pressure zones (see Fig. 149.6 - zones 1 and 4) and two traction zones (see Fig. 149.6 - zones 2 and 3). This type of movement includes vestibulo-oral tilt (torque or inclination) and mesiodistal (angulation).
With this type of movement, a certain place in the tooth root does not move and rotation occurs around it (see Fig. 150, a - 0). The location of the rotation axis depends on a number of circumstances: the place of application of force to the crown, its clinical height, the magnitude of the acting force, and the anatomical structure of the socket. But most often the axis of rotation is located between the middle and apical third of the root (see Fig. 149, b, c and 150, a). At this point, the periodontal fissure retains its original size, periodontal tissue is not compressed and, therefore, no movement occurs. If you trace from this point “0” (see Fig. 150, a) towards the neck and apex of the tooth to the points of contact of the root with the wall of the socket, then you can clearly see that the degree of compression of the periodontium gradually increases (see Fig. 150, a - 2 and 6).
When studying the topographic relationships of the tooth in the alveolus in a transverse section in the cervical area (see Fig. 150, b), it is clear that the root is in contact with the wall only in a small area (see Fig. 150, b - 1). In adjacent areas (Fig. 150, b - 2) very slight compression of the periodontium can be seen, and at point 0, which is the center of resistance or rotation, it is completely absent.
For the body movement of the tooth, it is necessary to create such a force that its resultant passes through the center of rotation or, at least, in the immediate vicinity of it (Fig. 142,152). The solution to this issue can be twofold: first, move the point of application of force closer to the center of rotation, which is difficult to do directly in relation to the root, but you can lengthen the rigid fastening from the vestibular side of the apparatus used towards the apex of the root, creating a couple of forces; the second is to create, by combining two apparatuses, a pair of oppositely acting forces of equal magnitude. For example, if, during retrusion of a front tooth, a force is applied to any removable apparatus in the cervical area to move it labially, then a second force can be created closer to the cutting edge on the vestibular side, directing the force to the oral side.
Tissue changes during vertical movements of teeth are subject to general laws, namely, when there is a load along the axis of the tooth in the direction of the root apex, bone tissue is resorption at the bottom of the socket, and with the opposite effect - tooth extension - new bone is formed there. It should be noted that during intrusion, it is undesirable to carry out simultaneous extrusion of the neighboring one, since the latter will predominate.
Dental alveolar lengthening (“extension”, extrusion) under the influence of orthodontic appliances is most often planned for the lateral teeth in the treatment of a deep bite or for the anterior teeth in the treatment of an open bite, as well as in the elimination of supra- or infraocclusion of individual teeth. Under the influence of traction force, new bone is built in the area of the crest of the alveolar process (i.e., at the edges of the socket), the bottom of the alveoli (see Fig. 153, 154) and its entire internal surface.
Extrusion of single-, double- and multi-rooted teeth occurs according to the same laws; only in the last two groups of teeth is the formation of new bone at the dome of the interroot septum clearly visible (see Fig. 153, b - IV). In all cases, bone is also formed at the edges of the alveoli. Tissue transformations are identical both during tooth extraction with mechanically operating devices and with functional guides; the difference can only be quantitative. After extrusion, as a rule, minor correction of the gum contours and sometimes the bone socket is required.
Dentoalveolar shortening (immersion, impaction, intrusion) can be straight, purely vertical, or inclined, depending on the point of application of force. The practical application of this type of tooth movement occurs in relation to the anterior teeth when treating a deep bite and in relation to the lateral teeth when correcting an open bite. With increased pressure (the action of the orthodontic apparatus), the periodontium is compressed mainly in the area of the root apex (pressure zone) and less along the rest of the inner surface of the socket, and according to this, bone tissue resorption occurs (Fig. 156).
A special situation is created in the interroot septa, on the surface of which a wide zone of pressure appears and not only their dome, but also the entire surface is resorbed (see Fig. 156, IV). On the frontal histological section in the area of two incisors, one of which was subjected to intrusion (Fig. 155), the septum near the latter was compressed. No changes were noted on the cancellous bone beams lying immediately below the circular ligament, but a small number of osteoclasts were noticeable on the deeper ones. According to the movement of the septum, the periodontal space of the displaced tooth on the traction side was one third wider than that of the neighboring one. The cervical ligament of the tooth being moved is lowered, while that of the symmetrical tooth is elevated.