Concept and reasons for origin
The term “small lower jaw” in dentistry and orthodontics has several interpretations with significant differences:
- Micrognathia (also microgenia) is a pathology manifested in the form of defective or delayed development of the entire lower jaw, as well as its individual fragments;
- Prognathia is an intensive growth of the upper part of the jaw apparatus, which results in the visual effect of insufficient development of the lower jaw.
Both pathologies manifest themselves in both infancy and adulthood. Clinical manifestations of the anomaly make it possible to detect the presence of abnormalities at the primary stages of development, which provides the possibility of preventive treatment.
In children
In infancy, improper formation of the lower jaw is caused by various factors, the main one of which is a violation of the uniform process of fetal development in the prenatal period. At this stage, the relationship of jaw proportions is established, which can be influenced by:
- improper maternal diet;
- presence of genetic predisposition;
- consumption of nicotine and alcohol products;
- exposure to serious illnesses with complications.
In the early stages of a child’s life, factors influencing the development of pathology are:
- late formation of bite;
- metabolic disorders in the body;
- early loss of baby teeth;
- bad habits (pacifiers, pacifiers);
- improper feeding.
The primary signs of small lower jaw syndrome in children are recession of the chin and lower lip, abnormal tooth growth and impaired sucking function. Timely identification of symptoms allows the anomaly to be stopped without the use of orthodontic treatment methods.
In adults
In older age, factors provoking the formation of pathology are:
- incorrect or incomplete treatment in childhood;
- receiving severe injuries to the jaw apparatus;
- disorders of the body's metabolic processes;
- pathologies formed in bone tissue (rickets, ostiomyelitis);
- abnormal development of the orbicularis oris muscle.
Characteristic manifestations of small lower jaw syndrome in adulthood are distortion of the patient’s facial features, deformation of the dentition, and problems with eating solid foods.
Types of dental malocclusion in children
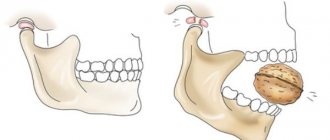
- Distal bite.
The lower jaw is posterior to the upper jaw
- Mesial bite.
Does the child have an incorrect bite, does the lower jaw protrude forward? This kind of bite is called mesial. In this poetic form, we can give a brief description of another common type of jaw disproportion, when the lower jaw is much more developed than the upper.
- Cross or scissor bite.
A less common, but very unpleasant dental anomaly. With a crossbite in a certain place, the jaws close in the opposite relationship - they close in reverse, which is why the dentition resembles scissors.
- Deep bite.
A very common type of malocclusion in children and adults, when the upper teeth cover the lower teeth by more than half.
- Open bite.
One of the most complex anomalies, causing physical and psychological discomfort to the child. The upper and lower rows of teeth cannot meet completely, causing a noticeable gap to form between them.
Above we described what a child’s malocclusion looks like in various manifestations, but we should also briefly talk about the correct one, which can be perceived as a kind of guideline. The ideal bite is considered orthognathic. It is distinguished by an absolutely even dentition without gaps, curvature or crowding, when the upper teeth cover the lower ones by one third. There are several types of correct bite, but if your child has dental defects, this almost always indicates problems.
Treatment and prevention
The choice of treatment technique is determined by the clinical picture of the development of the pathology, as well as the age group to which the patient belongs. The main vector of therapy is to stimulate the development and growth of the lower jaw.
In childhood
The period of primary occlusion is one of the most favorable in terms of correction possibilities, since it allows the use of gentle treatment methods. The main methods used at this stage are:
- prosthetics for prematurely fallen milk teeth, ensuring the preservation of the normal shape of the jaw arch;
- sanitation of the oral cavity, accompanied by the restoration of individual damaged teeth and cleaning of defective roots;
- grinding of the areas of jaw closure - fissures - which allows you to eliminate malocclusion in the form of bumps on the chewing surface;
- normalization of breathing and tongue function, including by trimming the lingual frenulum and correcting the nasal septum;
- use of special corrective trays, plates or nipples.
Quite often, in order to stop the primary signs of pathology, it is enough to wean young children from bad habits.
As an adult
The treatment method during the period of permanent or mixed dentition is determined by the specifics of the anomaly.
To treat prognathia at the variable stage, special corrective orthodontic appliances, such as a Frenkel adjuster, a facebow or a Herbst device, can be used. Microdentia is treated with the help of distractors - devices that stretch the bone tissue and then replace it in the jaw with new bone.
At the permanent stage of occlusion, the most effective method is jaw surgery, which involves removing part of the dentition and excision of the alveolar-ridge area. It is also possible to use a radical technique - plastic surgery, in which the lower jaw is broken off from the main bone and moved forward, and in its place new bone material is placed, fixed with special plates.
The easiest way to avoid orthodontic intervention and stimulate the normal development of the lower jaw is in childhood - to do this, it is enough to follow simple preventive measures, prevent the development of bad habits and contact specialists at the first signs of pathology.
How to determine malocclusion in a child?
“How can you tell if a child has a malocclusion?” - This is a question many parents ask. It is important to understand that only an experienced pediatric orthodontist can make an accurate diagnosis here, so we strongly advise you to undergo regular preventive examinations with this specialist from a very early age until the complete replacement of baby teeth with molars. If the baby teeth are located too closely together, this can also become an additional complication when the molars erupt (the latter take up more space because they are larger). In the case of a small child (under 3 years old), it is difficult to be guided by purely visual principles and determine by eye whether the bite is correct or incorrect. Be that as it may, there are a number of signs that directly or indirectly indicate that the child has prerequisites for orthodontic anomalies.
Improper breathing
The child's mouth is constantly in a half-open position, he does not breathe through his nose (of course, if there are no colds).
Snore
If your baby constantly snores in his sleep, this may also be one of the consequences of the development of malocclusion.
Jaw formation
Pay attention to how the child's jaws are formed. Ideally, there should be no noticeable disproportion between the top and bottom. Additionally, if a child continually pushes their lower jaw forward, this is considered a clear sign of pediatric bite problems.
Postural disorders
If your child has postural and spinal problems, this may affect the development of malocclusions.
Treatment of distal occlusion
The orthodontist faces several important tasks. First, the lower jaw needs to be pushed forward. At the Propricus clinic, the procedure is performed using aligners. They are convenient, can be removed while eating, and are easy to clean. Now you need to close the non-closing of the lateral teeth. A braces system will help with this. The second task is to adapt the size of the upper jaw to the new size of the lower jaw.
To correct a distal bite after braces, you need to install a fixed appliance or a removable plate. When correction with devices is not possible, the doctor resorts to surgical treatment methods. Our clinic has a team of orthodontists and other doctors to correct TMJ dysfunction. We will be happy to give you the smile of your dreams.
Expert of the article you are reading:
Pokrovskaya Natalya Sergeevna
Head of the Department of Orthodontics
Specialization: Invisalign bite correction, neuromuscular diagnostics, pediatric orthodontics.
Need some advice?
Enter your phone number and we will give you a free consultation
I want a consultation
*By making an appointment you consent to the processing of your data
Diagnostics
To determine the cause of the pathology and assess its severity, the orthodontist conducts an examination. During the initial examination, doctors at our clinic evaluate the functioning of the joint, the patient’s posture, and whether nasal breathing is impaired. Analysis of TRG of the skull in the lateral surface reveals all skeletal abnormalities. Using a 3D skull model, you can understand how the teeth and jaws are positioned. By analyzing plaster casts of the jaws, you can find out their size and how the jaws close. All this is needed to understand how to correct a distal bite.
Causes of malocclusion in children
The causes of malocclusion in children can vary, and most of them are difficult to address without orthodontic treatment. Below you can see a list of the key reasons for the occurrence of such anomalies in a child.
Genetics.
If you are wondering why your child has an incorrect bite, look at yourself first. Genetic predisposition is the most obvious and common cause of malocclusion in a child. If one or both parents have pronounced anomalies, then with a very high degree of probability their children will inherit them.
Bad habits.
Children often chew and put into their mouths literally everything they can get their hands on. Often such cravings provoke a violation of the formation and development of teeth. Malocclusion in a child from a pacifier is also quite common.
Breathing problems.
Children with nasal breathing disorders are much more likely to suffer from malocclusion, as experts say.
Problems with the musculoskeletal system.
The spine is the main “bearing structure” of our body, so it is not surprising that the functioning of the musculoskeletal system affects the dental system.
Other diseases.
The risk group (meaning malocclusion) also includes children with diabetes mellitus and central nervous system diseases.
Consequences of distal occlusion
Any violation of facial proportions removes a person’s appearance from the ideal of beauty and reduces his attractiveness. Insufficient development of the lower third of the face, an inexpressive chin, protruding teeth - all this creates an unfavorable impression of a person. In addition to this, other problems develop over time:
- diction suffers;
- the process of chewing food becomes difficult, which negatively affects the functioning of the entire digestive system;
- improper distribution of chewing load reduces the service life of teeth, leads to rapid abrasion of enamel, tooth loss due to inflammatory processes in the periodontium;
- pathological changes in the temporomandibular joints lead to the appearance of clicking sounds when chewing and become one of the causes of frequent headaches;
- If a patient has malocclusion, prosthetics becomes difficult, and the service life of crowns and dentures decreases.
Problems increase gradually, and their presence is not always associated with existing prognathia. However, it is better to think about your health when correction of the distal bite can be carried out as planned.