Why can caries complications occur?
Unfortunately, many people consider caries to be a harmless dental disease and seek help from a dentist only when they experience pain in their teeth. However, the appearance of pain in the tooth area indicates that the development of caries is taking its course, moving from a simple form to more and more severe conditions. According to the depth of the carious process, caries in the spot stage, superficial, medium, acute and chronic deep caries are distinguished - all this refers to uncomplicated forms. But complications arise when the lesion spreads deep into the tooth to the pulp (dental nerve) and bone tissue around it. At this stage, diseases such as acute, retrograde and chronic pulpitis and acute periodontitis, the main complications of caries, arise and progress.
Damage to the pulp or periodontium, as a rule, is a consequence of untimely contact with the dentist or poorly performed earlier filling or prosthetics, the so-called caries under the filling. From the formation of caries in the spot stage to the destruction of the pulp can take from 12 to 18 months, it all depends on the form of the course, that is, it can be acute caries or chronic caries. In any case, when demineralization has passed through the enamel and dentin, an infection enters the cavity of the crown and root canal, causing severe inflammatory and painful processes.
Caries
Classification of caries Dental caries is the most common human disease. Anatomical and physiological characteristics, reactive properties and general resistance of the body in childhood leave their mark on the course of caries. Caries of primary teeth under the age of 2 years is localized mainly on those tooth surfaces that formed in the antenatal period (smooth surfaces of the incisors of the upper and lower jaw), especially if it was unfavorable for the development of the fetus (hypoxia of various etiologies, malnutrition, chronic extragenital diseases of the mother, anemia, toxicosis of pregnancy, etc.). After 3 years, caries affects the chewing surfaces of molars, and after 4 years, the contact surfaces of temporary molars. It should be noted the high incidence of caries on the chewing surface (80.8%) of the first permanent molars. A feature of the carious process is its occurrence during the period of teething (6-7 years - first permanent molars, 11-13 - second permanent molars) and rapid progression due to incomplete mineralization. The largest percentage of the occurrence of initial forms of caries occurs precisely during the period of tooth eruption. An increase in intensity is observed at a later age and is due to the progression of existing foci of initial caries. In accordance with the International Classification of Diseases (ICD-10), the following are distinguished: - By 02.0. Enamel caries. — By 02.1. Dentin caries. — By 02.2. Cement caries. — By 02.3. Suspended dental caries. — By 02.4. Odontoclasia. — By 02.8. Other dental caries. — By 02.9. Dental caries, unspecified. Stain stage (macula cariosa) Focal demineralization of enamel, depending on the nature of the course, is divided into slow and fast-flowing. A differential diagnosis between these forms can be made on the basis of anamnesis, clinical picture (color, size, shape of the lesion), and data from staining of teeth with a methylene blue solution. The clinical picture indicates that demineralization of tooth enamel goes through at least three stages. The early stage is a white spot measuring 1-3 mm. In the 2nd, developed stage, distinctive signs of slow and rapid demineralization of the enamel appear. Slow-flowing demineralization is characterized by uniform changes in the enamel surface: on several teeth one of the stages of development of focal demineralization of the enamel predominates, which suggests the possibility of the simultaneous occurrence of foci of demineralization. The rapid demineralization of enamel in the 2nd stage is characterized by the activity of the process. Foci of demineralization lose clear boundaries, their edges become blurred. The enamel surface is rough, matte. The probe easily gets stuck in the demineralization area. The enamel loses its density and is easily scraped off with an excavator. The intensity of staining is on average 60 points. Increased staining is associated with an increase in enamel porosity. Rapid demineralization moves into the 3rd stage - the defect stage. At this stage, characteristic signs for both forms of damage are also noted. Summarizing the above, G. N. Pakhomov et al. propose the following classification of dental lesions with focal demineralization. Focal demineralization of tooth enamel: 1. Slow: - initial stage; - developed stage; — stage of the defect. 2. Fast-flowing: - initial stage; - developed stage; — stage of the defect. In children who frequently consumed sweets, the slow-moving form of enamel demineralization was 1.7 times more common and the fast-moving form was 3.5 times more common than in children who consumed sweets in moderation. After removing plaque from the entire surface of the tooth, an area of dull white or pigmented (from gray to black) enamel is discovered; the surface is smooth, sometimes rough, but painless and dense. Lesion in the stain stage on the vestibular and cervical surfaces of the tooth most often appears in children with the third degree of caries activity on a large group of teeth, up to the defeat of all teeth. It can occur in children of any age. The slow-onset form of enamel demineralization most often affected the incisors of the upper jaw (54.9%). In 2nd place in terms of the frequency of detection of a cervical slow process was the group of lower incisors (17.9%), followed by the group of small molars of the lower (8.7%) and upper (6.7%) jaws. Foci of rapid demineralization of enamel were more common on the upper incisors (45.8%) than on the lower jaw (21.5%). The canines of the upper (7.2%) and lower (7.4%) jaws, as well as the small molars of the upper (9.1%) and lower (9%) jaws were affected equally. Superficial caries (caries superficialis) . It is characterized by softening of the affected enamel, which is removed with a little effort by an excavator. Most children at this stage do not complain. Some of them indicate pain from sweets and sours, and children 1-3 years old refuse sour fruits. Upon examination, an enamel defect is detected, usually round in shape. When the process is chronic, its edges are flat, and when it is acute, they are steep. Exposure to cold and chemical irritants is often painful. Average caries (caries media) . Depending on the activity of the process and age, average caries has some clinical differences. In children 1-3 years old: in most cases it is very active, but they still cannot localize their sensations and express them, so average caries is detected during preventive examinations of children by a dentist, less often by parents. A feature of the clinical course of caries in children is the so-called planar form of caries, when the process of tissue demineralization spreads faster over the surface of the tooth than in depth. Occasionally, planar, slow-moving caries does not progress without treatment, but “stabilizes.” The affected enamel is erased when chewing, the exposed dentin has a color from light yellow to dark brown, dense, shiny, painless when probing. This form is called arrested caries. It is most often found on the chewing surfaces of the first temporary molars in children 4-7 years old. The slow progression of caries in children is observed relatively rarely: carious dentin is brown, dry, and difficult to remove with an excavator in the form of scales; at the bottom of the cavity the dentin is dense and often pigmented. In preschoolers and schoolchildren, there is an intermediate course, when both decalcification and pigmentation of carious tissues are moderately expressed. Deep caries (caries profunda) In temporary and permanent teeth with incomplete root formation, this form of pathology practically does not occur. Due to the morphofunctional characteristics of dentin and pulp, deep destruction of dentin is always accompanied by pronounced reactive and dystrophic changes in the pulp. These changes, under the influence of irritations caused by the treatment of the carious cavity with a drill and medications, easily turn into inflammation and necrosis. Each case of deep destruction of tooth dentin should be thoroughly examined using clinical (response to temperature stimuli, probing, percussion, etc.), electrodiagnostic and radiological research methods. During the active course of caries in children aged 1.5-3 years, replacement dentin is practically not formed, the dentin of the bottom of the carious cavity is deeply infected, there are changes in the pulp characteristic of developing forms of chronic pulpitis or pulp necrosis, even in the absence of complaints from the child on the day of the visit doctor In the differential diagnosis of deep caries and complicated caries, it is necessary to take into account the anatomical features of the teeth. The process is most active in children aged 1-3 years, when the activity of the pulp is reduced, there is little functional ability to produce replacement dentin, and the protective properties of the pulp are minimal. The process progresses rapidly, causing in most cases complicated forms of caries. In relation to permanent teeth, the diagnosis of deep caries is justified for any activity of the process. With regard to primary teeth, this diagnosis is made with great caution, mainly in older preschool children and in cases of compensated caries. Temporary teeth are smaller than permanent teeth and their enamel layer is thinner. When determining a carious cavity, i.e. proximity of the pulp, it is necessary to take into account the group affiliation of the teeth, their size, the age of the child, and the location of the cavity. For example, on the contact surface of the lower incisors in children 2-3 years old, a cavity with a depth of 1 mm is considered deep, and in schoolchildren 12-15 years old on the chewing surface of the molars, a cavity with a depth of 3-3.5 mm can be considered medium. With active caries, not only is there no or almost no replacement dentin, but also the protective sclerosis in the dentin of the cavity bottom is weakly expressed. Dentinal tubules remain wide, the cytoplasmic processes of odontoblasts are destroyed, the tubules are filled with mixed bacterial flora, therefore, irreversible changes in the pulp of temporary teeth often occur in shallow carious cavities. Despite the fact that caries in temporary teeth develops in accordance with the same patterns as in permanent teeth, the clinic identifies a number of features in the manifestation of the main symptoms of the pathology. These features, in turn, are determined by the degree of maturity of the tooth in which caries develops, as well as risk factors predisposing to a certain localization of the carious cavity, the intensity of destruction of tooth tissue, pulp reaction, etc. As already noted, the main feature of the carious process in children is the rapid course of the pathological process. Children more often than adults experience acute, or “blooming” caries (CC), which in a short time (from several weeks to 3 months) can completely destroy the tooth crown. “Blooming” caries is an acute carious process that affects many or all erupted teeth, quickly destroys coronal tissues, often localized on surfaces that are usually not susceptible to caries, with early involvement of the dental pulp in the process. In one recent study, individuals with active CD were defined as having 5 or more new carious lesions per year. "Blooming" caries usually affects primary teeth in the order of their eruption, with the exception of temporary incisors on the lower jaw. These teeth are likely to be resistant to caries because they are in close proximity to the submandibular salivary glands, which secrete secretions, and because of the cleansing action of the tongue during pacifier sucking. The first carious lesions are usually found on the labial surface of the maxillary incisors near the gingival margin as an area of whitish decalcification or softening on the enamel surface shortly after their eruption. These lesions quickly become pigmented and acquire a light yellow color; within a short time they reach the proximal surfaces and the cutting edge of the incisors. Less commonly, areas of decalcification may initially be localized on the palatal surfaces, and in some extreme cases even near the incisal edges of the incisors. As the process progresses, it often spreads around the circumference of the tooth, leading to pathological fracture of the crown with minimal trauma. Gradually, other teeth are involved, namely the first and second primary molars and, ultimately, the canines. Blooming caries can also affect permanent teeth due to children's tendency to frequently consume cariogenic breakfasts and sugary drinks between meals. Typical “blooming” caries in adolescents is characterized by carious lesions of the buccal and lingual surfaces of molars (buccal and lingual caries), the proximal and labial surfaces of the mandibular incisors (proximal and labial caries). A specific form of “blooming” caries can develop in children and adolescents whose saliva production has significantly decreased under the influence of radiotherapy undertaken to treat cancer in the head and neck area, or due to surgical excision of tumors in the oral cavity. In such patients, fillings fall out soon after treatment, teeth are often covered with plaque, saliva is viscous and scant. Children suffering from acute dental caries have a history of acute infectious diseases, chronic concomitant diseases - rheumatism, chronic tonsillitis, etc., and a tendency to colds. A dental examination reveals caries damage to a large number of teeth, often exceeding 12-14. All groups of teeth are affected, including the canines and lower incisors, which are usually resistant to caries. As with acute caries, symmetrical teeth are often affected. Acute (“blooming”) caries is characterized by a multiplicity of carious defects (up to 3-4 defects on the crown of each affected tooth). So-called “bottle” caries develops quickly in a group of children when they are bottle-fed at night. Usually occurs in 2.5-15% of children. It is characterized by rapid damage to the anterior teeth of the upper jaw, which later spreads to the chewing teeth of both jaws. Due to late eruption, canines are less affected than first molars. “Bottle” dental caries is typical for all socio-economic groups of the population and is often an indicator of the social level of the family. The same system for the occurrence of caries with indiscriminate and prolonged breastfeeding. The cause of this pathology is prolonged exposure to a cariogenic substrate, which comes into contact with the vestibular surface of the upper anterior teeth for 8 hours. In addition, at night there is a low level of salivation and a reduced buffer capacity of saliva. The peculiarity of the course of acute caries manifests itself at different depths of the defect. Thus, initial caries in its most acute form is characterized by the formation of a dirty gray spot (spots) or area(s) of enamel clouding with unclear contours. Such lesions are usually detected by a painful reaction when exposed to mechanical, temperature or chemical stimuli. In case of superficial caries, when the defect is localized in the enamel or reaches the enamel-dentin junction, the enamel appears heterogeneous, fragile, brittle; such defects are usually extensive, with uneven edges, as the process quickly spreads in breadth, along the plane. This picture is especially often observed in temporary teeth, with a characteristic cervical localization, encircling the neck of the tooth. In such cases they talk about “circular” caries . In the most acute cases of superficial caries, there may be complaints of pain associated with eating sweet, sour, and salty foods. When such a defect is localized on the approximal surface, as with other forms of caries, complaints about food getting stuck come to the fore. In the most acute course of moderate caries, a cavity (cavities) with uneven contours, undermined edges, formed by brittle whitish enamel is discovered. Usually there are complaints of pain from chemical, temperature irritants, and when localized on the proximal surface - of food getting stuck. In the most acute cases of moderate caries, there may be complaints not only about the effects of cold. Sometimes pain occurs from hot foods, which may be due to the involvement of the pulp in the chronic inflammatory process. Deep damage to primary teeth in the most acute course of caries has to be diagnosed extremely rarely, since the progression of the process is complicated relatively early by inflammation of the pulp. A detailed diagnosis, reflecting both the depth of the lesion and the nature of the course of caries, is the basis for complex treatment and is of great importance for the practical use of preventive means. Complications of caries Without timely and proper treatment, caries can develop into more severe forms of tooth disease (pulpitis, periodontitis) and lead to tooth loss.
How dangerous is caries in its advanced state?
So why is advanced caries so dangerous? Firstly, dental treatment in most cases will involve surgery, and any operation is always a risk: the risk of poor-quality treatment, the risk of swelling and other undesirable consequences. Secondly, serious exacerbations of caries will certainly affect your general well-being due to constant pain, which will be concentrated not only in the tooth area, but throughout the entire jaw, in the temples, ears and eyes, swelling of the gums and a sharp increase in temperature are also possible.
If caries is not treated and the pain is tolerated, the nerve of the tooth dies on its own and starts the process of decay in the carious cavity. The infection begins to penetrate deeper tissues, causing irreparable damage. The body begins to fight inflammation on its own, forming a granuloma around the tooth root, which can later increase in size and transform into a cyst. As you can see, the consequences of caries can be different, but one thing is clear - they are all serious and can have a significant impact on human health.
INTRODUCTION
Effective treatment of dental caries continues to be one of the most important problems in practical dentistry. Unfortunately, domestic dentistry cannot yet boast of any special achievements in this area.
We analyzed the long-term results of “free” treatment of dental caries in a number of municipal dental institutions, in which, despite the widespread development of paid dental care, the vast majority of the population is treated. The quality of fillings was assessed according to the following generally accepted criteria:
1. Anatomical shape.
2. Edge fit.
3. “Recurrent” caries.
4. Condition of the contact point (for cavities of class II according to Black). It was found that when using traditional methods and filling materials, after six months approximately 30% of the fillings did not meet the requirements, after a year - more than 50%, after two years - about 70% of the examined fillings (Fig. 1). Moreover, these indicators did not differ significantly for cement, plastic, metal and composite fillings (Fig. 2).
We noted that fillings made from amalgam and composites were more likely to have a violation of the marginal seal with the development of “recurrent” caries, as well as caries in the fissures located next to the filling. In our opinion, this is due to a violation of the technique of preparing carious cavities and a deviation from the rules for using filling material.
Fillings made of cements and plastics, as a rule, did not meet the requirements for 3-4 positions at once, which indicates their low clinical value. We believe that there are several reasons for this low effectiveness of treatment.
Firstly, when preparing carious cavities, there is widespread adherence to the principle of “biological expediency” by I.G. Lukomsky, formulated by the author in the 40-50s of the 20th century, as opposed to the “non-physiological”, “bourgeois” principle of “preventive expansion” of Black. It must be recalled that the principle of “biological expediency” is based on the so-called. “biological” theory of caries by I.G. Lukomsky, according to which carious lesions of the enamel arise as a result of dysfunction of odontoblasts caused by endogenous factors. According to this theory, relapse and further progression of carious lesions depend on the condition of the dental pulp, and the quality of the applied filling does not affect this process. The “biological” theory was quickly recognized as untenable, but the method of preparing carious cavities became established and became widespread. This was also facilitated by objective reasons: the lack of tools and drills that allow the formation of a cavity quickly, efficiently and painlessly; lack of time for the doctor, who is placed within strict limits by the standards of “production” (20-30 minutes per patient - 25 U ET per day). Our experience shows that under such conditions it is almost impossible to effectively treat caries. In addition, standards for the treatment of dental caries have not yet been developed and the doctor’s responsibility for the quality of the treatment is almost completely absent.
At the same time, we want to immediately warn dentists against thoughtless, formulaic use of Black’s “preventive expansion” method, since it is not without its drawbacks, which will be discussed below.
The second reason for the low effectiveness of caries treatment is a violation of the regimes for preparing carious cavities and non-compliance with the rules for carrying out the preparation stages. In some cases, the doctor allows the hard tissues of the tooth to overheat during preparation without cooling, which leads to necrosis of the enamel around the filling. Often, in an effort to preserve hard tissue as much as possible, the dentist leaves infected, non-viable enamel and dentin. For the same reason, as a rule, additional support platforms and retention points are not formed. And the stage of finishing the edges of the enamel is not even described in some manuals.
The third reason is the widespread use, especially in budgetary medical institutions, of filling materials with unsatisfactory physical and chemical properties and, first of all, silicophosphate cements (Fig. 3).
What to do if complications have already occurred?
First of all, seek help from a dentist and do not put off visiting him for a day, even if you have already developed caries and are determined to have a tooth removed! Any tooth damaged by caries is a source of infection, which can spread to any area in the oral cavity, trachea or esophagus and cause a number of other diseases. In addition, the sooner you see a doctor, the greater the likelihood that the tooth can be saved.
If the clinic has modern materials and equipment important in the treatment of periodontitis and the treatment of pulpitis, you can count on a high-quality procedure. In particular, diseases such as advanced periodontitis and periostitis can also be cured, but only surgically. In general, traditional treatment consists of removing the nerve, thoroughly cleaning the canals and filling it. However, after such manipulations the tooth becomes more fragile. And do not forget that with the transition to a more complicated stage of caries, the price of its treatment also increases.
How does caries manifest on the front teeth?
Caries on the front teeth most often appears on the enamel surface, but in older people or people with periodontal disease, the exposed surfaces of the tooth roots are also where the disease develops.
Symptoms:
- Whitish matte spots, initial carious lesion (white spot lesion, incipient lesion). Due to plaque on smooth surfaces, as well as the frequent location on proximal surfaces (when interdental caries of the anterior teeth develops), only a dentist can determine the initial stage of development of the disease. The surface layer of enamel at the site of a carious lesion loses mineralization, the enamel becomes weaker by 1-10%.
- Formation of a carious cavity due to demineralization of the enamel with subsequent infiltration of bacteria deep into the dentin.
- Unpleasant sensations. The tooth reacts with pain to cold, hot, sweet or sour foods. The tongue can feel a change in the surface of the tooth (it can be injured). Food particles and floss get stuck.
Prevention of caries complications
Having encountered such a problem at least once, most likely, you will no longer want to exhaust your body with toothache and shell out decent sums for complex treatment. Therefore, you should not neglect preventive measures: visit the dentist once every six months and carry out hygienic cleaning. If, nevertheless, a hole has formed in the tooth and it becomes ill, you should choose a doctor with extreme caution. Remember that the result of poor treatment will be a more serious complication of caries, which may require surgery, and, worse, tooth extraction. In addition, complicated caries requires more expensive treatment than its initial formations.
Agree, you never thought that such harmless caries can cause serious consequences, including tooth extraction. Now think about what is cheaper, faster and more painless - going to the dentist for an appointment twice a year or postponing this moment for several years, then heading straight to the dentist’s office? It’s up to you to decide, of course, but life is given to enjoy joyful moments, and not to endure toothache. And dentists are ready to help us with this!
Stages of caries on the front teeth
Caries on the front teeth develops in the following stages.
Spot stage
If you examine a stain after removing plaque using a dental probe, the roughness of the surface is noted, and when the probe is advanced, smoothness is noted. If you look at a section of a tooth under a polarizing microscope, a significant lack of minerals and an increase in the volume of enamel pores from 5 to 25% are found directly in the affected area. The components of saliva, water and proteins (protein elements) penetrate into these pores.
Initial stage of caries
Superficial caries
Over time, due to the penetration of foreign substances into the enamel, the stain darkens, but intensive cleaning cannot return the color. A carious cavity gradually forms, without affecting the dentin, since the surface layer of enamel at the site of a carious lesion is characterized by a loss of inorganic substances, reaching 1-10%.
Average caries
Caries spreads deeper. On an x-ray, the cavity exceeds half the thickness of the enamel, but does not yet affect the dentin. The rate of destruction of the dental crown at this stage slows down somewhat, since the so-called opaque (dark layer) of enamel is located here. Pores occupy almost 2-4% of it, they are small, because remineralization processes take place here. The tooth tries to recover on its own.
Deep caries
Destroys dentin, passing through the enamel-dentin border and spreading along the dentinal tubules towards the pulp. Dental pulp and dentin have their own protective mechanism. In dentin, sclerotization of the tubules begins, the processes of odontoblasts move away, and replacement irregular dentin is formed at the dentin-pulp boundary. The inflammatory process in the pulp, a reaction to the penetration of bacteria, is also a protective mechanism. If short-term pain occurs when eating cold food, it may be deep caries.
If we talk about caries of the roots of the front teeth (more often found on the canines than on the incisors), then the protective mechanism of the tooth works differently. The bare root surface, which has been exposed to the microbial-bacterial environment of the oral cavity for a long time, is covered with a thin layer of root cement. Strengthening (demineralization) of both the cement and the underlying enamel occurs, and the dentin becomes sclerotic. There are fewer dentinal tubules at the root, so the process proceeds more slowly and is initially shallow. However, over time, caries covers increasingly larger root surfaces.
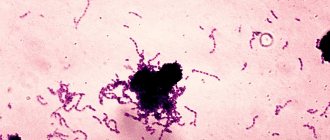
The composition of plaque on root surfaces differs from the composition of the enamel surface; Aktmomyces fungus is especially common here.
Diagnostics
Whether it will be painful to treat caries on a front tooth depends on the degree of damage. To diagnose it use:
- Fluorescent radiation. Due to the uneven reflection (the carious spot does not glow), the presence of the disease can be determined. The method is suitable for preventive examination.
- Vital staining with a mixture of methylene blue (1%) and red (0.5%) solutions. A carious stain is colored differently than healthy dental tissue. The method is cheap, it also allows you to identify areas of caries, but it is not used for prescribing treatment, because does not show the depth of the carious cavity.
- Electroodontometry. Check the condition of the pulp using an electric current.
- X-ray. The image shows the depth of destruction and the protective reaction of the tooth. The most accurate method by which treatment is prescribed in the most severe cases.