Causes
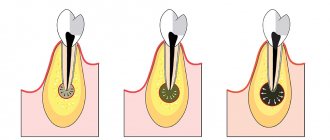
A cystic formation in the form of a capsule isolating the inflammatory focus develops against the background of the following diseases:
– pulpitis, periodontitis;
– extensive carious lesions;
– respiratory tract infections (otitis media, inflammation of the maxillary sinuses, tonsillitis);
– weakened immunity;
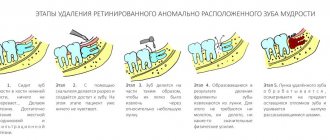
– difficult teething;
– bite defects;
– chronic stomatitis;
– cracks, chips of tooth enamel, mechanical injuries to teeth.
Cyst of the nasopalatine (incisive) canal
The nasopalatine canal cyst (incisive canal cyst) was first described by Meyer in 1914. These incisive canal cysts (nasopalatine duct cysts) are non-tumor cysts that arise from degeneration of the nasopalatine ducts. The ducts are usually obliterated in utero. Persistence of the ductal epithelium leads to the formation of a cyst. The structure of the epithelial lining of the nasopalatine canal is not the same. Closer to the nasal cavity, the epithelium of the canal is cylindrical or ciliated; the section of the canal adjacent to the oral cavity is lined with flat epithelium. In connection with these features of the epithelial lining of the nasopalatine canal, the structure of the cyst shell depends on its location. If the cyst is located closer to the nasal cavity, its shell is lined with columnar or ciliated epithelium, and the cysts of the lower parts of the canal contain a lining of stratified squamous epithelium. The reasons that cause the proliferation of quiescent ectopic epithelial remnants are still unknown. Another assumption about the pathogenesis of incisive canal cysts is that they arise due to retention of the excretory ducts of the minor salivary glands located in the nasopalatine canal. This is the most common type of non-odontogenic cyst, which is observed only in the mid-frontal sections of the upper jaw.
It is most often found in the 4th to 6th decades of life (45-50 years), more often in men, and occurs in approximately 1% of the population.
Cysts of the incisive canal grow slowly, painlessly, rarely reaching large sizes. They usually appear after the destruction of the palatine bone in the form of a hemispherical elastic protrusion located along the midline of the bony palate behind the central incisors. Sometimes cysts are first discovered during suppuration, and then their clinical appearance resembles a palatal abscess. Patients may have nothing to complain about or complain of swelling of the hard palate, sometimes pain; if the neurovascular bundle is involved in the pathological process, parasthesia may occur in the papilla incisiva area. When growing in the vestibular direction, the cyst can cause tooth resorption and displacement.
When examining the oral cavity in the anterior part of the palate, a painless round-shaped formation with clear boundaries can be determined in its middle. On palpation o. The central incisors of the jaw are, as a rule, intact, the electrical excitability of the pulp is within normal limits. An X-ray examination reveals a rounded loss of bone tissue in the area of the incisive foramen. The contours of the periodontal gap of the central incisors are preserved. Instead of a normal incisive foramen, a center of clearing of the bone tissue of an oval or round shape is found, located in the midline. The incisive canal cyst, unlike the odontogenic cyst, is located strictly in the midline. If it is projected onto the roots of the teeth, then in these cases the periodontal gap of the tooth can always be detected against the background of clearing of the bone. A cyst should be defined as an expansion of the incisive foramen of more than 0.6 cm. Cysts of the incisive canal must be distinguished from radicular cysts of the upper central incisors. The decisive diagnostic method is CBCT examination.
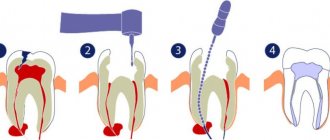
Treatment of incisive canal cysts is surgical.
Clinical case
A 46-year-old woman came for a preventive examination. History of chronic slowly progressive generalized periodontitis in adults. No complaints. On the OPTG, a rounded area of radiolucency with clear boundaries was noted, 1.4 cm in diameter in the projection of the roots of the 1.2, 1.1, 2.1, 2.2 teeth. The EDI of the above teeth is 3-5 μA, the teeth are intact, percussion is painless, physiological mobility was determined. Further, differential diagnosis was carried out with the following diseases: nasopalatine canal cyst, enlarged nasopalatine canal, giant cell granuloma, follicular cyst of the supernumerary tooth, primordial cyst, nasoalveolar cyst. A CBCT examination was performed, which made it possible to diagnose a nasopalatine (incisive) canal cyst.
The patient, under local anesthesia, underwent enucleation of the cyst using a palatal approach, into the bone defect with xenogeneic osteoforming material Bio-oss under the Biomatrix collagen membrane. The cyst shell was sent for histological examination, which confirmed the diagnosis.
Photo report of the work
Removal of retention cyst of the lower lip, local anesthesia
A retention cyst of the lower lip is a benign formation formed from a minor salivary gland with a blocked duct. Such a cyst may form outside the gland, but the contents of the cyst will be the same, and its walls will consist of epithelial tissue. What can cause such a pathology and why is it dangerous? Small salivary glands are found in large numbers on the mucous membrane of the oral cavity, in particular on the inside of the lower lip. When biting your lip or as a result of another injury or inflammatory process, the gland duct can be blocked - temporarily or permanently. The saliva produced by the gland will accumulate, forming a cyst with liquid contents. Often, in addition to saliva, the cyst contains blood that has entered the cavity as a result of hemorrhage caused by injury. Temporary blockage occurs as a result of tissue swelling, and after 10-15 days the cyst caused by such blockage will resolve without a trace. If the duct is completely blocked (for example, during the epithelization of an injured area of the lip), such a cyst will increase in size, and at first it will simply interfere during conversation and eating. As it increases, it will begin to create aesthetic discomfort; the contents of the cyst may begin to decompose, causing suppuration, which may result in pain and additional swelling. In some cases, such cysts periodically break through, their contents flow out, but when the site of the break becomes overgrown, the liquid begins to accumulate again, and the process becomes chronic, threatening not only the expansion of the inflammation zone, but also infection with further complications. If the cyst does not break through, it can increasingly increase in size, as a result of which it is increasingly injured; inside it, the process of tissue degeneration into malignant can begin. The risk of malignant degeneration of the cyst is especially high in people who smoke or have a hereditary predisposition to cancer. Therefore, if during the first 15 days after the initial injury the newly formed cyst has not resolved, doctors most often recommend removing it surgically to avoid further complications. It is extremely important to find a competent and experienced doctor who, at any stage of development of the pathology, will determine the degree of danger of the cyst and carry out treatment in the safest and most effective way.
After an initial survey and examination, the doctor may prescribe the patient an ultrasound and probing of the salivary gland canals, as well as puncture of the cyst to obtain a sample of its contents and conduct a histological examination. Sialography may also be prescribed to obtain information about the condition of the salivary glands, the stage of development of the cyst (also called mucocele) and to identify or exclude an oncological process. If, as a result of research, a malignant component of the formation is excluded, the doctor proceeds to prepare for its removal. As with any other surgical procedure, the patient must refrain from drinking alcohol before removing a cyst; If the patient is taking any medications that reduce blood clotting, it is necessary to consult with the doctor who prescribed them regarding the advisability of temporarily discontinuing them. The procedure itself is not very painful, so it is performed under local anesthesia. The doctor can use either a regular scalpel or a laser, radio frequency or ultrasound method of performing surgical procedures. The doctor decides which removal method to choose based on the condition of the cyst, its location, inaccessibility and other information. After the anesthesia begins to take effect, the doctor pulls back the lip, allowing the most convenient access to the cyst. Since it is extremely difficult to fix the lip in a comfortable position, as a rule, the doctor’s assistant holds the lip while performing all manipulations. Next, the doctor makes several incisions along the edges of the formation so that the cyst shell can be completely separated from healthy tissue. Then the doctor completely removes the contents, washes the resulting wound and applies stitches.
After the operation is completed, the doctor gives the patient the necessary recommendations regarding wound care. If the sutures are not made of self-absorbable threads, the patient will need to return after the time specified by the doctor to have the sutures removed. You need to understand that the lips - and their inner part too - are an area with a large number of nerve endings. Therefore, after the anesthesia wears off, after the operation is completed, at first the patient may experience discomfort in the operated area. This is natural, and if the patient conscientiously follows medical instructions regarding the care of the wound and oral cavity during the rehabilitation period, he will soon be able to forget about the cyst and completely return to a full, healthy life.
In the multidisciplinary clinic “Medistar”, only highly qualified specialists, experienced and qualified professionals in their field practice medicine, who have performed a huge number of successfully performed operations of varying degrees of complexity. Modern technical equipment and our own laboratory allow you to go the entire way - from diagnosis to complete treatment - within our medical center, without leaving it in search of any procedures or diagnostic methods.