The Medikastom dental clinic provides caries treatment in Moscow at a professional level, offering affordable prices, first-class service and high quality services. The qualifications of our specialists, modern techniques and innovative technologies allow us to treat caries at any stage and invariably achieve a positive result. We will help you maintain healthy teeth and provide prompt treatment of caries even at night, as well as on weekends and holidays - the Medikastom dental clinic is open 24/7.
Different types of caries: WHO classification
Caries is a slowly occurring pathological process in hard dental tissues, which develops under the influence of unfavorable external and internal factors. According to statistics, this disease occurs in more than 90% of people in the world.
In this article
- Different types of caries: WHO classification
- How does dental caries develop in the root area?
- Features of the progression of dental caries
- Dental cement caries - main clinical manifestations
- Diagnosis of cement caries: basic and additional methods
- Treatment of cement caries: main stages
- Prevention of root caries
According to the classification of the World Health Organization, there are several types of caries: enamel, dentin, cement, as well as suspended, other, unspecified caries, and odontoplasia. In this article we will talk about dental cement caries, better known as tooth root caries.
Doctor's tactics in the presence of root caries
L. A. Lobovkina
Candidate of Medical Sciences, Head of the Treatment and Prevention Department of Branch No. 6 of the Federal State Institution “GVKG named after. N. N. Burdenko" Ministry of Defense of the Russian Federation
A. M. Romanov
Candidate of Medical Sciences, Chief Physician of the Implamed Clinic (Moscow)
Tooth root caries is the result of the interaction of a complex of unfavorable factors leading to the emergence and progression of the demineralization process in the area of the tooth root. Root caries is a serious problem for dentists, as it can minimize the chances of success of therapeutic treatment of a tooth, lead to complications such as fracture of the crown of the tooth, the rapid development of endodontic complications, etc. The tendency for the circular spread of the pathological process can significantly complicate the surgical and restorative treatment of root caries. Ultimately, it is this localization of carious lesions that most often leads to tooth loss [9].
The most typical localization of root caries is in areas of the dentition with low salivary clearance (that is, less well washed by saliva). In the frontal part of the dentition, the exposed buccal surfaces of the roots of the upper incisors are more susceptible to root caries; in the lateral group, the molars of the lower jaw are more susceptible [9].
According to WHO expert forecasts, the problem of tooth root caries among the population of older age groups is steadily growing (Tkachenko O., 2014). The increase in the prevalence of root caries among the population of older age groups is due to an increase in average life expectancy, poor oral hygiene, a lack of effective methods for preventing gum recession, a high incidence of periodontal diseases, etc. [4]. Thus, the critical depth of the periodontal pocket for the occurrence of this nosology is a distance of 2-4 mm from the gingival margin [2].
RJ Billings identifies 3 groups of main risk factors for root caries:
1. biological factors (composition of dental plaque, level of salivary secretion, salivary pH, salivary buffer capacity, hereditary factors);
2. behavioral factors (hygienic behavior, general health awareness, eating habits, socio-cultural behavior, psychological awareness);
3. individual factors (general health, problems of mobility, coordination, understanding, periodontal treatment performed, functional disorders).
However, the key risk factor in the occurrence of root caries is not the amount of plaque, but its qualitative characteristics. While Streptococcus mutans dominates in the microbiological ratio when tooth crown caries occurs, actinomycetes (Actinomyces viscosus, Actinomyces naeslandii, Actinomyces species) predominate in root caries [3, 11].
Features of the development of root caries and its treatment are reduced tissue mineralization, proximity of the pulp, difficulties in preparation and selection of filling material [10]. Consequently, the main task in the treatment of root caries is the competent selection of rational filling material and correct restoration of the root shape, ensuring good hygiene.
In accordance with the principle of minimal intervention, it is advisable to treat a carious stain without a defect in the hard tissues of the tooth, if possible, without filling [4]. It is recommended to use fluoride-containing products in combination with careful regular individual and professional oral hygiene. If there is a defect in the hard tissues of the tooth, surgical treatment is performed.
Very often, during consultations, doctors work only with composite materials, although in some cases their use is unjustified. Despite their high mechanical strength, abrasion resistance, aesthetics and good adaptation to cavity walls, they have a number of disadvantages, including polymerization shrinkage and deformation of large-volume fillings over time, insufficient biocompatibility with hard dental tissues, lack of cariesstatic effect, high cost [ 8].
Glass ionomer cements (GIC) can be alternative materials in a number of clinical situations [5].
The undeniable advantages of the GIC are [6, 7]:
1. Formation of a strong chemical bond with the hard tissues of the tooth.
2. Bioactivity, cariesstatic and antibacterial effect.
The cariesstatic effect is achieved largely due to the prolonged release of fluoride from the cement mass. This process begins immediately after filling and continues for at least one year. Diffusion of fluorine into surrounding tissues causes increased mineralization and promotes the formation of fluorapatites in enamel and dentin. This leads to increased acid resistance and decreased dentin permeability, worsening living conditions for pathogenic microorganisms and preventing the development of recurrent caries.
3. A low modulus of elasticity provides high elasticity, which allows GIC to withstand occlusal loads under fillings and crowns, help compensate for polymerization shrinkage of composite materials, and also eliminate stresses that arise in the cervical region during microbending of the tooth during chewing.
4. The coefficient of thermal expansion of GIC is close to the coefficient of thermal expansion of tooth tissue, which is important for ensuring long-term tightness at the filling/tooth tissue interface.
However, glass ionomer cements also have the disadvantage of high opacity, which does not allow obtaining highly aesthetic restorations when using GIC alone. In this regard, companies producing dental materials are looking for ways to improve GICs, including increasing their aesthetics.
One of such GIC is “Ionolux” (VOCO, Germany), the peculiarity of which is that it combines glass ionomer and composite parts, which determine its excellent properties. Thus, due to the composite component, its aesthetic qualities have improved, the possibility of immediate finishing has become possible immediately after polymerization, the formation of a chemical bond with composites and very low solubility in water have been noted.
Unlike analogues, when working with Ionolux, there is no need for adhesive preparation of hard dental tissues (for example, there is no stage of priming of hard tissues, which is mandatory for some similar materials from other manufacturers), since it is a self-adhesive cement. It is well known that the more curing mechanisms GIC has, the less fluoride ions it releases into surrounding tissues. However, in terms of the release of fluoride ions, Ionolux is not inferior to classical GIC, which is especially valuable in children's and gerontological appointments.
Clinical case
Patient G., 59 years old, complained of an aesthetic defect and pain in the area of 2.2 and 2.3 teeth under the influence of chemical and temperature stimuli (Fig. 1).
Rice. 1. Initial clinical situation: teeth 2.2 and 2.3 - cement caries.
The patient was offered restoration of teeth 2.2 and 2.3, to which she agreed. It was also recommended to undergo orthopedic treatment due to the absence of a large number of teeth.
The preliminary stages included professional, individual oral hygiene, discussion with the patient of the features of the restoration and mutual responsibility for the results of the work.
The choice of color shade was preceded by mechanical cleansing of the vestibular surface of the tooth, symmetrical to the one being restored, and adjacent teeth using a brush and fluoride-free paste (for example, Klint, VOCO, Germany). Next, the color was selected by comparing the color scale included in the set of materials with the shade of the teeth. When performing this stage, the conditions of the optimal light-color environment were observed.
After anesthesia, preparation of defects in teeth 2.2 and 2.3 was carried out with pear-shaped and spherical burs. To ensure a smooth transition of the material, a bevel of the enamel was created towards the cutting edge using fine-grained flame-shaped burs (with red or yellow stripes) (Fig. 2).
Rice. 2. Teeth 2.2. and 2.3 after preparation.
For medicinal treatment of the formed cavities, a 2% solution of chlorhexidine was used. Then Ionolux glass ionomer cement was introduced into the cavity as a base liner (Fig. 3).
Rice. 3. Tooth 2.3: glass ionomer cement “Ionolux” was added.
Next, adhesive preparation of hard dental tissues was carried out, including conditioning the enamel with Vococid gel (35% orthophosphoric acid) and applying the self-etching bond Futurabond HP (VOCO, Germany). The superstable emulsion of nanoparticles contained in Futurabond HP, obtained using the patented Sol-gel technology, allows the material to be applied in only one layer and photopolymerizes for 10 seconds, which ensures extreme adhesion strength and ease of use. A special feature of Futurabond HP is that it releases fluorides, which prevent the development of secondary caries.
It is currently believed that self-etching adhesives are ideal for the restoration of cervical defects in dental hard tissues [3,4]. The fact is that over time, hypermineralization (dentin sclerosis) occurs in the area of the bottom of the defect, leading to the closure of the lumen of the dentinal tubules with mineral crystals, making it difficult for adhesive systems to access these areas. The use of self-etching adhesive systems makes it possible to transform the smear layer and simultaneously decalcify the surface layer in the defect area in combination with preliminary etching of the bevel boundaries with phosphoric acid.
We used Admira as a restoration system»
(VOCO, Germany) - material based on ORMOCERL®. This system includes the Admira microhybrid composite material, the Admira Flow fluid composite and the 5th generation Admira Bond dentino-enamel bond. However, if in a conventional composite the polymer matrix is only organic and shrinks during the polymerization process, then in the Admira material the matrix is inorganic-organic: its basis is an inorganic frame based on silicon oxide. This modification of the resin leads to the fact that after polymerization, almost all of the residual monomer is retained on the side chains, and is not in a free state, as in conventional composites. Therefore, “Admira” is the most biocompatible material, that is, the risk of developing allergic reactions, especially from the gingival margin, is minimized. In addition, this matrix is more wear-resistant.
Currently, a new material from VOCO based on one ceramic is being registered in Russia - «
Admira Fusion
»
(Admira Fusion). Thanks to the innovative combination of already proven nanohybrid technology with ORMOCER® technology, silica forms the chemical basis for both the filler and the resin matrix. This one-of-a-kind Nano-ORMOCER® technology offers a number of advantages, namely high filler content, extremely low polymerization shrinkage and very low shrinkage stress (polymerization shrinkage and polymerization stress levels are more than 50% lower compared to conventional composites). At the same time, “Admira Fusion” is distinguished by very high stability of color tone. The particle conversion rate of the material reaches 95-99%, which is almost the same as that of composites used for indirect restorations (Robert A. Lowe, 2016).
The restoration of tooth 2.2 was carried out similarly (Fig. 4).
Rice. 4. Teeth 2.2 and 2.3: final appearance after restoration.
Finishing of the restorations was carried out using the Safe End system (SSWHITE, USA), which includes carbide 10-, 20- and 32-point tungsten carbide burs. The 10-blade bur is used to remove excess material and contour the restoration. The 20-blade bur provides a smooth surface ready for polishing. Burs effectively remove composite material while preserving as much hard tooth tissue as possible. Unlike other systems, these burs have different lengths, specially adapted to the type of tooth and the area being treated. The tapered shape of Safe End burs is ideal for treating the transition between the composite material and the enamel surface. These burs are easy to clean before disinfection due to the straight blade shape.
In addition, carbide finishing burs have advantages over finely dispersed diamond ones:
- they work selectively (“distinguish” the softer composite from the harder enamel, allowing the natural tooth structures to be preserved);
- have a cutting rather than a grinding mechanism of action, that is, they remove material in the form of chips, which provides a smoother surface compared to diamond burs;
- They have a rounded tip, which allows treatment without trauma to the marginal edge of the gums and the circular ligament.
In order to reduce the marginal permeability of the root surface and to add shine to restorations, it is recommended to coat them with Easy Glaze filled light-curing varnish (VOCO, Germany).
Thus, for the treatment of root caries and filling subgingival defects, it is recommended to use glass ionomer cements, which ensure good adherence of the material to the root surface and isolation of dentin from external cariogenic factors. I would like to note the high efficiency of treatment of root caries using glass ionomer cement “Ionolux” both in the “sandwich” technique and independently in comparison with composite materials.
Literature
- Alimsky A.V. Gerontostomatology: present and prospects // Dentistry for everyone. - 1999, No. 1. - P. 29-31.
- Grudyanov A.I. Periodontology. Selected lectures. - M.: Dentistry, 1997.
- Grudyanov A.I., Chepurkova O.A. Root caries // Institute of Dentistry. - 2003, No. 4. - P. 87-90.
- Dedova L.N., Kandrukevich O.V. Root caries: clinical picture, diagnosis, treatment. Educational and methodological manual. - Minsk: BSMU, 2013.
- Dmitrieva L. A., Borisova E. N. Dental health of elderly and senile people depending on social status. — Moscow, Final Trade Board of the Russian Ministry of Health. Exhibition “Medicine - achievements and prospects”. - March 22-23, 2004.
- Mount G. J. Adhesion of glass ionomer cements // DentArt. - 2003, No. 2. - P. 17-22.
- Mount G. J., Ngo Hien. Bioactivity of glass ionomer cements // DentArt. - 2003, No. 4. - P. 28-33.
- Nikolaev A.I., Tsepov L.M. Practical therapeutic dentistry. - M.: MEDpress-inform, 2007.
- Solovyova A. M. Root caries and the role of fluoride prophylaxis in its prevention and treatment // New in dentistry. - 2011, No. 3. - P. 36-37.
- Schmidseder D. Aesthetic dentistry. Atlas of dentistry. - M.: MEDpress-inform, 2004.
- Nyvad B., ten Cate GM, Fejerskov O. Microradiography of experimental root surfasce caries in situ. G.Dent. Res 1997;78;12:1845–1853.
How does dental caries develop in the root area?
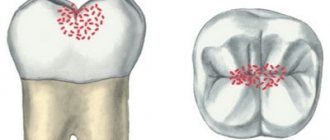
A tooth consists of a visible crown, neck and root. The crown is the visible part that is located above the gum. The neck is located lower and covered with soft gum tissue. The area where the root, or cementum, of the tooth is located is the alveoli (the depressions in the upper and lower jaws).
Root caries can develop as an independent dental disease or as a complication of cervical caries. It is considered more dangerous for the tooth because it reaches the pulp faster. With cement caries, the lesion is usually located under the gum, it is not noticeable during external examination, and therefore is more difficult to diagnose.
The main cause of root caries is usually inflammation or gum disease. With this pathology, the gum does not adhere tightly enough to the tooth, resulting in the formation of a periodontal pocket where food debris and plaque accumulate. Gradually it hardens and turns into tartar, which provokes carious lesions.
Other risk factors for developing root caries are:
- cariogenic bacteria in dental plaque are one of the leading risk factors that leads to periodontal diseases (the tissues surrounding the tooth) and, as a result, exposure of the root surface;
- carbohydrate foods that serve as a breeding ground for bacteria;
- insufficient intake of fluoride into the body;
- impaired characteristics of saliva;
- insufficient oral hygiene;
- features of the anatomy of the dental system;
- critical pH (approximately 6.2 - 6.7);
- cervical caries, which gradually moves to the tooth root;
- violation of crown installation technology, as a result of which the gums recede and expose the root.
Some researchers also name low resistance of teeth to carious lesions, endocrine diseases, and diseases of the gastrointestinal tract as possible risk factors for root caries.
Deep root caries is usually called elderly caries because it most often develops in people over 45-50 years of age. This is due to age-related changes in the oral cavity, decreased immunity, and loss of hygiene skills. Together, this leads to the active proliferation of microbes in the oral cavity, which provoke carious lesions of the tooth root.
Treatment of deep tooth root caries
Patients who were not lucky enough to receive such a diagnosis want to know: is it possible to treat tooth root caries and what is done to eliminate tooth root caries? The answer to the first question: yes, this disease can and should be treated. On the second, treatment tactics depend on what stage the pathological process is at, how many units it has affected and at what speed it develops. To ensure that the measures taken give the best result, CELT dentists take into account the condition of the patient’s oral cavity, as well as the presence of concomitant diseases.
Remineralization
This method can only be used at an early stage of caries development. It is aimed at influencing cement and dentin with preparations that contain sodium or tin fluoride, or calcium preparations, as well as antiseptics. They are used during applications to stop the pathological process due to the remineralization of dental tissues. In the vast majority of cases, the technique gives good results, since the porous structure of the cement absorbs drugs well.
Preparation
If the diagnosis reveals damage to hard tissues and a violation of the boundary between cement and dentin, the following measures are taken:
- Local anesthesia;
- Opening a carious lesion;
- Preparation of healthy dentin (practice with rapid progression of the disease);
- Careful removal of softened dentin tissue;
- Formation of a cavity for filling;
- Carrying out filling with a material that is not susceptible to moisture.
The latter is due to the fact that the filling area is located near the gum and the gingival fluid can destroy the normal material. The patient may receive a recommendation to visit a dental surgeon: the latter will perform an intervention and cover the exposed root with a gum flap. This is important because cement effectively protected by gum tissue will not be susceptible to the negative effects of bacteria and acids.
After treatment, the patient needs to regularly and correctly carry out oral hygiene measures. They will eliminate the risk of relapse of the disease and the development of secondary caries around the cavity that was filled. You should not only brush your teeth, but also use dental floss twice a day after meals. In addition, it is recommended to rinse your mouth with alkaline mineral water after consuming sweets, including fruits.
Features of the progression of dental caries
In the area of cement, caries can occur in different ways, and on this basis it is classified into 4 types:
- progressive;
- rapidly progressive;
- remission;
- relapse.
Progressive root caries is characterized by a relatively slow rate of tooth root destruction. With rapidly progressing lesions, the lesion spreads in depth and breadth at high speed. The remission stage is when root cement caries does not progress. Relapse suggests that root caries develops along the edges of a previously placed filling.
Stage 3: Dentin caries
The third stage of dental caries is known as dentin caries. This occurs when tooth decay spreads through the enamel onto the dentin. Dentin is the part of the tooth that is located between the enamel and pulp. When caries reaches dentin, it spreads quickly because dentin is softer and less mineralized than enamel. When enough subsurface enamel is weakened due to loss of calcium and phosphate minerals, the enamel breaks down and a dental cavity is formed, which can be visible to the eye. To avoid dentin decay, a dental filling will likely be needed to restore the tooth, but this must occur before decay reaches the dentin layer.
Dental cement caries - main clinical manifestations
At an early stage, there may be no symptoms of cement caries at all, making early diagnosis difficult. When a cavity grows, the following symptoms may appear:
- Discomfort while eating.
With root caries, mobility of the damaged tooth is often observed, which causes discomfort while eating. In addition, minor pain can result from food particles getting into the gum pocket or directly into the carious cavity.
- External defects.
If caries spreads from the root upward to the cervical area, during the examination the dentist may detect visible changes in the color and structure of the tooth.
- Pain.
It can appear when the tooth is exposed to cold or hot, or when eating salty, sweet, or sour foods. It is impossible to detect root caries on your own, so you need to visit the dentist twice a year. This is especially important for older people and those with gum disease. In such patients, root caries and deep caries are quite common.
Clinic and diagnosis of enamel caries
The difficulty in diagnosing initial enamel caries in the spot stage is that the patient does not experience any discomfort - the tooth reacts normally to changes in temperature, sweet, sour and salty foods and only in rare cases, for example, if enamel caries develops in the area of the sensitive neck of the tooth, mild discomfort is possible. Visually, enamel caries can appear as a white spot or a small cavity. The tooth surface in the affected area may become slightly rough.
One of the most insidious clinical cases of enamel caries is lesions in the interdental spaces. Since this area is hidden from view, pathology can often only be detected at a later stage.
What complicates the diagnosis of enamel caries is that damage to tooth enamel is not always caries. Fluorosis, erosion, abrasion of enamel and hypoplasia have similar symptoms. For example, both fluorosis and hypoplasia are accompanied by white spots or roughness on the enamel.
Types of diagnostics
- Visual examination
in the clinic using drying - this allows you to detect a rough surface on smooth enamel. - Diagnosis
of caries on tooth enamel using dyes: a quick and easy way to determine whether a patient is developing caries - or if it is just pigmentation. The fact is that with initial caries, tissue softening occurs in the enamel, and if the lesion is carious in nature, the dye will easily penetrate into the affected tissue and color it. With fluorosis or hypoplasia, staining will not occur. - Fluorescent diagnostics:
exposure of teeth to special ultraviolet lamps, during which healthy tissue begins to glow with a bluish or greenish light, but in the area affected by carious bacteria there is no similar effect. The method is quite accurate, but expensive.
Diagnosis of cement caries: basic and additional methods
Diagnostic methods that help identify dental caries are divided into basic and additional.
The main ones include:
- patient interview;
- external visual inspection;
- probing - determining the depth of the cavity, as well as the density and tenderness of tissues, using a dental probe;
- percussion (tapping on the tooth).
Additional diagnostic methods are:
- staining with a special dye to see the affected areas;
- thermal test - the tooth is irrigated with cold water and the pain reaction is assessed;
- radiography - helps to detect hidden carious cavities and caries of contact surfaces;
- electroodontometry - prescribed to determine the condition of the pulp;
- luminescent method - illumination of teeth with ultraviolet rays, under which tissues affected by caries change their shade.
Root caries itself is most often diagnosed through sequential manipulations:
- remove deposits from under the gums using ultrasonic and manual instruments;
- isolate the tooth root from saliva using a special plate;
- using a probe, assess the condition of the root surface;
- with the help of x-rays or radiovisiography, even small defects under the gum, in the gingival zone, and carious lesions at any stage are detected;
- if necessary, confirm the diagnosis of “cemental caries” or differentiate it from pulpitis, thermometry or electrical odontometry is prescribed.
For your information …
Oral diseases are dangerous because they can occur with complications and ultimately lead to a deterioration in the health of the body as a whole. The most common and well-known diseases are gum disease and caries. Gingivitis (lat. gingivitis) - inflammation of the gingiv (gums) and caries (lat. caries dentis) of teeth most often owe their occurrence to facultative microflora (microbial deposits, bacterial processes), which manifests itself with inappropriate oral hygiene. Pathological processes (complications of the initial stages of diseases) can be caused by exogenous and endogenous factors of the state of the body as a whole. Exogenous (external) causes are viral or infectious diseases that result in a weakened immune system. Endogenous (internal) causes are chronic diseases of internal organs or hormonally caused changes in the body (pregnancy), which result in hormonal imbalance, metabolic disorders, etc. An important role is played by the structure of the jaw system and dentition (bite), as well as hereditary predisposition.
Treatment of cement caries: main stages
With root caries, the most difficult task is to gain access to the affected area, especially if the carious lesion is located under the gum. Traditionally, treatment of root caries takes place in several stages:
- Retraction. First, the dentist artificially exposes the neck of the tooth and part of the root, lowering the gums with special devices.
- Coagulation of the gums. It is carried out if indicated using laser exposure to gum tissue. The essence of the manipulation is to remove overgrown tissue.
- Direct treatment of caries. The choice of tactics depends on the degree and depth of the lesion. If caries is in the initial stage of the stain, then remineralizing therapy will be sufficient - restoring the mineral composition of tissues with the help of fluoride preparations. If the doctor reveals more extensive and deep caries with the formation of a cavity, then surgical treatment with preparation and filling will be required.
- Installation of an inlay or crown if the volume of destroyed tissue is more than 50%.
It is necessary to treat cement caries only in a trusted clinic with a reliable specialist, since violation of treatment technology and the use of low-quality materials can cause secondary caries, provoke the development of infection and inflammation of the gums, and lead to tooth loss.
The effectiveness of non-invasive treatment methods
If the damage caused to the tooth is insignificant, and the enamel is sufficiently dense, treatment of enamel caries in the white spot stage can be carried out without preparation and filling. In this case, the affected area is ground and polished, which avoids the recurrence of the disease. After this, the tooth is locally fluoridated, and the process of restoring the enamel from the inside begins. This treatment method is called remineralization. Fluoridation can also be done at home - using special preparations - but only after consulting a doctor.
Also, modern methods of non-invasive treatment of enamel caries include: chemical-mechanical treatment (infiltration), air-abrasive treatment and ozone treatment. All these methods allow you to do without a drill and carry out treatment with virtually no discomfort for the patient. At the same time, it is possible to preserve healthy tooth tissue to the maximum - the microhardness of the enamel is damaged during enamel caries, and all of the above methods allow you to act only on softened tissue, without affecting the healthy parts of the tooth.
Regardless of the chosen technique, in order for the treatment of dental caries to be effective and the disease not to recur, the participation of the patient himself is important. Only a conscientious approach to hygiene will help maintain oral health.
Prevention of root caries
The following preventive measures will help reduce the risk of root caries:
- Maintaining oral hygiene. In addition to brushing your teeth, it is important to pay increased attention to careful and thorough gum care and high-quality cleaning of periodontal pockets. For this purpose, it is convenient to use irrigators, which with a powerful stream of water remove food debris even from under the gums, massage the gums, helping to strengthen them.
- Timely treatment of gum disease, as this is one of the main causes of root caries.
- A rational and balanced diet with a minimum amount of fast carbohydrates and a large amount of vitamins and minerals.
- Limited consumption of hard foods that can injure the gums.
- Regular visits to the dental clinic at least twice a year.
Following simple preventive measures will help prevent root caries and maintain dental health even in old age.
Symptoms of caries
With all the variety of types of caries, its signs are approximately the same and depend on the degree of demineralization and penetration of carious microbes deep into the dental tissues.
- Spot formation. The appearance of a patch of demineralized enamel on the surface of the tooth. Its structure is broken. At this point, the problem can be solved by simply replenishing the mineral deficiency in the area of the stain. Nothing bothers the person, and the white spot can be detected by staining with methylene blue.
- Superficial caries affects the enamel of the tooth, and middle caries affects the dentin. Typical symptoms include dark cavities in the crown, slight pain during brushing, and increased sensitivity to hot, cold, sweet and sour foods. To prevent caries from progressing to medium or deep, you need to urgently undergo treatment for superficial caries.
- Deep caries is often quite painful, and sometimes the pulp is separated from the cavity by only a thin layer of dentin. Acute pain occurs when there is a sudden change in temperature or exposure to chemical or mechanical irritants. When they are eliminated, the unpleasant sensations immediately disappear.
- If the pain continues for hours and occurs when chewing or the slightest touch to the tooth, it means that caries complications have already developed - pulpitis or periodontitis. These are very unpleasant and dangerous diseases that require serious treatment.
At the initial stage, caries can only be recognized by a dentist. This is why it is so important to visit a doctor for a preventive examination at least twice a year. Spend just half an hour on a visit, and caries treatment will consist only of tooth remineralization. Agree, maintaining a healthy smile is so easy if you spend a little more time on it!