Most patients at a dentist's appointment have long become accustomed to complex dental terms. Bridge, veneer, filling, premolar – these words are practically easy to understand when a doctor diagnoses a problem and prescribes treatment.
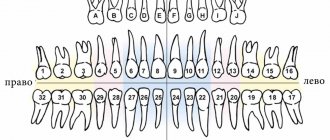
Most often, patients are confused by incomprehensible numbering . For example, when talking about wisdom teeth, the dentist can explain to the patient that the lower “eights” need treatment. Moreover, each tooth has its own numerical designation, which can reflect its type and exact location in the oral cavity.
Over the entire existence of dentistry as a science, several classifications of teeth have been invented, which are called dental formulas. Depending on the chosen numbering method, each tooth is assigned a specific number. In some systems, teeth are designated by a combination of letters, numbers and even symbols, which allows the dentition to be depicted in the form of an accurate diagram.
Classification of teeth
Among permanent human teeth, experts distinguish the following groups:
- incisors for cutting food;
- fangs, the function of which is to tear off individual food particles;
- premolars that crush food;
- molars, which serve for final grinding of food.
| Functional group | Clinical picture |
| Incisors |
|
| Fangs |
|
| Premolars | Small molars |
| Molars |
|
Such varieties indicate the development of a mixed type of nutrition in a person.
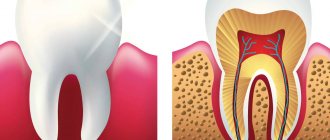
From an anatomical point of view, the tooth structure diagram includes the following parts:
- crown - the main visible part that rises above the surface of the gum;
- neck – the gingival area of the transition of the crown to the root;
- root - a fixing element located in the thickness of bone tissue and gums.
Teeth structure
Alternative names for human teeth
In addition to the official names, there are also alternative names for human teeth. They are not written in dental records, but have long been used in informal communication, since these teeth in people are located or grow in certain places or at certain times.
Eye teeth
The upper canines are called eye teeth because of their close location to the branches of the facial nerve. When they become inflamed, the pain radiates to the eye area and upper face. How close the incisive canals and the dental nerve are located to each other is shown in the figure:
Wisdom tooth
The wisdom tooth is the posterior third molar. He was called “wise” because he grows up in adulthood - when a person has already gained wisdom (by about 20 years).
Dental surfaces
The construction of a tooth profile consists of the sides discussed below.
Occlusal surface
The chewing side usually faces the teeth of the opposite side.
Occlusal parts of the dentition
Experts note that in incisors and canines this area is represented by the cutting edge.
Vestibular surface
This part of the teeth is oriented towards the vestibule of the mouth. The vestibular surface in the front part of the dentition is called the labial surface, and in the area of the large molars it is called the cervical surface.
Vestibular sides
Lingual surface
The structure of the front and molar teeth includes the lingual side directed towards the tongue. Experts call this side of the upper teeth the palatine.
Palatal surfaces of the upper incisors
The last two surfaces of the teeth described above are adjacent to the adjacent ones within the dental arch.
Contact surfaces
In the structure of the teeth of the human upper jaw, it is customary to distinguish between two types of contact sides that come into contact with adjacent teeth.
These surfaces come in two main types:
- mesial, which faces the midline of the oral cavity;
- distal – peripheral side of the tooth.
Contact surfaces
Lower molars
Three molars in a quadrant without corresponding primary teeth.
First lower molar
This is the first permanent tooth that erupts at the age of 6 years and completes its formation at approximately 9-10 years. The crown has five cusps, two lingual and three buccal (Fig. 1.49). 22-23 mm long. There are usually two roots, one mesial and one distal (97%), and we rarely find a third distolingual root (3%). In the mesial root we find two canals in 65% of cases: they may have only one apical foramen (40%) or two separate ones (60%). The distal root has one canal (70%) or two canals (30%); there may also be two separate apical foramina (38%) or only one (62%) (Figs. 1.50, 1.51 and 1.52) (Figs. 1.53 and 1.54).
Rice. 1.49. Lower first molar: occlusal view
Rice. 1.50 Anatomical pictures from Hess and Keller: lower molar with very complex canal anatomy
Rice. 1.51 Anatomical pictures from Hess and Keller: lower molar with very complex canal anatomy
Rice. 1.52 Anatomical pictures from Hess and Keller: lower molar with very complex canal anatomy
Rice. 1.53. Micro-computed tomography scan of the roots of lower molars: note the complex morphology of the pulp space
Rice. 1.54. Micro-computed tomography scan of the roots of lower molars: modern digital techniques reproduce the subtle and complex morphology of the pulp space previously illustrated by Hess histological images
All roots on the buccal side have a moderate distal slope. The pulp chamber is triangular or square, depending on the number of canals (3 or 4), located in the center of the crown in the mesial-lingual area. Because of this feature, during the formation of the pulp chamber access cavity, it is important to be careful not to remove precious tooth structure in the distal area.
The shape of the access cavity should be triangular or trapezoidal with the larger base facing the mesial ridge and the smaller (or triangular apex if there is only one distal canal) slightly distal to the central occlusal fossa (Figs. 1.55 and 1.56).
Rice. 1.55 Lower molar: access cavity to three canals
Rice. 1.56 Lower molar: trapezoidal access cavity to four canals
If there is a third root, its mouth can be found along the bottom of the pulp chamber in the corners of the base of the trapezium.
Second lower molar
The tooth erupts at the age of 11 years and is very similar to the lower first molar with some differences.
It is smaller than the first molar by 1-2 mm in each direction. It has four cusps on the occlusal surface and usually two roots, one mesial and one distal. The mesial root has only one canal in 13% of cases; most often there are two channels that end in only one opening (49%), or there are two channels with two independent openings (38%). The distal root has only one canal in 92% of cases. Rarely there are two canals with one apical foramen (5%) or two separate foramina (3%).
The access cavity to the pulp chamber is located in the middle of the mesial-lingual region and has a trapezoidal shape. Due to the size of the pulp chamber and its proximity to the mesial-lingual wall, we advise careful design of the access cavity to avoid unnecessary excision of tooth structure (see Figures 1.55 and 1.56).
Third lower molar
Erupts after 17 years, usually at the age of 25. Also called "wisdom teeth", they have an atypical and varied morphology. It can have from three to five tubercles (Fig. 1.57). Often there is a fusion of roots from two or three roots. And, as a consequence, the anatomy of the canals cannot be schematized, as with the upper molar. Experience in root canal treatment will help the clinician perform the endodontic procedure correctly (Figs. 1.58, 1.59, and 1.60).
Rice. 1.57. The varied occlusal morphology of mandibular third molars may have four to five cusps
Rice. 1.58 (a) Lower third molar with a curved mesial root fused to the distal one. (b) Lower third molar: distal root
Rice. 1.59 (a) Lower third molar with four roots, two mesial and two distal: the mesiobuccal root is a very curved canal in the middle third. (b) Lower third molar: distal view showing graceful curvature of the distolingual root
Rice. 1.60 (a) Lower third molar: on the buccal side, two separate mesial roots are visible with extremely severe curvature, according to Schneider. The distal root has a moderate 3D curvature in the mesial and lingual direction. (b) Lower third molar: from the distal side, a 3D curvature of the distal root is visible in the lingual as well as mesial direction
Igor Lukinykh
Signs of teeth
Some features of the shape of the dentition make it possible to determine whether a tooth belongs to the upper or lower jaw.
Experts determine the right- or left-sided arrangement of teeth according to the following characteristics:
- Crown angle . The chewing surface with the mesial contact side forms a sharper angle than with the distal contact side.
- Tooth root sign. The intraosseous part of each tooth is always deviated in the peripheral direction.
- Curvature of enamel . The transition of the vestibular surface to the mesial surface is always the most round compared to the opposite side.
Signs of teeth
Internal composition of teeth
These organs are a solid hollow formation.
In the section you can see:
- internal cavity, which is filled with pulp;
- hard tissues, which are represented by dentin, enamel and cement.
Pulp, dentin and enamel
Structural differences between dentin and bone tissue
A significant difference between the hard tissues of teeth and bone is the complete absence of cell bodies - osteoclasts and osteocytes, which take part in the growth and development of bone tissue. The formation of new layers of dentin occurs due to dentinoblasts located in the pulp.
And the processes of these cells pass through the thickness of dentin, the structure of which also includes collagen fibers and a special adhesive substance.
Internal structure of dentin
In the crown part, the tooth is covered on the outside with enamel, and in the root area - with cement.
Enamel
The histological structure of tooth enamel contains 97-98% mineral salts. The molecular part of this outer shell is the so-called fibrillar protein, which forms special cells for fixing minerals.
Enamel structure
The surface layers of enamel contain an increased amount of fluoride compounds, which gives it increased strength.
The main structural elements of enamel are enamel prisms, which have an S-shaped bend in the direction from the tooth surface to the pulp. Histology indicates that the thickness of these elements ranges from 3 to 7 microns.
Cement
In dentistry, cement is the name given to the coarse fibrous tissue that covers the tooth root. From a biological point of view, this structure consists of collagen fibers compacted with calcium salts.
Microscopic image of root cement
Pulp
The internal cavities of teeth in children and adults are filled with pulp in the form of loose connective tissue, nerve endings, blood vessels and dentinoblasts.
Pulp extracted from a tooth
The main function of this organ is to counteract inflammatory and infectious lesions. Thanks to the branched blood network, the pulp provides nutrition and growth of tooth dentin.
Periodontium
The complex of ligamentous apparatus, which is located in the space between the bone alveolus and the root, is called periodontium. This tissue includes collagen fibers, cells of the immune system, osteoblasts and osteoclasts.
Retaining apparatus
The main components of the periodontium are connective tissue bundles that are stretched between the alveolar wall and the root cement. Collagen fibers are tightly intertwined with each other by anastomoses, which ensures reliable fixation of the root. All teeth and their structure also have slight mobility and this is normal.
Direction of periodontal fibers
Upper premolars
Two per quadrant, premolars erupt between 10 and 12 years of age, and root formation is completed after 3 years. They replace temporary molars.
The first and second premolars have a similar crown but different morphology.
Upper first premolar
The first upper premolar erupts when the child is about 10-11 years old. It has a length of about 21-22 mm, and its buccal-palatal dimensions are 9 mm and mesial-distal dimensions are 7 mm. It has two cusps, buccal and palatine, which are slightly shorter (about 1 mm). The pulp space is determined by the shape and size of the outer crown (Fig. 1.24). In approximately 72% of cases, two roots with two different apical foramina are present (Fig. 1.25). Premolars may also have only one root with two canals (13%) (Fig. 1.26a, b), and in some cases three roots (6%) (Fig. 1.27). In addition, in 37% of cases we found a distal root bend in the apical third.
Rice. 1.24 First upper premolar: occlusal view
Rice. 1.25 Upper premolars: graphical representation of the access cavity; note the mesial position of the second premolar access cavity (right in the figure) to facilitate passage of the distally curved canal
Rice. 1.26 (a, b) Upper single-root premolar: buccal and proximal view
Rice. 1.27 Anatomical pictures from Hess and Keller: complex pulp space of an upper single-rooted premolar; two different channels have multiple messages along the root and two separate outputs
The access cavity to the pulp chamber should have an oval shape in the buccal-palatal direction, from one tubercle to another Fig. 1.28.
Rice. 1.28 Anatomical pictures from Hess and Keller: an upper premolar with three roots, two buccal and one longer palatal
Upper second premolar
The second upper premolar erupts between the ages of 10 and 12 years. It is very similar to the upper first premolar, both in size and crown shape. But there are some main differences between the roots, presented in three versions:
One root with one canal in 75% of cases (Fig. 1.29a, b)
Rice. 1.29 (a, b) Upper first premolar: mesial and distal view
One root with two canals and one or two separate apical foramina (12%) (Fig. 1.30 and 1.31)
Rice. 1.30. Anatomical pictures from Hess and Keller: an upper single-rooted premolar having two canals merging into one exit; lateral canals are also present in the apical and middle third of the canal
Rice. 1.31 Anatomical pictures from Hess and Keller: upper single-rooted premolars have two canals with separate exits, apical and lateral
Two separate roots and canals (12%)
Three separate roots (usually two of them buccal) with three canals (1%)
On the buccal side, the roots have a distal curvature in 27% of cases, and a vestibular curvature in 12% of cases, and in 20% of cases they have two sharp curvatures.
The endodontic access cavity to the pulp chamber has an oval shape in the buccal-palatal direction. If there is significant distal apical curvature, the approach should be moved closer to the mesial marginal ridge, maintaining an oval shape (Fig. 1.28).
Age-related changes in dentogingival tissues
Over time, the human dentofacial system undergoes the following changes:
- reduction in the height of the enamel layer due to abrasion of the enamel;
- the formation of microcracks, which provokes gradual staining of teeth yellow and brown;
- active formation of secondary dentin and, accordingly, a decrease in the volume of dental pulp;
- age-related thickening of the walls of blood vessels also causes a narrowing of the pulp cavity;
- an increase in the amount of cement, which is observed both with an increase in chewing load and without it;
- thickening of periodontal bundles in the area of teeth that serve as support for bridges.
Age-related microcracks and darkening of enamel
Regeneration of dental tissues
Restoration of enamel, dentin, pulp and cement is possible, but not in all clinical cases.
Regeneration of the anterior and chewing teeth, as a rule, occurs due to the following processes:
- replenishment of enamel with minerals, which is carried out both from saliva and through the blood vessels of the pulp;
- in the pulp chamber, cellular elements form a special connective tissue capsule around the inflammatory focus, thereby preventing further spread of infection;
Some features of the structure of teeth
Normally, a person’s dental structure looks like this:
- central and lateral incisors, which have one root and one root canal;
- fangs with one pronounced and massive root;
- small molars, the first of which are distinguished by a double root and two canals, and the structure of the 25th tooth is already characterized by a single root with the same number of root canals;
- large molars - the upper group has three roots and the same number of canals, and the lower group includes two roots and three canals.
Removed 25th tooth
Difference between baby teeth and permanent teeth.
PHOTO: Caries of primary front teeth. The enamel of baby teeth is thinner and less mineralized, which makes it less resistant to caries.
Unlike permanent teeth, the “lifespan” of primary teeth is much shorter. Resorption of tooth roots begins 2-3 years after their eruption in the oral cavity and continues until they fall out.
Contrary to popular belief, baby teeth, just like permanent teeth, have roots and a nerve (pulp). The roots hold the tooth in the bone. Under the milk tooth is the germ of a permanent tooth. As the permanent tooth erupts, it stimulates the resorption of the roots of the baby tooth, and by the time the baby tooth falls out, only the crown remains.
Since baby teeth (like permanent teeth) have a nerve (pulp), they can hurt if an infection from a carious cavity enters the tooth cavity, causing the development of pulpitis (inflammation of the nerve of the tooth).
392measures and structure.
- Primary teeth are smaller than permanent teeth and have less massive roots;
- Baby teeth have a more complex anatomical structure of root canals, which leads to a more labor-intensive treatment process than in permanent teeth;
- The hard tissues of primary teeth are less mineralized and less resistant to abrasion and the development of caries.
- the hard tissues of baby teeth are much thinner than those of permanent teeth: the inflammatory process quickly reaches the nerve of the tooth;
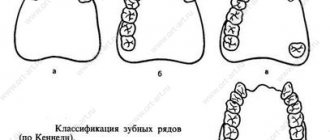
Types of closure of dentition
In dentistry, it is customary to distinguish the following three groups of occlusions:
- the central form, when the most complete contact of all rows of rows occurs;
- anterior form, with the lower jaw shifted forward;
- lateral form, which is characterized by the fact that the teeth, the structure of the human jaw, are deformed to the right or left.
Central view of teeth closure
Namely, the relationship of the dentition in the position of central occlusion is called occlusion.
The physiological norm includes the following bite options:
| Physiological occlusions | Clinical picture |
| Orthognathia |
|
| Progenia | Reverse dentition ratio |
| Biprognathia | Slight tilt |
| Straight bite | Contact of the upper and lower incisors along the cutting edges |
The choice of treatment and prevention method for dental diseases depends on the external and internal structure of the tooth and what type of occlusion is observed.
Functional properties of elements
Teeth perform several functions at once. Each element has a distinctive shape according to its purpose. The main role of the units is digestive. The quality of assimilation of useful elements by the body depends on the thoroughness of grinding the products. Only after chewing and moistening with saliva will the food be ready for subsequent processing by the digestive organs.
Chewing one piece lasts on average 10-20 minutes. The force exerted by the teeth on food sometimes reaches 80 kg. Incomplete dentition can lead to disturbances in the digestive system.
Another function of the elements is aesthetic. With malocclusion, a person may develop psychological problems, since the first thing others pay attention to during a conversation is a smile. Teeth also play a role in the formation of syllables. In the absence of one or more elements, the pronunciation of syllables changes: a lisp appears, speech is distorted.