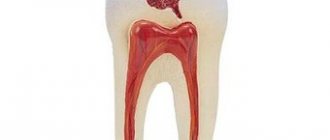
Fissure sealing is an extremely effective method of caries prevention and the main etiotropic method for the prevention of fissure caries. It involves the prevention of caries of the chewing surface of molars by filling fissures and other anatomical recesses of healthy teeth with adhesive materials - sealants in order to create a barrier to external cariogenic factors (microorganisms and carbohydrates)
Sealing tasks:
— eliminating the local risk of caries;
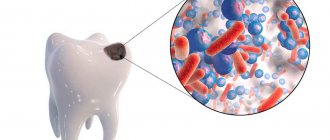
— creating conditions for the death of microorganisms remaining in the deep areas of the fissures; — elimination of potential reservoirs for the accumulation of cariogenic microorganisms; — acceleration of enamel mineralization in the fissure area when using glass ionomer cements.
Currently, glass ionomer cements, compomers, and composites are used for sealing.
Based on their chemical composition, sealants can be divided into groups:
1. Composite sealants: - classic, - sealants-ormokers, - flowable composite materials. 2. Compomers. 3. Glass ionomer cements Composite sealants can be: self-hardening and photo-hardening, for example: Estiseal LC, Fissurit, Helioseal.
Composite sealants and compomers are used to seal the fissures of teeth that have completely erupted.
Glass ionomer cements can be used for prophylactic coating of fissures in teeth at the eruption stage (Fuji VII, Fuji Triage).
Techniques for using sealants: - cleaning teeth with a regular brush, - cleaning with a circular brush with antiseptics, - applying material to fissures, - correction of teeth closure, - insulating the glass ionomer surface with varnish, - monitoring the safety of the sealant every 3-6 months.
Toothpastes for children
Requirements for children's toothpastes: Fluoride content. Daily use of fluoride toothpaste in combination with proper brushing techniques is the basis for caries prevention! The use of low fluoride toothpastes containing less than 500 ppm F in the formula as a preventive measure is considered unsatisfactory. One of the problems associated with the use of fluoride toothpaste in children is the ingestion of the toothpaste by children with the subsequent risk of dental fluorosis.
Parents are advised to monitor the amount of toothpaste and the process of brushing teeth in children under seven years of age. Low abrasiveness. For temporary teeth (baby teeth) and newly erupted permanent teeth, the use of gel pastes is optimal. The RDA value for baby toothpastes should not exceed 50.
The absence of flavoring additives that can make a child want to eat pasta. It is preferable to use neutral, mint or fruit flavors that do not cause rejection in the child.
Examples of toothpastes for children aged 2 to 3 years: - Blend-a-med (0.005% NaF-250 ppmF) - My first Colgate (NaF) - Elmex enfant (aminofluoride - 250) - Lacalut Baby (aminofluoride – 250 ppm F, vitamins A, E) – Lacalut Kids 4-8 (aminofluoride – 500 ppm F, vitamins A, E) – Oral-B Stages fruity ( NaF – 500 ppm F) – Pokemon ( Na2PO3F- 500 ppm F)
Toothpastes for children from 2 to 6 years old: - Blend-a-med Junior Gel - Colgate junior (0.15% NaF- 680 ppm F-) - Colgate junior super star (0.76% Na2PO3F - 1000 ppm million F-) - Lacalut Kids 4-8 (aminofluoride - 500 ppm F-) - Lacalut Teens 8+ (aminofluoride and NaF -1400 ppm F-) - Dental dream for children (0.5% Na2PO3F -660 ppm F-) – Four Fruit – Mildfresh junior (0.76% Na2PO3F – 1000 ppm F) – Sanino Junior – New Pearl Junior 7-12 years (0.76% Na2PO3F – 1000 ppm F, oil tea tree) – Children's pearl complex – Prodent for teenagers
What other systems exist?
Black's classification is topographical; dentistry uses several more ways to divide types of caries into features:
Universal classification ICD 10
ICD 10 is a generally accepted and unified classification of diseases that applies to all human organs, including teeth. The classification of caries according to this system is described in detail here.
Histological
Involves sorting according to histological characteristics, i.e. the conclusion is made based on what tooth tissue is affected: enamel, dentin or cement. The classification includes 3 corresponding varieties:
- Enamel caries.
- Dentin caries
- Cement caries.
According to the clinical course
Using diagnostic methods and analysis of patient complaints, the doctor determines the nature of the disease:
- Spicy.
- Chronic.
According to the depth of the lesion
The main method that helps to choose an approach to treatment. For example, medium caries lesions of the contact surface of the tooth (type 2 according to Black). There are 4 types:
- At the spot stage.
- Surface.
- Average.
- Deep.
In relation to the condition of the pulp
A conclusion is made about the involvement of the pulp in the process of tooth destruction.
- Simple.
- Complicated.
By number of teeth affected
How many teeth are affected by caries at the time of the patient’s visit to the dentist.
- Single.
- Multiple.
- Generalized.
If you find an error, please select a piece of text and press Ctrl+Enter.
Tags caries treatment
Did you like the article? stay tuned
Previous article
Pathological causes of burning tongue and proper treatment
Next article
Gentle and effective treatment of periodontitis with a smart device Vector
The structure of the pterygopalatine fossa
Author: Chen C
The pterygopalatine (pterygopalatine) fossa can be defined as the “control center” of the maxilla, as it provides vasculature through the maxillary artery, as well as somatosensory and autonomic innervation through the maxillary nerve and the pterygopalatine ganglion of the midface. Located along the visual line separating the facial and cerebral regions of the skull, the pterygopalatine fossa represents a natural intersection between the anatomical regions related to the skull base, facial, intracranial, oral and cervical regions (Roberti et al., 2007). The pterygopalatine fossa is located between the palatine bone, that is, the most posterior part of the upper jaw, and the pterygoid plate of the sphenoid bone (Figures 1 and 2). Its shape is an elongated and inverted tetrahedral pyramid with the apex pointing downwards. Originally, the term “pterygopalatine fossa” was used only for the most superior and medially limited part that contained the pterygopalatine ganglion; however, the definition has expanded to include the complete bony compartment, which contains several important neurovascular structures (Daniels et al., 1998).
The pterygopalatine fossa communicates with several anatomical regions (Table 1), including the middle cranial fossa through the foramen rotundum and the pterygoid canal, the orbit through the inferior orbital fissure, the nasal cavity through the sphenopalatine foramen, the oral cavity through the pterygoid canal and the infratemporal fossa. through the pterygomaxillary fissure (Erdogan et al. 2003; Hwang et al. 2011a). The arterial component of the pterygopalatine fossa is located anteriorly, and the nervous system component is located posteriorly (Morton and Khan 1991).
Brief description of the openings and their contents in the pterygopalatine fossa (Table 1)
| Hole | Location relative to the pterygopalatine fossa | Connection with the pterygopalatine fossa | Vascular contents | Neural content |
| Round hole | Posterosuperior | Middle cranial fossa | Venous plexus | Maxillary nerve |
| Pterygoid canal (Vidian canal) | Rear | Middle cranial fossa | Pterygoid artery and vein | Pterygoid nerve |
| Inferior orbital fissure | Anterosuperior | Eye socket | Infraorbital artery and vein | Infraorbital nerve; orbital and zygomatic branches from the maxillary nerve |
| Sphenopalatine foramen | Medial | Nasal cavity | Sphenopalatine artery and vein | Nasal branches of the maxillary nerve |
| Palatovaginal (pharyngeal) canal | Superomedial | Nasopharynx | Pharyngeal branch of the maxillary artery | Pharyngeal branch of the maxillary nerve |
| Vomerovaginal canal | Superomedial | Nasopharynx | Small arteries | Small nerves |
| Pterygopalatine canal | Lower | Sky | Descending palatine artery and vein (greater and lesser palatine artery and vein) | Greater and lesser palatine nerves |
| Pterygomaxillary fissure | Lateral | Infratemporal fossa | Maxillary artery (enters the pterygopalatine fossa) | Posterior superior alveolar artery (emerges from the pterygopalatine fossa) and vein |
Figure 1 Side and left view of the skull showing the location of the pterygopalatine fossa (inverted pyramid)
What are blind fossae?
The upper jaw, maxilla, is a paired bone with a complex structure due to its diverse functions: participation in the formation of cavities for the sensory organs - the eye socket and nose, in the formation of the septum between the cavities of the nose and mouth, as well as participation in the functioning of the masticatory apparatus.
The transfer of the grasping function from the jaws (as in animals) to the hands in humans due to their work activity has led to a decrease in the size of the upper jaw; At the same time, the appearance of speech in humans made the structure of the jaw more delicate. All this determines the structure of the upper jaw, which develops on the basis of connective tissue.
The upper jaw consists of a body and four processes.
A. The body, corpus maxillae, contains a large air sinus, sinus maxillaris
(maxillary or maxillary, hence the name for sinus inflammation - sinusitis), which
with a wide opening, hiatus maxillaris
, opens into the nasal cavity. There are four surfaces on the body.
Front surface, facies anterior,
in modern humans, due to the weakening of the chewing function caused by artificial cooking, it is concave, while in Neanderthals it was flat.
Below it passes into the alveolar process, where a number of elevations are noticeable, juga alveolaria
, which correspond to the position of the dental roots.
The elevation corresponding to the canine is more pronounced than others. Above it and laterally there is a canine fossa, fossa canina
.
At the top, the anterior surface of the upper jaw is delimited from the orbital by the infraorbital margin, margo infraorbitalis
.
Immediately below it is noticeable the infraorbital foramen, foramen infraorbital
, through which the nerve and artery of the same name emerge from the orbit.
The medial border of the anterior surface is the nasal notch, incisura nasalis
.
Infratemporal surface, facies infratempordlis,
separated from the anterior surface by the zygomatic process and bears
the tubercle of the upper jaw, tuber maxillae
, and
sulcus palatinus major
.
Nasal surface, facies nasalis
, below passes into the upper surface of the palatine process.
A ridge for the inferior nasal concha (crista conchalis)
.
Behind the frontal process there is a noticeable lacrimal groove, sulcus lacrimalis
, which, with the lacrimal ossicle and inferior concha, turns into
the nasolacrimal canal - canalis nasolacrimalis
, connecting the orbit with the lower nasal meatus.
Even more posteriorly there is a large opening leading to the sinus maxillaris
.
Smooth, flat orbital surface, facies orbitalis,
has a triangular shape.
On its medial edge, behind the frontal process, there is a lacrimal notch, incisura lacrimalis
, into which the lacrimal ossicle enters.
Near the posterior edge of the orbital surface, the infraorbital groove begins, sulcus infraorbitalis
, which anteriorly turns into
canalis infraorbitalis
, which opens with the above-mentioned
foramen infraorbitale
on the anterior surface of the upper jaw.
Alveolar canals , canales alveoldres
, for nerves and vessels, extending from the infraorbital canal to the front teeth.
B. Processes. 1. Frontal process, processus frontalis,
rises upward and connects with the pars nasalis of the frontal bone.
On the medial surface there is a ridge, crista ethmoidalis
- a trace of the attachment of the middle turbinate.
2. Alveolar process, processus alveolaris,
on its
lower edge, arcus alveolaris
, has
dental cells, alveoli dentales
, of the eight upper teeth;
the cells are separated by septa, septa interalveolaria
.
3. Palatine process, processus palatinus
forms most of
the hard palate, palatum osseum
, connecting with the paired process of the opposite side by a median suture.
Along the median suture on the upper side of the process facing the nasal cavity there is a nasal ridge, crista nasalis
, connecting to the lower edge of the vomer.
Near the anterior end of the crista nasalis
on the upper surface there is a noticeable hole leading into
the incisive canal, canalis incisivus
.
The upper surface is smooth, while the lower one, facing the oral cavity, is rough (impressions of the glands of the mucous membrane) and bears longitudinal grooves, sulci palatini
, for nerves and blood vessels.
In the anterior section, an incisive suture (sutura incisiva)
.
It separates the incisive bone, os incisivum,
, which in many animals occurs in the form of a separate bone (os intermaxillare), and in humans only as a rare variant.
4. Zygomatic process, processus zygomaticus,
connects to the zygomatic bone and forms a thick support through which pressure is transmitted to the zygomatic bone during chewing.