The dentofacial system is an important component of the human masticatory apparatus. It meets morphological and functional characteristics, such as number, size, shape, color, structure of dental units. There are a number of genetically determined or external factors that lead to disruption of these characteristics. Dental anomalies can have various consequences: some lead to periodontal pathologies, various forms of caries, others seriously limit chewing function, cause injury to the mucous membrane, and others cause aesthetic problems.
Improper growth of teeth results in speech and bite defects and breathing problems. As a result, the patient’s general health seriously suffers, and psychological problems arise.
Reasons causing anomalies
Anomalies of the dental system are very diverse and include both anomalies of dental units and incorrect formation of the dentition, as well as abnormalities in the development of the jaws. The most frequently diagnosed abnormalities of dental units. They can be caused by a wide variety of reasons, including both exogenous (caused by external factors) and endogenous (formed as a result of the physiological state of the patient).
Endogenous causes
Endogenous anomalies are formed as a result of genetic and endocrine disorders.
- Many structural features of the dental system, leading to improper development of teeth, are genetically determined. This can occur through direct inheritance (abnormal number and shape of teeth, edentia, diastema), through inheritance of a mismatch in the size of the jaw bones, through inheritance of a mismatch in the size of the jaw and teeth (crowding of teeth or sparse arrangement of teeth). Dental anomalies of this type include disorders associated with hereditary and congenital pathologies (clefts of the soft and hard palate, cleft lip, Down syndrome, Vaanderburg syndrome, Seckel syndrome, Shershevsky-Turner syndrome).
- Another part of the endogenous causes of dental anomalies are problems of the endocrine system, such as hypothyroidism (in later stages), hyperparathyroidism, hypocortisolism. Their frequent symptoms may be delays in the eruption and replacement of teeth, and disturbances in the formation of the enamel layer.
Exogenous causes
Exogenous (external) causes of dental anomalies are, for the most part, external unfavorable factors that affect the baby’s body during the formation of tooth germs. There are prenatal (prenatal), postnatal (postpartum) and intranatal (associated with childbirth) periods.
- An example of a prenatal factor is a pregnant woman living in poor environmental conditions. Various developmental disorders of the fetus can also occur as a result of the mother’s poor lifestyle.
- Factors in the intranatal period may include complicated labor, birth injuries, consequences of asphyxia and oligohydramnios.
- In the postnatal period, dental anomalies develop as a complication of pathologies in early childhood. These include childhood infections, rickets, hypovitaminosis, and micronutrient deficiency.
All these reasons are of a common nature. Local factors that affect dental development include everything related to improper oral care, feeding errors or bad habits. Among them are feeding too soft food, prolonged sucking of a pacifier or finger in early childhood.
Childhood injuries and caries with complications lead to dental anomalies.
The death of tooth germs or the development of supernumerary teeth can occur due to osteomyelitis.
Causes and diagnosis
Negative factors that can lead to the development of tortoanomaly include:
- Genetic predisposition;
- Incorrect development of the jaw arch;
- Mechanical damage that caused tooth rotation;
- Tumor formation in bone tissue;
- Crowding of units or uneven eruption;
- Micrognathia and macrodentia;
- Premature change of bite;
- Atypical position of the tooth germ.
To make an accurate diagnosis, as a rule, a visual examination is sufficient, but in some cases the use of auxiliary techniques is allowed. This list includes:
- X-ray survey of the problem area, determining the position of the root segment relative to neighboring units;
- Orthopantogram, which reveals the condition of bone tissue;
- Analysis of anthropometric data, establishing the degree of rotation in accordance with the tables developed by Wetzel and Ustimenko.
Detection and correction of pathology at an early age allows you to avoid radical correction methods, restore the aesthetics and functionality of the dentition, and prevent the further development of anomalies that negatively affect the condition of the jaw.
Anomalies in the number of teeth
All anomalies in the number of teeth are divided into three types:
- hyperodontia (excess of dental units above normal);
- edentia (complete absence of teeth);
- hypodontia (insufficient number of teeth).
Hyperodontia
Hyperodontia is a disorder of the formation of the dentition, which is expressed in the presence of supernumerary teeth (over 32 dental units in an adult). The cause of the disease may be a violation of the mechanism of formation of tooth germs in childhood or infancy. Hyperodontia mainly affects the incisors of the upper jaw. Other teeth are involved in the pathological process less frequently. Extra dental units grow small and have a cone shape.
The disease can be true or false.
- With true hyperodontia, the formation of extra dental units occurs in the human jaw.
- False hyperodontia occurs when the loss of primary teeth is delayed, which interferes with the normal growth of permanent teeth.
With polyodontia, teeth may erupt away from the dentition or next to a correctly positioned dental unit, which leads to its gradual displacement. The dentition can be seriously deformed, which leads to serious diction problems.
If supernumerary teeth interfere with the development of normal teeth, they must be removed. Broken teeth are corrected by installing braces.
In those rare cases when a row violation does not occur, the supernumerary tooth is preserved. Prosthetics are used to correct the shape.
Hypodentia
Hypodentia is a deficiency of dental units. This disorder occurs most often due to the death of tooth germs in the fetus. A small number of teeth causes a shift in the midline, the formation of wide gaps between teeth (diastema and three), and shortening of the dentition. All this adversely affects the bite. Possible ways of correction are prosthetics.
Edentia
Adentia is a complete or partial absence of teeth. With edentia, the continuity of the dentition is disrupted, which leads to difficulties in chewing and speaking. The reason is a violation of the development or death of tooth germs under the influence of genetic factors or under the influence of unfavorable external factors during the formation of the dental plate in the fetus (the formation of the germs of permanent teeth in the fetus occurs after the 17th week of intrauterine development). The disorder is corrected using prosthetics or dental implantation.
Anomalies of dental development
The dentofacial system is an important component of the human masticatory apparatus. It meets morphological and functional characteristics, such as number, size, shape, color, structure of dental units. There are a number of genetically determined or external factors that lead to disruption of these characteristics. Dental anomalies can have various consequences: some lead to periodontal pathologies, various forms of caries, others seriously limit chewing function, cause injury to the mucous membrane, and others cause aesthetic problems.
Improper growth of teeth results in speech and bite defects and breathing problems. As a result, the patient’s general health seriously suffers, and psychological problems arise.
What to do in such a situation? To get started, we recommend reading this article. This article describes in detail methods of controlling parasites. We also recommend that you consult a specialist. Read the article >>>
Supernumerary teeth (hyperdentia) are found in both primary and permanent teeth, more often in males. In a primary dentition, the teeth are positioned normally. The supernumerary milk tooth erupts primarily in the area of the anterior teeth of the upper jaw.
In the permanent dentition, supernumerary teeth are usually smaller in size than normal teeth and have an irregular shape. Most often they are localized in the area where the central anterior teeth and molars of the upper jaw are located. The supernumerary tooth has an awl-shaped shape with a conical crown and a shortened root. It is typically located between the maxillary central anterior incisors, but can also be impacted and displaced. It is likely that the reason for this phenomenon is the presence of an additional tooth germ with autosomal dominant heredity.
If the supernumerary tooth is located between the central and lateral incisor of the upper jaw, it is called an awl-shaped tooth.
Distomolars are formed from the distally elongated dental lamina of the third molars (sometimes the fourth and fifth molars). These are small teeth similar in shape to molars.
When supernumerary teeth are located on the buccal surface between normal molars, they are called “paramolars.”
Additional canines (mostly in the upper jaw) or premolars (mostly in the lower jaw) are often impacted and can only be detected radiographically.
In patients with congenital nonunion of the maxilla and palate and dysostosis cleidocranialis, hyperdentia occurs more often than in other patients. Sometimes, at the birth of a child or after some time, the central incisors of the lower jaw (natal, neonatal teeth) may erupt. These teeth are not always supernumerary; they are often normal teeth that have erupted prematurely. Often the mineralization processes in them are disrupted, the teeth have significant mobility (there is a possibility of their falling out with subsequent aspiration).
Congenital absence of teeth is defined as edentia (absence of all teeth), oligodontia (partial edentia) and hypodontia (absence of single teeth). These anomalies are often combined with autosomal dominant inherited ectodermal dysplasia, Down syndrome, congenital nonunion of the maxilla and palate, otofacial dysostosis, etc.
The presence of very large or very small teeth is called macrodentia or microdentia, respectively (lateral incisors of the upper jaw, third molars).
Rhizomegaly is the presence of roots whose length exceeds normal (canines of the upper jaw), rhizomycria is the formation of roots of shorter length (central incisors of the upper jaw, third molars, premolars).
Taurodentism is a rare dental anomaly in which the pulp chamber of molars and premolars reaches the root area. The root is wide, dense in structure, without branches. The structure of the hard tissues of such a tooth is usually normal.
A condition in which overly wide teeth are found with a groove or notch in the middle (the crown of the tooth is sometimes twice the size of a normal one) is called gemination. The pulp chamber is usually one, but it can branch in the coronal direction. The formation of such a tooth is caused by disturbances in the development process, leading to the fusion of tooth buds. If a tooth germ is separated, an additional twin tooth appears (schizodentia).
Sometimes there is a complete or partial fusion of two adjacent tooth germs in the area of the root and crown. The roots of adjacent teeth can also connect.
It is difficult to differentiate tooth fusion at the site of cement location from the above case. A special anomaly in the development of an individual tooth is invagination, i.e., depression of the surface of the tooth during its development.
The impact of any pathological factors on the developing dental system is often the cause of various anomalies of this system. The data available in the literature indicate that anomalies in the pathology of the maxillofacial system are quite common. There are cases of a combination of several types of anomalies, since often the development of one type of anomaly entails the occurrence of another. For example, a change in the number and size of teeth is usually combined with their incorrect location in the dental arch.
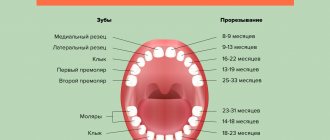
In the clinic, the most common anomalies associated with changes in the timing of teeth eruption, their number, size, shape, color, and position in the alveolar process. Teeth develop and erupt at certain times, and by the time of their eruption one can judge the physical development of the child. A delay in the eruption of all or individual groups of teeth is observed in children suffering from rickets, tuberculosis, suffering from dysfunctions of the nervous or endocrine system, as well as from chronic starvation, etc. Disturbance in the eruption of individual teeth is more often associated with some local reasons, for example, incorrect the location of the rudiments, as a result of which the teeth cannot erupt. Retention of teeth occurs, that is, they are retained in the jaw. The canines of the upper jaw, the third molars of the lower jaw, and less often the premolars are more often affected by retention. Tooth retention can be the result of abnormal development of the jaws, inflammatory processes in them, which causes fusion of the roots of the teeth with the bone tissue of the alveoli. Fusion of the roots of adjacent teeth can also cause impaction of these teeth.
Often, retention of the canines of the permanent dentition or premolars, as well as their eruption outside the arch, is associated with the early removal of the canine or second molar of the primary dentition. Retention in these cases occurs as a result of overgrowth of the alveolus with bone tissue or movement of the first premolar or first molar of the permanent dentition towards the extracted tooth, i.e., to the place where the canine or second premolar should erupt. Often impacted teeth are located in such a way that only part of their crown erupts (semi-retention). In these cases, conditions are created for the occurrence of an inflammatory process around the crowns of semi-impacted teeth, and pericoronitis occurs, which is especially often observed in the area of the third molars of the lower jaw.
In some cases, orthodontic methods can stimulate the process of eruption of an impacted tooth and install it in the dentition. Impacted teeth that cause inflammation or any other undesirable changes in the jaw system are usually treated surgically. Cases of eruption of impacted teeth in old age after tooth loss or atrophy of the alveolar process have been described.
Cases of early teething are quite rare. These include intrauterine eruption of the temporary central incisors of the lower and, somewhat less frequently, the upper jaws. It is assumed that the reasons causing the premature eruption of “congenital” teeth are the formation of a tooth germ ahead of time, its accelerated development, possibly even outside the bone tissue, the superficial location of the tooth germ, the inflammatory process of the periosteum of the jaw or gums, etc. The crowns of such teeth significantly fewer milk teeth of the same name, erupted on time, yellowish in color, less often white. Many teeth have areas of enamel necrosis.
In order to normalize the child’s nutrition, “congenital” teeth are in most cases removed. Since the tooth root develops later, this operation does not cause difficulties or complications. Often, after removing the crown of a tooth, a small red tubercle remains on the gum, which is a pulp with a growth zone, which soon disappears. Later, a tooth root may develop in the area of the removed crown, the length and width of which is less than the normal roots of primary teeth. The germ of the permanent tooth of the same name develops normally, but more often at an earlier date compared to teeth of the same group. It is considered normal when a person has 20 teeth in the primary dentition and 32 in the permanent dentition. A change in the number of teeth can occur in both the primary and permanent dentition, but the primary dentition is more stable in this regard.
A decrease in the number of teeth is called partial edentia, and the absence of all teeth is called complete edentia. Adentia is considered primary if teeth are missing as a result of the death of the rudiments of individual or all teeth. Secondary adentia occurs as a result of tooth extraction due to their disease. There are many reasons behind primary adentia. The most common of them is a violation of metabolic processes in the child’s body and the associated disorder in the processes of mineralization of the teeth germ with their subsequent death. At the same time, other groups of teeth with later stages of formation usually have malformations of enamel and dentin (hypoplasia). The death of a tooth germ may be associated with local causes - an inflammatory process in the area of the root apex, temporary (baby) tooth, or in the alveolar process. Partial or complete aplasia can occur as a result of a hereditary disease - ectodermal dysplasia. Depending on the timing of the development of this disease, aplasia of temporary and permanent teeth or only permanent teeth may occur.
It should be noted that most authors do not classify the absence of third molars as an anomaly due to the fact that these teeth are considered reducing. There are people who lack the lateral incisors of the upper jaw. Some authors also classify them as endangered, while others see a connection between this anomaly and congenital syphilis.
Along with cases of partial or complete aplasia of teeth, the formation of a larger number of teeth compared to normal is observed. Supernumerary teeth are more common in the permanent dentition. They may have a normal shape, characteristic of any group of teeth, or it may be changed. The spiky shape of supernumerary teeth is common. They are rarely located in the dentition, often erupt outside the dental arch or displace normal teeth beyond its limits, taking their place. Sometimes several supernumerary teeth erupt, forming a second row. More often, such eruption is observed in the area of the frontal teeth of the upper jaw. In some cases, supernumerary teeth erupt in the dentition, pushing apart normal teeth. For example, a supernumerary awl-shaped tooth sometimes erupts between the central incisors of the upper jaw.
Depending on their shape and position, supernumerary teeth are removed if they interfere with chewing function, injure the mucous membrane, or do not externally meet aesthetic standards. In some cases, if the supernumerary tooth has the shape of a normal tooth, and moving it into the dentition is less difficult than the normal one, then the last tooth is removed and the supernumerary is moved into the dentition.
To date, there is no sufficiently satisfactory explanation for the reason for the formation of supernumerary teeth. Some authors regard this phenomenon as atavism, others as increased productivity of the dental plate. Incorrect development of jaws and teeth, caused by any general diseases, heredity or local factors, is the cause of violation of the timing of eruption and incorrect placement of individual teeth or groups of them in the dentition. Underdevelopment of the jaws can lead to crowded teeth, with some teeth erupting in the buccal or lingual position and the front teeth overlapping each other in a tiled manner. A similar anomaly occurs when inheriting a small jaw of one parent and wide teeth of the other. Inverse relationships, i.e., inheritance of a large jaw and small teeth, lead to the formation of gaps between the teeth - three. They can also occur in cases of dysfunction of the pituitary gland and in cases of acromegaly formation. Gaps between only two teeth, usually the central incisors of the upper and lower jaws, are called diastema. The formation of diastemas is associated with hereditary factors or low attachment of the labial frenulum.
Tooth eruption with a displacement towards the cheek is often observed in third molars. In these cases, such teeth can cause the formation of pressure ulcers.
Bad habits in children can contribute to improper teething: sucking fingers, tongue, upper or, more often, lower lip, cheek. Finally, as noted, the eruption of teeth outside the arch may be the result of early removal of primary teeth.
Anomalies in the location of the teeth include the so-called tortoanomalies - cases when the lateral surfaces of the tooth are turned towards the tongue and vestibule of the mouth, or the tooth is rotated 180°, i.e. its oral surface is turned towards the vestibule of the mouth or, conversely, the vestibular surface is turned to the side the oral cavity itself.
There are cases of teeth cutting out of place - such teeth are called wandering.
Different people's teeth are not the same size. These deviations are not clearly expressed, and some authors provide average figures characterizing the size of normal teeth in each group. However, there have been cases in which the teeth differ sharply in size from normal ones: they are either very large or, conversely, small. This anomaly is associated with disruption of the activity of the endocrine glands during the period of tooth development.
The close proximity of tooth rudiments in the dental plate can lead to the fusion of these rudiments, resulting in the eruption of fused teeth (dens confusi). The fusion of the central incisors with the lateral incisors is most often observed. Such teeth are very wide; in the center of them, at the junction, a shallow hollow is noticeable on the vestibular and lingual surfaces. There have been cases of fusion of normal and supernumerary teeth. In addition, incomplete fusion of only the roots of the teeth is possible, while their crowns appear normal; There may also be inverse relationships. Incomplete fusion is more common in second and third molars.
The most common anomaly is an anomaly in the shape of the teeth. Normal teeth have a certain shape, characteristic of each group. However, during the period of tooth formation, a number of general and local pathological agents can cause deviations in the development of teeth and lead to changes in their shape. The most common underdevelopment of tooth crowns is hypoplasia. Teeth with hypoplasia can have different shapes. They are often named after the authors who first described them, for example, the teeth of Hutchinson, Fournier, Pfluger, Turner (see Non-carious lesions of teeth).
Changes in the roots of teeth are common; Among them, curvatures, changes in shape, size, and often in the number of roots are especially frequent. An increase in the number of roots is especially common in third molars; an additional, second, root is sometimes found in the second premolar, as well as the canine. In third molars, the roots may merge into one; in other cases, the size of the roots is increased and they are widely spaced from each other,
Changing the color of teeth is due to many reasons, both intrinsic and exogenous, as well as hereditary factors. Endogenous changes in the color of dental tissue can be seen in endemic fluorosis, when depigmentation of the enamel occurs, followed by exogenous impregnation of the surface layers of the enamel with a pigmenting substance from light yellow to dark brown. Discoloration is also observed with dental hypoplasia. Particularly characteristic is the yellow-gray color of teeth, which occurs as a result of taking tetracycline during their formation. Cases of teeth staining pink in patients with cholera, typhoid, and rheumatism have been described. In cases of these same diseases, as well as in cases of dysentery, porphyrinuria, and carbonic acid poisoning, some patients experienced red staining of teeth. In addition to fluorosis, yellow and brown colors have been observed in diseases of hematogenous jaundice, addneon disease, and chronic lead poisoning. Green color of teeth occurs due to chronic poisoning with mercuric chloride and copper salts. Long-term use of medications or water containing iron can lead to bluish discoloration of teeth.
The described cases of tooth staining are rare in the clinic, and some of them are considered incidental. Exogenous staining of teeth, which occurs for many reasons, is much more common. Among them, the most common are pigmentation of tooth tissues as a result of caries, from filling material (amalgam), some medicinal drugs (silver, resorcinol formalin liquid), etc. In addition, various staining of tooth crowns is observed in hereditary diseases: amelogenesis imperfecta, dentinogenesis, osteogenesis, Capdepon's dioplasia. The teeth may have a light yellow, amber, brown, or light purple color (see Dental diseases of non-carious origin).
Anomalies of magnitude
There are two forms of this type of deviation, including macrodentia (increase in the size of dental units) and microdentia (small teeth).
Macrodentia
With macrodentia, the size of dental crowns is significantly increased. The cause of the disorder is, in most cases, dysfunction of the endocrine system, which is characterized by the fusion of several rudiments together. The disease is localized mainly in the area of the upper incisors. Large teeth interfere with the process of eruption and growth of neighboring dental units, which leads to their abnormal arrangement and crowding. Giant teeth are found on or outside the dentition line. This is a serious cosmetic defect that causes serious functional impairment and psychological disorders. Pathologically enlarged teeth are removed, and the growth of adjacent teeth is corrected using prosthetics or braces.
Microdentia
Microdentia – teeth that are too small. The disorder mainly affects the upper lateral incisors, but may affect the incisors of the lower or both jaws. The cause of the anomaly has not been studied, but it is reliably known that it develops in genetically predisposed patients. With the problem of small teeth, patients develop too large interdental spaces, which significantly disrupts the aesthetics of the dentition. To correct the pathology, incorrectly growing teeth are removed or covered with crowns.
Conservative treatment
The anomaly can also be corrected using conservative methods. Often, a braces system is successfully used for this. At the first stage of pathology development, a nickel-titanium arc with a minimal cross-section is used. Then a thicker analogue is installed instead. At the last stages, an elastic rectangular chain is already used. Braces give good results, but wearing them is usually accompanied by discomfort.
Composite materials can be used to correct one tooth:
Elastic positioners are used only in cases of slight deviation. They can be described as double-jawed mouth guards with tooth channels and labial arches. Stabilization of muscle function is an additional function. The plates should be put on before bed and worn during the day for two hours.
If the pathology is caused by an overly narrow jaw, a Coffin loop can help correct the defect. The corrective part of the semicircular device has two arches (for the internal and external dentition), pressing on the curved units and forcing them to turn in the required direction. The ends are located on the alveolar ridge. The purpose of the device is to expand the jaw.
Monoblock with Coffin loop
Angle's device. The main element of the device is a spring arch that tightens the teeth. It can be stationary, sliding or expansive. The choice of a specific system depends on the type of anomaly. Using this device, you can return one tooth or several to its normal position.
Engle's apparatus
Shape anomalies
There are pathologies in the development of dental units, due to which they acquire an unnatural shape. These disorders are named after the scientists who first described them. The following types of dental shape anomalies are found: spiny teeth, Pflueger teeth, Fournier teeth, Hutchinson teeth.
- Spiked or awl-shaped teeth. With this pathology, the teeth acquire a cone-shaped shape. Wide at the base, they gradually narrow and, towards the cutting edge, become sharpened into a spike shape. This problem is combined with microdentia. There are irregularities and stains on the surface of the teeth. The disease affects the front and lateral incisors. The disease occurs in childhood and is caused by genetic factors in combination with external factors. Among them are vitamin D deficiency and endocrine system problems.
- Hutchinson's teeth are characterized by a modified crown shape of the incisors. Externally, they have the shape of a barrel, since the neck is significantly thickened. The cutting edge of the teeth acquires an arched notch. The enamel layer also suffers, which is present only on the sides and absent in the center.
- Fournier's teeth are a form of systemic hypoplasia of dental units associated with metabolic disorders at the stage of intrauterine development of the fetus. The barrel-shaped shape of the teeth is preserved, but the notch of the incisal edge is absent. The color of the enamel is not disturbed, but the enamel layer is underdeveloped, which can be seen during microscopic examination.
- Pflueger's teeth are a disorder that affects permanent dental units. Their crowns take on a conical shape. Thickening develops in the cervical region, and the chewing surface is significantly underdeveloped. The chewing function of the teeth is completely preserved.
- Turner anomaly. With this pathology, there is no enamel on the teeth. They have an abnormally lumpy surface, and replacement tissue, dentin, forms in the exposed areas.
Systemic hypoplasia with a violation of the shape of the teeth has three degrees of development. The third degree is the most dangerous, in which the crown is severely deformed and the enamel layer decreases. In this case, the defective teeth are removed and replaced with dentures. It is also possible to restore affected teeth using reflective components.
Etiology of the pathological phenomenon
Tortoanomaly is a polyetiological problem. Various factors, both acquired and congenital and/or genetically determined, can lead to its development.
The most common reasons include the following:
- Lack of space in a row due to narrowing of the jaw and/or macrodentia.
- Pressure on the causal unit from neighboring supernumerary or displaced units.
- Incorrect follicle formation.
- Too early replacement of “milk jugs” with permanent units or, on the contrary, their persistence (delay in eruption).
- Injuries in the area of the anterior teeth.
- Genetic predisposition.
- Malignant and benign neoplasms that put pressure on the problematic tooth.
Other factors cannot be excluded as the cause of tortoanomalies. In particular, bad habits, disorders in the prenatal period, improper treatment of other anomalies, etc.
What is coronoradicular teeth separation, in what cases is it performed, what does it give.
Come here if you are interested in the dangers of a split tooth.
At this address https://orto-info.ru/zubocheliustnye-anomalii/zubov/razmera/nazyivayut-korotkimi.html we will tell you how short teeth are corrected.
Anomalies of hard tissue structure
An altered shape, abnormal size or color of enamel is formed against the background of an abnormality in the structure of the hard tissues of the dental unit. Among such anomalies are:
- Hypoplasia (underdevelopment of tissue). The initial degree of the disorder is manifested by the presence of chalky spots on the enamel and areas where tissue deficiency is observed. Subsequently, all kinds of pits, grooves, and recesses appear on the surface of the enamel. The defect affects all teeth in the dentition.
- Hyperplasia (excessive tissue formation). Pathology also affects all teeth at the same time. It is characterized by areas where tissue growth is observed - tubercles, sagging enamel. The consequence of the pathology is a change in the shape and size of the teeth, a violation of the occlusion (the line of contact of the upper and lower jaws).
- Anomalies of amelogenesis (enamel formation) are expressed in the presence of brown or yellow spots on the surface of the teeth. Areas where the natural composition of the enamel is disrupted become especially sensitive. Microdentia develops against the background of pathology. The cause of the development of pathology is a deficiency of microelements that take part in the formation of dental tissue. Treatment consists of replenishing this deficiency. Additionally, local remineralizing therapy and physiotherapy are performed.
- Disturbance of dentinogenesis consists of dysfunction of the mechanism of dentin formation. The main symptoms of the disease are as follows: teeth become yellow-brown or grayish in color. The fragile dentin in these areas quickly wears off, causing tooth decay and then tooth loss. The disease occurs in genetically predisposed patients. The problem can only be solved by replacing the units destroyed by the disease with prosthetics.
Treatment methods
Treatment methods for tortoanomaly are determined by the severity and nature of the pathology, and are divided into the following categories:
- conservative;
- surgical;
- combined.
In general, depending on the amount of rotation of the tooth, the entire range of means and techniques designed to correct any dental anomalies can be used.
Conservative
Used for moderate and minor deviations from the norm (up to 40°). The general principle of conservative treatment is to create, using various orthodontic devices, a pair of forces that rotate the tooth around its axis into a physiologically correct position.
These orthodontic devices include the following:
- Trainers and elastopositioners are devices in the form of two-jaw mouthguards with lingual and vestibular arches that act on torto-abnormal teeth to return them to the correct position.
These devices are used for minor deviations, are put on at night and worn during the day for about 2 hours, mainly during the changing dentition. Simultaneously with the position of the teeth, they normalize (relieve hypertonicity) and the work of the masticatory muscles. - Braces are well-known non-removable systems, effective if the severity does not exceed 40°.
Used after replacing baby teeth with permanent ones. The difficulty of using braces to correct tortoanomalies is that the rotated crown prevents the clasp from fitting tightly to it. Therefore, the latter moves mesially or distally, and its position may change during the treatment process. - Various fixed hardware with springs, screws and arches.
It is often used to correct thoracic anomalies caused by lack of space due to narrowing of the jaws. Screws and springs expand the jaw, and lingual and vestibular arches act on the rotated tooth, returning it to its physiological position.
Aligners can also be used to correct tortoanomalies .
How to straighten teeth with braces, watch the video:
Surgical
Surgical control methods are used mainly in adults for disorders of any degree, and are divided into the following types:
- Removal of the causative tooth . Used as a last resort if other methods are not feasible or do not guarantee success.
- Compactosteotomy .
It is used as a stage of complex treatment - surgery + orthodontic methods. It is divided into lattice - drilling holes in the bone of the alveolar ridge in the root area in a checkerboard pattern - and tape - removing strips of bone up to 3 mm wide. Compactosteotomy makes the bones of the alveolar ridge more plastic and susceptible to restructuring. - Fibrotomy is the dissection of periodontal fibers with a thin scalpel, and rotation of the tooth into the desired position, followed by fusion of the fibers in the new position.
- Incomplete dislocation – rupture of the ligaments under local anesthesia by turning the tooth using forceps. The method is also called forced redressal.
It is mainly used for the anterior teeth of the upper jaw. The method is simple to perform if the surgeon has certain skills, but has limitations that make it rarely used.The width of the tooth being rotated must be less than the distance between adjacent teeth, and its single root must be absolutely straight (determined by x-ray). Rubber pads are placed on the cheeks of the tongs to protect the enamel from chipping. The turn itself is very slow.
Surgical methods are considered the most effective, but at the same time traumatic. Therefore, they are resorted to only when it is impossible to use conservative methods.
Is it necessary to correct the oral position of teeth and what do experts suggest?
In this publication we will talk about the reasons for the physiological absence of lateral incisors and ways to solve the problem.
Here https://orto-info.ru/zubocheliustnye-anomalii/zubov/formyi/slivshiesya.html we’ll talk about fused teeth: is it possible to fix this without surgery.
Color anomalies
Healthy, young teeth look snow-white due to a thick dentin layer and high-quality enamel, which has sufficient characteristics of whiteness, shine and transparency. Lifestyle, age, genetic factors, and ecology can slightly change the color of teeth from bluish to yellow. Small deviations are not considered pathology, although they indicate a change in the quality of the enamel.
Various pathological processes occurring in the body have a more significant impact on the condition of the enamel. The cause may be carious lesions, the use of medications, or a lack of certain microelements in the body. Teeth can take on a gray, pinkish, brown, purple and even black tint.
When starting to treat a patient, the dentist excludes the development of chronic pathologies. After a course of therapy and stable remission is achieved, other causes of discoloration of the enamel are eliminated. The final stage of treatment is a course of teeth whitening.
Specialists at the Consilium Dent choose the enamel lightening technique together with the patient. The selection criteria are age, condition of the enamel, and the wishes of the patient.
Retention period
Tortoanomalies corrected with orthodontic appliances require a long period of retention as the periodontal and interdental ligaments strive to return the tooth to its previous abnormal position.
Retention methods are divided into orthodontic, surgical and physiotherapeutic:
- Orthodontic retention primarily involves the use of lingual retainers bonded to the inner surface of the teeth. The device used to correct the anomaly can also be used as a retainer.
- The surgical method of retention involves dissection of the interdental papillae with ligaments that tend to return the displaced unit to its previous position.
- The physiotherapeutic method consists of vibration stimulation of the rotated tooth with a frequency of up to 50 Hz. Vibrations are accompanied by repair of the bone tissue of the alveolar sockets, which helps maintain the tooth in a rotated position. Vibration stimulation sessions are carried out several times a week.
The retention time by orthodontic methods depends on the severity of the tortoanomaly and the correction method used, and can be several months.
Position anomalies
Incorrect position of teeth always develops as a consequence of another pathology and forms an incorrect bite. May affect one or both jaws. Incorrect position of teeth makes chewing food and oral hygiene difficult. This can lead to digestive problems and the development of cavities. There are several options for the pathological position of teeth within or outside the dentition:
- External or vestibular position means that the tooth is located outside the dentition, closer to the vestibule of the mouth. This position is typical for canines and incisors and develops as a serious cosmetic defect.
- Oral or internal position. The teeth are deviated inward closer to the tongue. The disorder is typical for canines, incisors and premolars. May cause tongue injuries and dysfunction of the temporomandibular joint.
- Mesial and distal position. Dental units are displaced forward or backward along the dentition, which leads to its shortening.
- Supra and infraocclusion are high or low positions of teeth relative to the occlusal curve. The cause of the disorder is underdevelopment of the alveolar process. It appears due to the presence of some obstacle that interferes with the normal formation of the tooth germ. Effective therapy is surgery.
- Tortoanomaly. The tooth is rotated around a vertical axis. The disorder is typical for incisors, canines, and premolars. The anomaly can cause injury to adjacent teeth. Dental units are rotated into the correct position using orthodontic structures.
- Transposition. The teeth change their location with each other. The disease affects canines that exchange places with premolars or lateral incisors. The disorder develops at the stage of tooth germ formation. The therapy is as follows: problematic teeth are removed followed by prosthetics.
- Crowding of teeth occurs due to lack of space when tooth germs are located too closely. Crowded teeth are closely adjacent to each other and rotate around their axis. Occurs in combination with macrodentia or with an undeveloped basal part. To eliminate the violation, some dental units are removed.
- Diastemas and tremas are wide spaces between teeth. The disorder develops as a consequence of an abnormal shape and size. The problem is treated with orthodontic methods or by installing veneers, which helps restore the aesthetics of the smile.
Misaligned teeth cannot always be cured using braces. Severe pathology, which is characterized by a skeletal disorder of the maxillofacial region, is treated with surgical reconstruction. The pathological fragment is transferred to the desired position and then secured. A fragment containing part of the dentition or the entire dentition can be used.
General overview
Tortoanomaly is the most common violation of the position of individual teeth. According to various sources, it occurs in 10-20% of all diagnosed disorders.
The anomaly is a rotation of the tooth around a vertical axis, the magnitude of which can vary from several to 180°, that is, the position when the lingual (palatal) surface becomes vestibular.
The most common case is a rotation of approximately 45°. The maxillary lateral incisors are most often affected by tortoanomalies, and the lateral incisors of the mandible are somewhat less common.
But in principle, any element can, for one reason or another, be rotated relative to its longitudinal axis.
The most common reason why patients consult a doctor with a thoracic anomaly is dissatisfaction with the aesthetics of their smile. But when the anomaly is significant, functional problems arise along with aesthetic ones.
People begin to experience difficulty biting and chewing food, the tongue and mucous membrane of the cheeks are injured by the abnormally located unit, and they lose clarity of speech.
Diagnostics
An experienced dentist diagnoses dental abnormalities after an external examination and questioning of the patient. To clarify the diagnosis and identify the causes of the disease, a more detailed examination of the dental system is carried out:
- The construction of diagnostic plaster models and odontometric measurements make it possible to accurately identify changes in the size of dental units and their characteristics, which indicate the presence of pathologies.
- The color and transparency of the enamel are determined using a photographic method.
- Computed tomography or teleradiography makes it possible to obtain information about the condition of abnormal dental units in order to determine further treatment tactics.
- Panoramic radiography of the jaws is an important diagnostic method
- Electromyography of the jaws helps to assess the functional state of the facial muscular system.
To carry out differential diagnosis, the patient is referred for consultation to specialized specialists: endocrinologist, otolaryngologist, geneticist. Based on the diagnostic results, the attending physician determines treatment tactics. Depending on the type of disorder and the complexity of the disease, the patient may need the help of a dentist, surgeon, orthopedist, or implantologist.
Diagnostic measures
The pathology is easily diagnosed by examining the oral cavity. However, finding out its causes, assessing the position and condition of the roots and periodontium, necessary to draw up a treatment plan, usually requires additional research.
These include the following:
- X-ray (orthopantomography, targeted images). This is the main diagnostic method in dentistry, showing the condition of the periodontium and roots.
- CT scan. It is used when it is necessary to clarify the details of the subgingival part.
- Anthropometric and biometric studies. They allow you to determine the angle of rotation of the crown, the presence or absence of macro- and microdentia, and other features of the morphology of the elements of the dentofacial apparatus.
- Assessment of bite and occlusion using diagnostic models made from impressions of the jaws.
- T-scan is a computer method for analyzing occlusal contacts from Tekscan. Occlusion diagnostics T-scan is designed to identify problems with bite, accurately identify problem units, the closure of which causes improper distribution of the chewing load.
It is extremely rare that all or at least most of the methods listed above are necessary. However, it is useful to know about them in any case.
Prognosis and prevention
Consilium Dent clinic uses advanced methods of therapeutic, surgical, and orthopedic treatment of dental anomalies in patients. By skillfully combining them, experienced specialists are able to restore the aesthetics of a smile and ensure the normal functioning of the dental system, even if the degree of deviation is significant.
Prevention of anomalies in the formation and development of dental units begins during the period of intrauterine development of the fetus and is carried out throughout a person’s life. The main stages are as follows: monitoring the successful course of the prenatal period, caring for harmonious postnatal development, organizing a correct lifestyle while the baby is growing up, caring for dental health and general health throughout life. By conducting an annual preventive examination, the dentist identifies dental anomalies at an early stage, when the pathological process is still reversible.
Expert of the article you are reading:
Symptoms and signs
The degree of violation of aesthetics and functionality depends on the severity of the problem. With a slight turn, only aesthetics suffer, and even then not very much. However, if the rotation exceeds 20°, problems arise with the functionality of the dentofacial apparatus:
- The person begins to experience difficulty biting and chewing food.
- The abnormal tooth injures the tongue and the mucous membrane of the cheeks and lips.
- Begins to suffer from stomatitis.
- Experiences problems with speech.
Adaptation to the anomaly can lead to persistent malocclusion and occlusion with all the ensuing negative consequences - diseases of the gastrointestinal tract, dysfunction of the temporomandibular joint, etc.
Psychological trauma due to the deterioration of the aesthetics of a smile cannot be ignored. In any case, tortoanomaly worsens the quality of life, and even if it is mild, it deserves to see a doctor.