The result of dental canal treatment is the preservation and restoration of a tooth that is infected or has other pathology. The main task here remains cleaning the root canal. Infection and dying tissue must be removed from it. The resulting cavity is then securely filled. If treatment is not started in time, the inflammatory process will spread further and the tooth will have to be removed.
What is a root canal
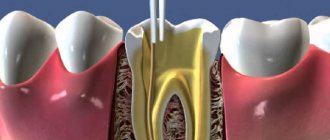
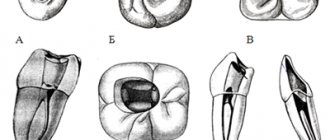
In addition to enamel and dentin, any tooth has a fairly large internal cavity. Its main part is called the pulp chamber. Thin tubules extend from it. They are located along the entire length of the roots. These are root canals. The number of roots varies among different groups of teeth. Accordingly, the number of channels is also different. The front teeth have only 1 canal. Side groups can have from 2 to 4.
Dental tubules are narrow tubes with many branches. They originate at the top of the root. This place is called the apical foramen. From here, neurovascular tissue passes to each root. If it is inflamed or dead, it is removed during endodontic treatment. Next, the resulting cavity is cleaned of its residues, disinfected and sealed.
Root canal treatment
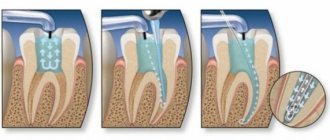
Root canal treatment takes place in several stages. Before treatment, X-rays or computed tomography must be taken. Using CT or X-ray images, the doctor will determine the approximate length of the root canals, shape, and the presence of obstacles to their cleaning.
Preparation for root canal treatment involves administering anesthesia and isolating the tooth from saliva using a rubber dam. If a tooth is severely damaged, the doctor can first restore its walls using temporary filling material.
When is endodontic therapy needed?
Strict indications are required for dental canal treatment. After all, if the neurovascular tissue is removed, the tooth loses strength and becomes susceptible to destruction. Therefore, endodontic treatment should be carried out only in cases of inflammatory processes or traumatic injuries. The most common are:
- Pulpitis. This is an inflammation of the neurovascular tissue (pulp). It is a soft, fibrous substance. In addition to blood vessels and nerve endings, it includes connective tissue and lymphatic vessels.
- Periodontitis. Inflammatory process in the root and adjacent tissues.
These diseases have the following symptoms:
- Swelling of the gums and changes in its color, the appearance of fistulas and purulent formations on it.
- Acute pain in the tooth that is aching or throbbing. It gets worse at night or with pressure.
- Putrid odor from the mouth.
Sometimes these symptoms may be absent. In such cases, inflammation is determined only upon examination. Only a specialist can make a conclusion about the need for endodontic treatment. He selects the most effective treatment regimen depending on the situation.
Treatment of instrumentally inaccessible (impassable) canals
The patency of the root canal depends mainly on the degree of its curvature and the location of the curvature:
— up to 25° — the channel is instrumentally accessible;
— from 25 to 50° — the canal is difficult to access instrumentally;
— from 50° — the channel is unavailable.
The location of the curvature closer to the mouth part makes it possible to expand the mouth part and facilitate the passage of the root canal even with significant curvature. There are other possible causes of canal obstruction. In the presence of hard-to-reach and inaccessible canals, devital amputation followed by mummification of the root pulp is indicated in the treatment of pulpitis. For this purpose, it is possible to impregnate (soak) the root canals with a liquid filling material containing resorcinol and formalin. For example, forphenan, foredent, etc. In addition to resorcinol and formalin, the liquids contain a catalyst for the polymerization reaction. Under the influence of a catalyst, the liquid turns into a glassy mass. Impregnating compounds have the ability to penetrate microtubules of hard dental tissues, providing a disinfecting and blocking effect. They can stain the tooth.
For impregnation, solutions and pastes containing parachlorophenol (cresodent, cresophen, cresopath, etc.) are used. Their antimicrobial effect is associated with the denaturation of microbial proteins in the canal. The material hardens by binding to the intracanal fluid.
Impregnation of instrumentally inaccessible channels can also be carried out using the silvering method, using an aqueous (30%) or alcoholic (3%) solution of silver nitrate. A 4% hydroquinone solution is used as a silver reducing agent. Sterilization of root canals by this method is based on the property of silver nitrate to diffuse deeply into the dentinal tubules, have a pronounced bactericidal effect, and obstruct the dentinal tubules by forming a film (silver mirror reaction). Treatment is also carried out in three visits. Silver ions can also be introduced into the channels using electrophoresis. The method is popular in children's practice.
Currently, as an alternative, a method of treating hard-to-reach canals has been proposed - depophoresis.
copper-calcium hydroxide, which is also carried out in two or three visits. When using this method, tissues are saturated (creating a depot) with ions of calcium hydroxide, copper hydroxide, and hydroxyl group. Filling the traversed part of the root canal is carried out with atacymite. A prerequisite is the passage of the canal by 1/3 - 2/3, preventing the entry of copper-calcium hydroxide into the periapical tissue. According to Professor Knappvost, under the influence of an electric field, copper-calcium hydroxide, penetrating into the canal system, ensures sterilization of the canals and root dentin and obturation of the holes.
5. Homework:
1. Write out the classification of means for irrigation and disinfection of root canals.
6. Literature:
Petrikas A.Zh. Pulpectomy. A textbook for dentists and students. — 2nd ed. - M.: AlfaPress, 2006. - 300 p.
2. Cohen S., Burns R. Endodontics: Trans. from English - St. Petersburg, 2000.
3. Poltavsky V.P. Intracanal medicine: Modern methods. - M.: Medical Information Agency LLC, 2007. - 88 p.
7. LEARNING OBJECTIVES:
1. Patient Z. came to the clinic with complaints about the presence of a carious cavity in the tooth, food retention between the teeth.
Objectively: on the chewing surface of tooth 37 there is a deep carious cavity filled with softened dentin and food debris. Temperature tests are weakly positive, probing the bottom of the carious cavity is slightly painful. Electroodontodiagnosis of the tooth (EDD) was carried out; the obtained values were 40 mA.
Make a diagnosis. Make a treatment plan.
Old methods of root canal treatment
Previously, endodontic treatment involved removing the pulp. For this purpose, for example, arsenic paste was used. It was inserted into the affected cavity and contributed to the death of the tissue. After this, the doctor removed the pulp from the tooth and filled it. This was the end of the treatment. Another common method was the placement of a resorcinol-formalin mixture. It froze in the cavity, thanks to which it was possible to stop the disintegration of tissues.
These methods had the following major disadvantages:
- Resorcinol-formalin and arsenic mixtures do not always completely kill the nerve. Therefore, when healing tissue, the patient could experience acute pain.
- Arsenic and resorcinol-formalin mixture are very toxic. They can accumulate in different organs.
- After pulp removal, tissue may remain in the root canals. Often they caused re-inflammation.
These methods of endodontic treatment were used due to the lack of adequate anesthesia, under which the affected pulp could be completely removed. Today dentistry has much more gentle methods.
Solving problems with very curved channels
The ultimate goal of endodontic treatment is to prevent the development of periapical lesions, as well as to create an environment conducive to their healing. To achieve such goals, it is necessary to adhere to certain classical principles of chemical disinfection and mechanical treatment of the root space. It is important to note that it is the success of the mechanical treatment of the endodontist that determines the effectiveness of all subsequent iatrogenic manipulations performed in the root canal.
For reliable obturation of the canal space with gutta-percha, it is necessary that it meet certain criteria, including:
- continuous conical shape of the main root canal, resembling a tapering funnel from the mouth to the apical foramen;
- narrowing of the cross-sectional diameter of the main canals in the apex area;
- preservation of the original shape of the channel during its processing;
- maintaining the original position of the apical foramen;
- maintaining the size of the apical foramen whenever possible.
The biological purpose of mechanical treatment of the endodontic space is as follows:
- restriction of the work of endodontic instruments within the boundaries of the root canal;
- prevention of extrusion of necrotic tissue into the postapical region;
- removal of all organic tissues from the space of the main and additional canals;
- creating a space of sufficient size to ensure effective irrigation and medicinal treatment without compromising the functional state of the tooth through excessive reduction in the thickness of dentin tissue.
Achieving the above goals in straight root canals is a fairly clear and logical process, however, in cases where there are various forms of anatomical variations in the endospace, this task becomes noticeably more complicated. It is especially difficult to achieve an adequate result of mechanical treatment of the canal in those with a pronounced bend of the endospace or in the presence of furcations and additional anastomoses (photo 1). It is quite difficult to follow classical intervention algorithms in such cases, therefore, to solve such problems, special NiTi files were developed, the sequence of application of which using the TCA technique helps to optimize the results of machining.
Photo 1a-c. Complex anatomical structure of root canals.
Treatment of canals with bends
Based on canal curvature, Nagy et al classified root canals into the following four categories:
- Straight or I-shaped (28% of root canals);
- Apically curved or J-shaped (23% of root canals);
- Curved along the entire length or C-shaped (33% of root canals);
- Multiple curved or S-shaped canals (16% of root canals).
Schäfer et al found that 84% of the root canals they studied were curved, while 17.5% had a second curvature and were classified as S-shaped. Of all the root canals with curves analyzed, 75% had a curvature level of less than 27°, 10% had a curvature ranged from 27 to 35°, and 15% had a pronounced curvature of more than 35°.
Traditionally, the severity of root canal curvature is described using the Schneider angle parameter: root canals with a bend of up to 5° are classified as straight canals, with a bend of 10 to 20° as moderately curved, and canals with a curve of more than 25° as severely curved. curved. Decades later, Pruett et al reported that two curved root canals can have the same Wein angle but completely different curvature parameters. To evaluate the latter, the radius of curvature parameter was introduced, which is defined as the radius of a circle passing through the curvilinear part of the channel. When using rotary tools, the number of cycles until the tool fails is significantly reduced as the radius of curvature decreases and the angle of curvature increases. Further attempts to mathematically describe the curvature of the channel on the basis of available two-dimensional radiographs led to the introduction into the theory of such parameters as the length of the curvature and its location, determined by the height and distance of the curvature. Estrela et al described a method for determining the radius of curvature of the root canal using CBCT slice data, which the scientists analyzed in specially developed software. According to their approach, the following three categories of root canal curvature were identified: small (r=4 mm), intermediate (r=4-8 mm) and large (r=8 mm). The smaller the radius of curvature, the greater its steepness. All of these attempts to describe root canal curvature had one goal: to develop an approach to assess the risk of apical foramen transportation and unexpected instrument separation.
Transport of channels and separation of instruments
According to the Glossary of Endodontic Terms, canal transport is the removal of the root canal wall structure on the outer side of the curvature in the apical half of the canal due to the properties of the files to restore their original linear shape. For stainless steel hand files and hand and machine NiTi files, the shape recovery properties are directly related to the size and taper of the tool. The larger the size and taper of the file, the more the file tries to restore its original shape, which is associated with an increase in the mass of metal in the structure of the tool. If the files exactly repeated the morphology of the endospace, then problems with transporting the canals would not arise at all, since in such an ideal situation the file would move strictly along the trajectory of the canal. Because the shape of the channels and instruments is different, each instrument moves along its own path within the curved channel, which is determined by its ability to recover. When attempting to increase the size of the apical foramen during mechanical treatment, as a rule, the amount of reduction of dentin tissue on the outer apical part of the curvature increases. To prevent this effect, doctors try to use instruments of a larger cone, but of a smaller size, for mechanical processing of the apical space in canals with pronounced curvature. Increasing the cone with this approach leads to a reduction in the angle of the bend, a decrease in its length and an increase in the radius with a reposition of the bend more apically (photo 2).
Photo 2. Treatment of the endospace leads to changes in bending parameters.
Reducing the volume of treatment of the apical part of the canal in those with pronounced curvature is indicated with the need to achieve the following goals:
- a smaller preparation diameter is associated with a smaller volume of canal wall reduction, a smaller increase in file size, and therefore with a lower risk of developing undesirable effects;
- files of smaller diameter are characterized by greater elasticity and less resistance to fatigue, thus, when working with these files, the possibility of transporting the canal as the size of the apical foramen increases is reduced.
The above-mentioned approaches to instrumental treatment of root canals, although safer, are also characterized by a number of disadvantages. Firstly, an increase in the taper of the endospace in its coronal part to ensure easier patency in the apical third provokes excessive reduction of dentin tissue, which compromises the biomechanical prognosis of the tooth. In addition, processing canals with smaller files makes it difficult for irrigation solutions to penetrate to the appropriate depth of the endospace. In canals with pronounced bends, the possibility of adequate irrigation of the root canal directly depends on the possibility of sufficient instrumental expansion of the apical third. Apical preparation of the apical part of the canal in order to achieve the appropriate level of disinfection in conditions of pronounced curvature is one of the most difficult practical tasks in endodontics, especially considering the prevalence of modern principles of minimally invasive interventions. In addition, there is a high risk of separation of rotary mechanical files in canals with pronounced curvature. The causes of such complications can be two main mechanisms: cyclic fatigue and torsion fatigue. When a rotary tool is activated within a curved channel, constant tensile and compressive stresses are generated within the physical center of rotation of the curvature. If the tip of the file is blocked in the endospace structure and the motor continues to rotate, the shear moment of the tool material exceeds its limit values, which also leads to the development of maximum levels of torsional fatigue (torsional fatigue). The greater the complexity of the morphology of channel bends, the fewer cycles of operation under such conditions the instrument can withstand.
Using Shape Memory Controlled Files
NiTi alloys are softer than stainless steel, but have a lower level of elasticity (about one-fourth to one-fifth that of stainless steel). At the same time, this material is more durable, rigid and elastic, due to which NiTi files are characterized by shape memory. NiTi files used in endodontics contain approximately 56% nickel and 44% titanium. However, they can exist in the form of two different temperature-dependent crystal structures called martensite (low-temperature phase) and austenite (high-temperature phase). The lattice organization can be transformed from austenitic to martensitic state by controlling temperature and stress. During the reverse transformation, the alloy passes through an unstable intermediate crystallographic phase called the R phase. The use of files during endodontic treatment provokes the development of stress, which, in turn, causes an instantaneous martensitic transformation of the NiTi file. A change in the shape of a tool is associated with a change in the parameters of its volume density. It is this property of the file, which is the ability to withstand stress without developing permanent deformation, that is called superelasticity. Superelasticity is most pronounced at the beginning of stress development, when the tool can easily overcome up to 8% deformation. After 100 deformations, this level drops to 6%, and after 100,000 – to 4%. It is within these boundaries that the shape memory effect is observed. In addition to stress, martensitic transformation of a file can also be caused by temperature changes. When the austenitic phase of a NiTi file cools, it begins to transform into martensitic phase. The temperature at which the martensite phase is completely restored again is called the temperature of the final transformation of martensite. When the martensite phase is heated, it begins to transform into the austenite phase. The temperature at which this phenomenon begins is called the temperature at which the austenite phase begins. At the final transformation temperature of austenite and above (Af), the material completes its shape memory transformation and demonstrates its superelastic properties. Until 2011, the Af temperature for most available NiTi tools was at or below room temperature. As a result, during clinical use, conventional NiTi files were in the austenitic phase, exhibiting their shape memory and superelasticity properties. In 2011, COLTENE introduced controlled shape memory files (CSF). The production of these tools involves the implementation of a unique thermomechanical process that controls the memory of the material, providing special elasticity and durability of the files, which is not typical for all other types of NiTi analogues. The Af-transformation temperature of CPF files is clearly higher than body temperature, as a result of which these files are in the martensite stage during operation in the endospace. In this phase, the instruments remain soft, plastic, without shape memory, and can be easily deformed, but after that they restore their shape and original elastic properties when heated to temperature Af.
A hybrid martensitic microstructure, like that used in HyFlex CM (COLTENE) files, also has a higher level of strength than an austenitic microstructure. At the same stress intensity, the rate of crack propagation in the structure of the austenitic phase is much higher than in the martensitic phase. A quantitative model for studying the process of crack development in the file structure made it possible to establish that the martensitic transformation of NiTi files increases the fracture strength of the tool by 47%.
More recently, the thermomechanical processing mechanism of CM has been combined with the mechanical fabrication procedure of NiTi files. Thanks to electrical discharge machining (EDM), it was possible to increase the surface hardness of files, their cutting efficiency and achieve unique parameters of resistance to functional fatigue. In the first published paper that demonstrated the results of using these files, the surface of the instruments was described as typical after an intrinsically safe specific treatment, and the level of degradation remained quite low even after multiple endodontic procedures. The authors also found that these files have surprisingly high levels of resistance to cyclic fatigue, and have a high safety profile even when working in highly curved canals, which has been confirmed in laboratory conditions. Pedulla et al also reported higher fatigue resistance values for HyFlex EDM (COLTENE) files, even compared to reciprocating machining and M-wire files.
Unfortunately, the literature data concerning the study of flexural stiffness and fracture resistance during the development of cyclic fatigue were carried out on NiTi files at room temperature. However, room temperature is not clinically significant. The use of modern instruments takes place at body temperature, which automatically excludes the possibility of direct application of the findings of previous studies in clinical practice. It is apparent that the transformation temperature (Af) of NiTi files designed for rotary or reciprocating processing can influence their clinical behavior under normal human body temperature conditions. Hulsmann et al (2019) reported that ambient temperature has a 500% influence on the service life of endodontic instruments. If the transformation temperature approaches body temperature, this can cause tools to appear flexible and fatigue resistant, but in fact become more rigid and less fatigue resistant. The Af of HyFlex EDM files was found to be close to 52°C, which is much higher than body temperature. Temperature analysis of EDM files confirmed the presence of a monoclinic structure of B19 martensite and a rhombohedral R phase. Thus, EDM instruments are always in the rhombohedral R-phase and martensitic crystallographic state at clinically relevant temperatures during endodontic treatment. The martensitic structure at body temperature allows these files to have excellent flexibility and resistance to fracture, as well as the absence of restoring forces, making them ideal for use during the machining of curved or morphologically complex canals.
Sequence of using HyFlex EDM Max files when processing curved canals
EDM technology has made it possible to implement the principle of endodontic expansion with a single rotary file. Generally, in most clinical cases, a 25/~ HyFlex EDM OneFile can be used with short peck movements while being sure to keep the instrument edges clear of debris and provide adequate irrigation. The OneFile is characterized by a size of 25 with a taper of 0.08. In this case, the taper of 0.08 is constant in the upper apical 4 mm of the instrument, but gradually decreases to 0.04 in the coronal part of the instrument. The file is characterized by the presence of three different cross-sectional zones along the entire length of the working part (rectangular in the apical part and two different trapezoidal cross-sections in the middle and coronal parts of the instrument). Thus, the developers managed to increase the file’s resistance to destruction and its cutting efficiency. When wider apical preparation is required, the designer introduces the following three HyFlex EDM finishing files with constant taper (40/.04, 50/.03 and 60/.02). For narrowed and obliterated canals, as well as for thin, long and S-shaped canals and canals with more than a 27° bend and a radius of curvature of less than 5 mm, a single file protocol is not indicated. In such cases, it is necessary to combine tools in order to achieve the most predictable treatment result. This is why the developer has also provided the Max Curve HyFlex EDM tool sequence, which includes files 15/.03, 10/.05 and 20/.05. The use of these files allows us to minimize the process of increasing the taper of the endospace, thus ensuring the minimum possible reduction of dentin on the canal walls. The Max Curve HyFlex EDM tool sequence can be used with the tactile controlled activation technique. Once the canal is identified, the minimal carpet is recreated using a 10/.02 stainless steel hand file. The 15/.03 HyFlex EDM tool is then used to follow the path of the carpet. After this, the 10/.05 HyFlex EDM file is used to widen the middle part of the canal. The apical 3 mm of the 10/.05 file act as a guide tip (without adhesion to the canal walls, photo 3). File 20/.05 HyFlex EDM is used as a final file to achieve the final smooth shape of the canal. After expansion with a 20/.05 instrument, the canal can be obturated with a 20/.05 gutta-percha cone and GuttaFlow biothermal sealer (COLTENE). The file sequence is easy to remember and ensures efficient and safe treatment of the endospace even in the most difficult clinical situations.
Photo 3. Sequence of HyFlex EDM Max Curve files.
Tactile control activation
In order to minimize the approach of using files with increasing taper, a tactile-controlled activation technique was proposed (photo 4a). This mechanical endospace technique can be defined as activating the stationary file only after it has been completely inserted into the patent canal. Essentially, the activation of the file occurs after the tactile sensation of achieving maximum adhesion of the cutting grooves to the walls of the endospace. Passive (non-activated) application of files is also useful, especially in cases of limited oral opening and incomplete visualization of the working field. Tactile-controlled activation can be classified into that during tool movement and during tool withdrawal. After creating access to the pulp cavity and localizing the mouths of the canals, their patency is ensured by the 10/.02 instrument. After this, the 15/.03 file is installed in the tip and inserted into the endospace until maximum resistance is felt (point A, photo 4b).
The file is then activated and pushed in the apical direction until the activated file reaches the point of resistance (point B, Fig. 4c). After this, the file is removed from the channel. The cutting edges of the instrument are cleared of debris, checked for deformations, and irrigation of the endospace is provided. The second time the same file is introduced, which can now go deeper in a passive state (point B, photo 4d). Re-activating the file will allow the file to advance the required length closer to the apical foramen (point C, photo 4e–g). Work with this tool is stopped only after it reaches the working length (point D, photo 4h). After reaching the working length, begin using the second file in the Max Curve sequence according to the protocol described above.
Photo 4a-h. Tactile controlled activation.
The thin apical 2 mm of a 10/.05 file will always remain free within the canal, which guides the file along the path of the endospace anatomy without the risk of developing excessive retention and breakage. File 20/.05 will ensure the final formation of the endospace and the conditions to ensure its proper disinfection and obturation. Mechanical processing of wider apical openings is achieved by increasing the width of the instruments used in particularly complex canals, such as those shown in photos 5 and 6; The use of a 20/.05 file would be most indicated, given the need to achieve proper disinfection of the endospace and minimize the risk of instrument separation. The TKA technique aims to minimize the time it takes to expand the endospace with an activated file, using file activation only when necessary to advance the instrument. With this approach and through the use of HyFlex EDM Max Curve files in a sequential manner, most anatomical variations of root canals can be treated without compromising the safety profile of the procedure.
Photo 5a-g. Treatment of the S-shaped mesiobuccal canal of the maxillary second molar using HyFlex EDM Max Curve files using the TKA technique: a) pre-treatment radiograph; b) radiograph after treatment; c) formation of the access cavity; d) view after processing with HyFlex EDM 15/.03 file; f) processing with HyFlex EDM 20/.05 file; f) obturation with gutta-percha pins 20/.05; g) view after obturation.
Photo 6a-d. Treatment of the S-shaped mesial canal of the mandibular second molar using HyFlex EDM Max Curve files: a) visualization of deep carious lesions; b) view after processing with HyFlex EDM 15/.03 file; c) view after obturation; d) view after restoration.
conclusions
NiTi files with CM effect are extremely flexible and have excellent fatigue resistance. They can be activated within the canal and passively moved along the bending path, guided by the original anatomy of the endospace. The TKA technique allows minimizing the time of close interaction of files with root dentin. During mechanical processing of the endospace, constant feedback tactile control of the manipulation is provided. For particularly complex clinical cases, a special sequence of HyFlex EDM Max Curve files has been developed, allowing clinicians to stay in tune with constantly moving progress.
Author: Dr Antonis Chaniotis (Greece)
Modern methods of endodontic treatment
In the treatment of tooth canals today there are two approaches: therapeutic and surgical. Let's look at them in more detail:
Therapeutic treatment. With this method, it is possible to preserve the entire pulp or at least part. The drug is placed into the cavity. The pulp chamber is isolated using a special gasket, then the tooth is filled. The drug can also reach tissues through dentin. To do this, special bandages with antibiotics are applied to the tooth. This therapy is used only in the initial stages of the inflammatory process.
Surgery. In this case, the pulp is completely removed, the canals are cleaned, disinfected and sealed. There are the following methods for filling cavities:
- Classical. The canals are filled with conventional filling material.
- Vertical filling. A special filling composition is administered as an injection.
- The use of thermophiles. A special heated composition on a carrier is placed into the cavity.
Sometimes, in order to cure the canal, you have to remove the tip of the root. This measure is necessary for cysts, granulomas, perforations, fibroids and other problems.
Stages of treatment
The Dentpremium Center provides dental canal treatment in stages. At the first appointment, the endodontist conducts an examination and diagnosis.
If root canal inflammation is suspected, radiography must be performed to determine the location of the lesion. Additionally, a computed tomography or orthopantomogram may be performed. After receiving all the data, the doctor determines the method of therapy.
Main stages of endodontic treatment.
- Pulpectomy. The endodontist anesthetizes the affected area, opens the tooth, and removes all necrotic and inflamed tissue. Giving the desired shape to the channels. Antiseptic treatment.
- Filling. Hermetically filling open cavities with a high-quality and safe filling composition: plastic (paste, gutta-percha), hard (pins) or hardening (cement materials). Filling using hot gutta-percha is considered the most effective.
- Crown restoration. The specialist’s task at this stage is to restore the anatomical shape of the tooth. For this, a filling (direct method) or a crown (indirect method) is used.
In case of inflammation of the dental canals, treatment is performed using strong anesthetics. Insufficient anesthesia can lead to pain, since the dental canals and pulp are connective and soft tissues equipped with nerve receptors.
At the Dentpremium clinic, specialists use only modern anesthetic drugs, which effectively anesthetize the area where the endodontist works for 2 hours. Treatment lasts from 30 minutes to 1 hour. In severe cases, it can take up to 2 hours. If sensation is restored during the procedure, another injection of anesthetic may be given.
Stages of endodontic treatment
- Diagnostics. If there is a suspicion of problems in the dental canal, an x-ray is taken. The specialist can also study the images that the patient already has. Depending on the diagnostic indications, treatment is selected.
- Pulp removal. First, the dentist anesthetizes the tooth. Then he opens it and removes all damaged tissue. Next, the cavity is given a convenient shape. Then the channels are disinfected using a special solution.
- Root canal filling. The cavities are filled with special materials. They are divided into hard (pins), hardening (various cements) and plastic (paste or gutta-percha). The most modern are the latter.
- Tooth restoration. This is the restoration of the shape of a tooth using a filling, crown or inlay.
Root canal instrumentation techniques in different age groups: a comprehensive narrative review
Introduction
As the world population grows, there is both an increase in life expectancy and a decrease in tooth loss. Because root canal treatment is performed on patients of all ages, clinicians should be aware of differences in root canal system morphology and dentin structure depending on patient age.
It is known that it is almost impossible to create guidelines or instrument calibers that would guarantee adequate root canal preparation in any age group. However, due to differences in canal morphology and dentin structure, as well as the use of different endodontic instruments and techniques available today, the clinician may use different methods to instrument the root canal system. Meanwhile, various tools—especially canal shaping files made from different heat-treated alloys with different geometric characteristics—are reported to have distinctive mechanical properties and resulting positive processing results. The choice of instruments may lead to inadequate clinical results in certain cases, depending on the properties of the instrument and the clinical condition of the patient, including age. Therefore, the purpose of this article is to review age-specific clinical guidelines for root canal instrumentation techniques through a literature search and review.
Review and search of literature
An electronic literature search was conducted, including MEDLINE (Ovid), PubMed, and Web of Science databases. The search used dictionary terms and arbitrary phrases, such as: “root canal treatment depending on age”, “root canal instrumentation depending on age”, “chemomechanical preparation depending on age”, “clinical recommendations in endodontics depending by age”, “toolkit for root canal treatment at different ages”, “geriatric root canal treatment” and “childhood root canal treatment”. However, a review of the literature revealed a lack of studies with practical clinical recommendations when selecting appropriate instruments for age-related root canal treatment.
Therefore, a comprehensive review of canal morphology, dentin structural characteristics, and endodontic outcomes in different age groups was taken from articles that were published from 1925 to 2018, rather than a systematic review. Previous studies have used different approaches to classify age-related morphological and structural changes, either based on statistics (to ensure a larger sample size) or without explanation of the classification. This review categorizes age differences into the following age groups: persons aged 20 years or younger, 21 to 40 years, and 41 years or older.
Morphology of root canals depending on age
- Contour and cross-sectional diameter of the channel
Differentiation of the root canal system due to the deposition of secondary dentin is an age-related process. With age, the pulp cavity usually decreases in size (Fig. 1).
Rice. 1. Panoramic radiographs showing the size of the pulp chamber and root canal depending on age. (A) Persons under 20 years of age (13 years), (B) persons between 20 and 40 years of age (39 years), (C) persons over 40 years of age (64 years). Image (A) shows the large pulp chamber and the direct direction to the canal opening. Image (B) shows the denticulate area and the direction at an angle to the canal orifice. Image (C) shows a small area of the pulp chamber and sclerotic canals.
Typically, people under the age of 20 have roots with one large root canal (mostly oval). Median mesial canals in mandibular molars are found mainly in individuals under 21 years of age. Individuals between the ages of 20 and 40 have several separate canals in one root. The number of root canals was found to increase mainly in the maxillary and mandibular second premolars, the distal root of the mandibular first molars, and the mandibular incisors. In patients over 35 years of age, more round canals were found in the mandibular second molar, while in those under 35 years of age, more oval canals were found.
The C-shaped configuration (type III) is more common in mandibular molars in individuals under the age of 40. In a study using cone beam computed tomography, patients younger than 42 years were 4 times more likely to encounter a mesial canal than patients older than 42 years. In people over 40 years of age, the deposition of secondary dentin leads to a decrease in the diameter of the canal and the disappearance of additional canals. Fewer canals were found in individuals aged 51–70 years. For example, in this age group, the absence of the second mesiobuccal canal in the maxillary molars was observed.
- Isthmuses
The incidence of canal isthmuses appears to be related to age. People under 20 years of age have wide and oval canals without isthmuses in the early stages of root development. In people aged 20 to 40 years, the deposition of secondary dentin in the mesiodistal direction leads to the formation of 2 canals with an isthmus. Up to 81% of mesial roots of mandibular first molars in individuals aged 20-39 years have isthmuses, especially at a distance of 4-6 mm from the apex. In persons over 40 years of age, the extent and number of isthmuses are significantly reduced, and the canal is completely separated. In people over 50 years of age, the incidence of isthmuses was 16.7%, and only 24% of people over 60 years of age had isthmuses in the mesial roots of mandibular molars. The ratio of partial isthmuses to complete isthmuses increases with age. Figure 2 shows isthmus characteristics in different age groups with cone beam computed tomography images.
Rice. 2. Cone beam computed tomography: three images of the mandibular first molar showing isthmus characteristics in different age groups. (A) Persons under 20 years of age (18 years): wide canal without isthmus, (B) persons 20 to 40 years of age (38 years): isthmus in the mesial root, (C) persons 40 years of age or older (62 years) : sclerotic mesial canals without isthmus, similar to one canal.
Age-related changes in dentin structure
With age, normal dentin undergoes physiological changes and turns into transparent (sclerosed) dentin. As the tooth matures, peritubular dentin becomes more mineralized and a decrease in the average number of dentinal tubules is observed. The process of mineralization and dentin sclerosis lead to narrowing of the tubules. In some cases, this process can lead to complete obliteration of the dentinal tubules. Mineralization begins in the third decade of life in the apical zone and develops coronally with age.
The penetration of bacteria into dentinal tubules may be a determining factor in their virulence in the root canal environment. Microbial diversity and microbial load are higher in young people and decrease with age. This decrease may be due to mineralization of the tubules, as well as a decrease in the space of the pulp cavity, isthmuses and accessory canals. Dentinal tubules typically have a larger diameter than the average diameter of Enterococcus faecalis (E. faecalis) cells by approximately 0.8–1 nm. However, due to age-related mineralization of the tubules in old age, the depth of penetration of E. faecalis into dentin through sclerotic or obliterated tubules decreases. On average, bacteria penetrate 65 microns less deeply in people aged 60–77 years than in people aged 18–24 years.
With age, the water content of dentin decreases and collagen modifications, such as cross-linking, increase. Because of these age-related changes, resistance to dental damage decreases in older adults, but significant reductions in dentin strength and fracture strength result in an increased incidence of vertical root fracture (VRF). VRFs are most common in posterior teeth in patients between 40 and 60 years of age. In addition, the growth rate of vertical cracks in “old” dehydrated dentin is 100 times higher than in “young” hydrated dentin. Pre-existing dentinal microcracks in endodontically untreated roots become more common with age (8.3% in persons over 40 years of age, 3.7% in persons over 20–39 years of age). In contrast, in individuals under 20 years of age, the dentin walls are thin, which can lead to coronal or root fractures of the tooth under normal functional stress.
Results depending on age
Data on the effect of patient age on the results of endodontic treatment are contradictory. Some studies reported that age had no statistically significant effect on results, while others stated that patient age significantly affected results. Some studies have shown that treatment in older patients had a higher success rate than in younger patients, while other researchers have found better results in younger patients and have demonstrated that age is a risk factor for complications. For example, older patients are 1.4 times more likely to have teeth removed after root canal treatment. The rate of subsequent removal increases by 1–2% each decade until it reaches a plateau after age 60.
These better results in older people can be explained by the gradual reduction of the pulp space, the disappearance of additional canals and isthmuses and the narrowing of the dentinal tubules up to complete obliteration. These changes limit the volume available for infection, which ensures adequate cleaning of the canal, as well as its formation and medicinal treatment. Reports of better results in younger adults may be explained by the increased prevalence of apical periodontitis with age, which is associated with a lower likelihood of successful endodontic treatment. Another explanation could be that older people have slower and less efficient healing processes or longer healing times. Immunological changes that occur due to aging include changes in pulp cells expressing macrophage-associated antigens. Aging is associated with low levels of expression of genes encoding transcription regulators and high levels of expression of genes involved in apoptolytic processes.
In addition, systemic diseases are more common in older age groups, and it has been reported that some systemic diseases may be associated with endodontic treatment outcome. Diabetes (non-insulin-dependent or insulin-dependent) or an impaired nonspecific immune response leads to decreased success of endodontic treatment in patients with preoperative periradicular lesions.
Table 1 shows the characteristics of canal morphology and dentin structure in different age groups, including the contour and cross-sectional diameter of the canal, the presence and characteristics of isthmuses, accessory canals, the number and diameter of dentinal tubules, and sclerotic dentin. Taken together, these age-related changes suggest that clinicians may choose different clinical approaches for different age groups.
Table 1. Characteristics of the canal morphology and dentin structure in different age groups.
Possible clinical suggestions
Within the limitations of the studies that were reviewed, the following possible clinical recommendations for root canal instrumentation can be made. For persons over 20 years of age, the recommendations are as follows. Large channels do not require additional expansion. Scraping instruments may be preferred to clear the root canal wall of biofilm while simultaneously activating the irrigation solution. Possible tools: Self-Adapting File (SAF; ReDent, Ra'anana, Israel) and XP-Endo Finisher (FKG Dentaire, La Chaux-de-Fonds, Switzerland). These systems are effective in cleaning a relatively large and oval canal lumen with a cleaning action while constantly changing the irrigant for SAF or eccentric movements of memory-controlled instruments such as the XP-Endo Finisher.
For persons aged 20 to 40 years, the following recommendations exist. The channels are generally open and difficulties in creating a carpet are rare. In these root canal systems, conventional nickel titanium (NiTi) rotary systems can be used to shape the canal to size #30–#35 followed by sodium hypochlorite activation. Possible instruments: ProTaper Next (Dentsply Sirona, Ballaigues, Switzerland), XP-Shaper (FKG Dentaire, La Chaux-de-Fonds, Switzerland) and 2Shape (MicroMega, Besançon, France). The use of scraping instruments in this age group may be considered in oval canals.
For people who are 40 years of age or older, the recommendations are as follows. In these root canal systems, after using stainless steel hand K-files (#06, #08 and #10), the NiTi system can be used to create a carpet. Possible tools include G-File (MicroMega), PathFile (Dentsply Sirona), OneG (MicroMega), ProGlider (Dentsply Sirona), Scout RaCe and Race ISO 10 (FKG Dentaire). Thereafter, expansion of the apical diameter of the root canal to size No. 30 or No. 35 is preferably carried out using NiTi instruments, which place less stress on the dentin. Possible instruments for this purpose are instruments with a smaller cross-sectional area (MTwo [VDW, Munich, Germany], Race [FKG Dentaire], ProFile, 2Shape), instruments with a smaller taper (0.02 and 0.04) (Race, ProFile ) ) and made from flexible NiTi (memory controlled file), such as HyFlex (Coltene/Whaledent, Inc, Cuyahoga Falls, OH, USA) and Typhoon (Clinician's Choice Dental Products, New Milford, CT, USA).
Table 2 presents the proposed algorithm for root canal instrumentation in different age groups. The current suggestions are based on available evidence and reflect the limitations of the studies that were included in the review. However, no single algorithm fits all teeth. The clinician may encounter inconsistencies between chronological age and biological age. Pathological or iatrogenic factors can change the contour and cross-sectional diameter of the canal. These factors include carious lesions or extensive restorations, attrition or attrition, occlusal trauma, periodontal disease and treatment, and orthodontic treatment. The irritants that each tooth encounters during its life must be taken into account due to the possible rapid increase in reaction and dentin deposition. In contrast, pulp necrosis in younger patients due to trauma or caries can lead to the formation of wider canals with thin dentin walls as these patients get older.
Table 2. Algorithm for root canal instrumentation in different age groups.
The contents of this review do not necessarily support any specific technique for specific clinical situations in patients of various age groups and root canal conditions. However, it may be generally acceptable to emphasize the importance of chemomechanical preparation, which always improves canal clearance through shaping and activated irrigation, regardless of the patient's age and canal condition. Correct assessment of root canal morphology, coupled with an adequate understanding of the influence of age on these characteristics, can help the clinician select the most appropriate instrumentation technique and irrigation activation.
conclusions
The current review examines age-related differences in canal morphology, dentin structural characteristics, and endodontic outcomes. Depending on age, clinical recommendations for instrumentation should ideally be based on a systematic review of randomized controlled trials, taking into account the quality of evidence and patients' values, preferences and financial resources. However, no studies suitable for this purpose have been conducted. Thus, the present article is the first attempt to interpret age-related morphological and structural changes and make practical clinical suggestions within the limitations of existing studies.
A systematic review is a comprehensive method of finding relevant studies on a specific topic, and then the identified studies are assessed and summarized according to a predetermined and explicit method. In contrast, narrative review is a traditional method of peer review. This method is subjective and there are no formal rules for selecting studies or standard statistical methods for pooling studies. Therefore, when reading and evaluating a narrative review, readers should keep in mind that the author's bias may or may not be present.
An additional limitation of these proposed clinical offerings is that the aforementioned tools are not available to all clinicians due to local market conditions and financial resources. Future research should examine the influence of patient age on other aspects of root canal treatment (eg, access cavity preparation, irrigation techniques, and obturation techniques). It can be concluded that the clinician's awareness of age-related differences in root canal morphology and dentin characteristics may influence the choice of instruments for root canal treatment.
Source : Restorative Dentistry & Endodontics
Translation by Tatiana Chuiko for the BELODENT.ORG portal
Canal treatment using a microscope
The diameter of the root canal of a tooth is approximately 1 millimeter. In such conditions it is impossible to work with it without special optics. The dental microscope allows you to increase visibility up to 32 times. Therefore, it is increasingly used in modern dentistry.
Advantages of using a dental microscope:
- The specialist can see and remove only tissues affected by inflammation, without touching healthy ones.
- An excellent overview of the tubule orifices is achieved. Seeing the number of their branches, depth and directions is very important during endodontic treatment.
- Due to targeted treatment of the pulp, complications can be avoided. The possibility of perforations is also eliminated.
Features of the treatment of chronic periodontitis with poorly accessible root canals
To localize the mouths of obliterated canals, it is advisable to use caries markers. produces the drug “CanalBlue” in disposable plastic pipettes with a thin tip of 0.125 ml. After adding a marker to the bottom of the tooth cavity, it is washed with water and dried with an air stream. Usually, the painted dots in the places of hidden canal mouths are well contrasted. It is also advisable to use means of optical magnification (microscopes, endodontic video cameras, binocular loupes, etc.).
In order to facilitate the passage and expansion of narrow and obliterated root canals, two methods are used: mechanical and chemical. Thin drills (reamers) are traditionally used to pass through channels; thin K-files are also used for this purpose. The angles of rotation of instruments in a difficult-to-pass channel should not exceed 45-90°.
(USA) offers a thin carbon endodontic instrument “Pathfinder” in two sizes for passing obliterated canals - “C-pilotfile” in six sizes (06, 08, 10, 12.5 and 15), Dentsply / Maillefer Corporation » - “ProFinder” (series of “Senseus” instruments) sizes No. 10, 13, 17 according to ISC, length 21 and 25 mm.
If the tooth root canal has poor patency, a chemical method can be used to expand it. For this purpose, complex or chelate substances are used, which decalcify dentin. The most commonly used is the sodium salt of ethylenediamine tetraacetic acid (EDTA). As a result of contact of EDTA with the wall of the tooth root canal, the latter is decalcified and softened, which significantly facilitates the process of mechanical expansion of the tooth root canal.
The best decalcifying effect was observed when using 20% tri-sodium salt EDTA (Berezovskaya V.I., 1966). After drying the tooth root canal, the EDTA solution is injected into the passable part on cotton pads or using a syringe and injected with a root needle. After 30 seconds, the spent EDTA solution is removed with a cotton swab, this procedure is repeated for 5-8 minutes, after which they try to mechanically remove decalcified dentin from the tooth root canal. Considering that EDTA does not have a negative effect on the oral mucosa and periapical tissues, its solution can be left for 12-24 hours in the tooth root canal. The success of using EDTA depends on the freshness of the prepared solution and the length of time it remains in the tooth root canal.
EDTA in the form of a solution is contained in the preparations "Largalultra" (Septodont), Edetat (Pierre Rolland, France), Endofree (Dencare), RootCanalEnlarger (Dentaires), Chela-JenLiquid (“Alpha-BetaMedicalSupplyInc.”), “Kanal-Dent-E” (“VladMiVa”), SmearClear (“SybronEndo”), etc. It should be noted that the importance of these drugs is currently increasing; their use is recommended not only in difficult-to-pass canals, but also for medicinal treatment of well-passable canals in order to influence the smear layer of dentin on the walls of the canals of the roots of the teeth, alternating with irrigation with a 3-5% sodium hypochlorite solution (Gettleman V.H. etal., 1991; Chistyakova G.G. , Manak T.N., 2006, etc.).
The use of EDTA in gel form is recommended during mechanical treatment of tooth root canals; it significantly reduces the likelihood of endodontic instrument breakage and facilitates the passage of canals and giving them the shape necessary for filling. Representatives of this group of drugs are “Canal +” “Septodont”, “RC-prep”, “RC-lube” (PremierDentalProd), “HPU 15” (“Spad”), “Endo-gl” (“VladMiVa” ), “FileCareEDTA” (“VDW”), “Glyde” (“Dentsply”), etc. These drugs cannot be left in the root canal under a bandage.
To chemically expand the root canals of teeth, you can successfully use a 36% solution of metacresol sulfonic acid, i.e. vagotil, which has a decalcifying effect and at the same time is a broad-spectrum drug (Gunchenko L.S., I Bogatyreva V.A., 1990). Due to its viscous consistency, vagotil diffuses well into the narrow canals of the tooth root, exhibiting a decalcifying effect not only in breadth, but also in depth. In teeth on the lower jaw, it is convenient to apply the drug using the jaws of tweezers or a pipette at the mouth of the canal, and then use a root needle or thin drill to pump the liquid into the canal. Residues are removed with a cotton ball. In teeth on the upper jaw, it is better to introduce vagotil into the root canals of the tooth with a drill, on which a thin cotton wool is wound to hold the solution. Vagotil can be left in the root canal of the tooth on the turunda for 24-48 hours under an airtight bandage. In our opinion, it is advisable to study the possibility of using vagotil to remove the mineral component of the smear layer of the walls of the root canals of teeth. It should be taken into account that for the treatment of obliterated canals and effects on the smear layer in endodontics, it is possible to use citric and phosphoric acids (but not liquid phosphate cement!) in a concentration of 6% to 30% in combination with a solution of sodium hypochlorite, however, the use of EDTA has an effect on dentin has a more gentle effect. After applying the acid solution, it is recommended to rinse the canal with distilled water, since there is a tendency for crystallization and precipitate to form on the canal walls.
A special situation arises when it is necessary to unfill previously filled root canals. In this case, special preparations are used to distinguish between filling materials in the canals. Thus, to soften materials based on eugenol and zinc oxide, Endosolv E (Septodont), DPS 10 (Spad), Eugenat (Omega-Dent), etc. are used.
“EndosolvR” (“Septodont”), “Resosolv” (“Pierre Rolland”), “Fenoplast” (“Omega-Dent”), etc. are intended for softening materials based on a resorcinol-formalin mixture.
It is believed that the liquid and gel "Solvadent" ("VladMiVa") promote disobturation of canals after filling with both zinc oxide-eugenol materials and phenol-formaldehyde resins, glass ionomer and zinc phosphate cements.
According to our observations, in the treatment of periodontitis, the gel “CarisoM” (“MediTeam”) can be successfully used as a means for chemical expansion of the root canals of teeth. Used to lubricate files during canal machining.
Recommendations after endodontic treatment
After stopping the inflammation of the pulp, it is necessary to consolidate the result. To do this, the patient must adhere to the following simple rules:
- Do not eat spicy, cold or hot food for several days. You need to wait until the treated teeth lose sensitivity.
- Maintain oral hygiene. You need to brush your teeth and floss twice a day.
- Eliminate solid foods from your diet for a while. Failure to comply with this rule can lead to tooth decay.
- Go to the dentist for dental checkups 2 times a year.
After endodontic treatment, teeth will become especially sensitive. This is how the body reacts to the filling material. However, after a few days this effect will disappear.
Clinic doctors
Often during endodontic dental treatment, dentists encounter root canal obstruction (obstruction of the root canals of the teeth). But in most cases, this problem can be solved thanks to the high professionalism of specialists and the excellent equipment of the DentaBravo clinic.
Why does tooth root canal obstruction occur?
There are several causes of root canal obstruction:
- Anatomical structure of the root.
The canals may be flattened, curved, with small branches or transverse bridges.
- Inflammatory phenomena in the pulp. Chronic caries, subacute and chronic pulpitis, mechanical overload of the tooth provoke overgrowth of the canals.
- Age-related changes. Over the years, deposits of dentin or dentin-like tissue (denticles) accumulate on the walls of the canals. They narrow the lumen and often contribute to root canal obstruction.
- Treatment using phosphate cement. This is a dense material that cannot be removed by ultrasound, solvents, or mechanical methods.
How to determine tooth canal obstruction
Diagnosis of root canal obstruction is very important, because quality treatment requires careful preparation. And in order to freely manipulate during cleaning and expansion, the doctor must determine the working length.
The most common research method is radiography. A photograph of the root of a tooth with an instrument inserted into it makes it possible to see:
- tooth length;
- direction of movement of the endodontic instrument;
- obstruction of the root canals of the tooth;
- canal curvature;
- presence of perforation;
- periodontal condition, etc.
If there are symptoms of root canal obstruction, they need to be opened to the apical narrowing so that endodontic treatment can be carried out.
How is tooth canal obstruction treated?
Usually, when treating pulpitis or periodontitis, the doctor works with a pulp extractor. If there are no problems with the channels, then difficulties usually do not arise. But if the canal is curved, narrowed, closed, or adjacent to an adjacent root, a special approach is needed.
Treatment of root canal obstruction requires the use of special chemicals and a stronger extractor to avoid metal fatigue and instrument fracture. For example, nickel-titanium files (titanium needles) are used - rotating extractors, which make it possible to pass root canals without preparation and reduce the risk of pinching or breaking the instrument.
Also, in case of obstruction of the tooth canal, thin drill burs are used - instruments with spiral blades designed to eliminate old filling material (pastes, cements, gutta-percha).
Unsealing is also done using solvents that work well with soft and flexible materials. Difficulties arise with channels filled with resorcinol-formalin paste. When it hardens, it becomes very hard, and to eliminate the obstruction of the tooth canal it is necessary to use strong substances, drilling with a bur and nozzles with ultrasound. Unsealing a resorcinated canal is a long and labor-intensive procedure associated with the risk of tooth perforation. And if the patient has a phosphate-cement filling, the root is generally amputated or its apex is cut off.
Treatment methods for dental canal obstruction are selected individually. For consultation and diagnostics, sign up at the DentaBravo clinic!
Cost of services
Service Price
Dental canal treatment from RUB 3,000.
1-canal tooth (mechanical and medicinal treatment of the canal) 900 rub.
1-canal tooth (canal filling with gutta-percha pins) 750 rub.
2-canal tooth (mechanical and medicinal treatment of canals) RUB 1,500.
2-canal tooth (canal filling with gutta-percha pins) 980 rub.
3-canal tooth (mechanical and medicinal treatment of canals) RUB 2,100.
3-channel tooth (canal filling with gutta-percha pins) RUB 1,300.
Expert of the article you are reading:
Akhmedkhanov Said Rashidovich
Dental surgeon, general dentist, implantologist, orthopedic dentist, dental therapist.
You may also be interested in:
Dental treatment during pregnancy Dental consultation Treatment of dental cysts Increased sensitivity of teeth: causes and methods of treatment Filling of dental canals Treatment of pulpitis Treatment of fistula on the gums Treatment of flux (periostitis)
Show more
Is it painful to treat root canals?
Thanks to the use of modern anesthetics, root canal treatment has become a painless procedure. The patient may feel mild discomfort only during the injection of the anesthetic.
Therefore, there is no need to be afraid of root canal treatment; moreover, you must remember that you should never postpone the procedure due to fear of the dentist! Inflammation in a tooth that has progressed to a certain stage of development cannot be cured, which means that the diseased tooth will have to be removed and a prosthesis put in its place. In addition, more serious complications may occur.
Preparation for filling
Before filling the canals with filling material, the doctor must thoroughly clean them and prepare the cavity in a special way. This process takes place in several stages:
- Removal of affected tissue
Most often, the need for root canal treatment arises as a consequence of another pathological process, in particular caries. To destroy the source of infection and open access to the mouths of the canals, the dentist removes dead and diseased tissue using a bur. - removal
Pulp is the sensitive tissue of the tooth, a plexus of blood vessels and nerves located in the coronal part and inside the roots. The method of filling root canals involves removing the pulp using a special tool. Most often, this procedure, like the previous one, is performed under local anesthesia to eliminate pain and discomfort when removing the pulp. - Measuring canals
In order to perform a quality filling, the doctor needs to obtain as accurate information as possible about the properties and current condition of the canals. For this purpose, before treatment, as a rule, a targeted radiograph is performed. An important procedure is also measuring the length of the channels. The length is individual and depends not only on the size of the root, but also on the degree of curvature of the canal. - Mechanical processing
Before filling, the channels are cleaned and expanded using special tools. This is necessary to completely remove the affected tissue, as well as to more densely and evenly fill the canal cavity with filling material. Mechanical processing is performed using special thin tools - files. With the help of a file, the canal is passed completely, from the mouth to the apex.
Only after completing all the preparatory steps can the doctor proceed to filling.
What is a dental microscope and why is it needed when treating root canals?
A dental microscope is considered today one of the prerequisites for the work of a modern dentist. Meticulous and highly precise endodontic treatment is impossible without magnification. Using a microscope helps:
- Clean the canal in the most inaccessible places, without missing anything, using the finest tools
- Preserve the maximum amount of healthy tissue
- Find missed root canals
- Guaranteed to remove all dental tissue affected by caries
- See cracks in the tooth
- Carry out the procedure quickly and accurately, remove the remains of old restorations or a broken instrument in the canal (during retreatment)
- Eliminate the risk of complications
The doctors at our clinic have the best equipment to achieve ideal quality. Of course, endodontic treatment in our clinics is carried out only under a microscope.
Important: endodontic treatment is an indication for crown installation. Of course, after canal treatment, the doctor will restore the tooth with composite material, but such a tooth still needs to be strengthened with a crown. Therefore, after root canal treatment, contact our orthopedic dentists!