Diseases of peripheral processes
The main and most frequently diagnosed lesion of the peripheral plexuses, which is accompanied by functional disorders, is neuropathy or neuritis.
Symptoms characteristic of a violation of motor, sensory, and autonomic function occur. The person feels pain that radiates along the affected segment. Diseases that occur with dysfunction of the roots include: degenerative and dystrophic processes, metabolic disorders, inflammation of the roots and pinching by a tumor, osteophytes, hernia or other neoplasm.
Other peripheral plexus disorders:
- Optic nerves
- Diagnostics
- Cranial nerve examination
- Spinal cord, medulla spinalis. Development of the spinal cord.
- Neurology of motor nerves
- Second branch of the trigeminal nerve. Maxillary nerve, n. maxillaris. Pterygopalatine ganglion, ganglion pterygopalatinum.
- Vagus nerve (X pair, 10 pair of cranial nerves), n. vagus
- Functions of cranial nerves
- Taste nerves
- Treatment of the disease
- Diagnosis of neuralgia
- Sensitive nerve structures
- polyneuropathy, when several or many processes are involved in the lesion;
- plexitis is a disease characterized by damage to the entire plexus;
- radiculoneuritis is a simultaneous pathological process in the roots of the spinal canal and trunks;
- myeloradiculoneuritis - a condition characteristic of damage to the spinal cord, nerve trunks and roots;
- radiculitis – symptoms characteristic of injury to the spinal cord roots;
- ganglionitis is a pathological process characterized by damage to the intervertebral nodes.
Anatomical structure
Infraorbital nerve: anatomy
The infraorbital (or inferior orbital) nerve is the main branch of nerve fibers arising from the maxillary nerve, which follows from the ending of the trigeminal nerve.
The latter is the largest pair (fifth in a row) of cranial nerves. A branch of the trigeminal nerve emerges from the posterior part of the brain through the foramen rotundum in the sphenoid cranial bone.
In the temple area, the nerve roots unite into the trigeminal ganglion, which diverges into three branches:
- ophthalmic;
- mandibular;
- maxillary.
The optic nerve distributes nerve endings to the skin of the forehead, cheekbones, nose, and parts of the eyeballs. The mandibular nerve branch goes to the masticatory and other muscles of the oral cavity, the inner surface of the cheeks and lips.
The maxillary branch, running through the pterygopalatine fossa (slit-like space in the lateral part of the skull), branches into three continuations:
- zygomatic nerve;
- nodal nerve branches;
- infraorbital nerve.
Through the infraorbital fissure, the infraorbital nerve enters the orbital cavity, continues along the infraorbital groove and through the infraorbital canal, and behind it, the infraorbital fissure enters the canine fossa, located in the anterior facial part of the skull.
The size of the infraorbital nerve varies from person to person. With brachycephaly (small height of the skull relative to its width), the trunk can reach 27 mm. With dolichocephaly (the reverse ratio of brachycephaly), the length of the nerve trunk is up to 32 mm.
Along its entire length, the infraorbital nerve gives off several branches, which diverge into main and scattered types. The main type of discharge is characterized by the presence of a main trunk and several large nerves extending from it. The nerves that emerge from the scattered type are small, there are many of them, and they have many connections.
The infraorbital nerve diverges into:
- Superior alveolar branches. They are divided into front, rear and middle. These branches intertwine with the alveolar vessels and run along the upper jaw, uniting into the upper dental plexus.
- Nasal branches – internal and external.
- Upper labial branches.
- Lower branches of the eyelids.
The infraorbital nerve and its branches are closely intertwined with the processes of the facial nerve, forming a single network of nerve endings that determine the mobility and sensitivity of the facial muscles.
Optic nerves
Visual disorders such as decreased acuity, color perception, visual field impairment, and blindness cause damage to any part of the second pair of the cranial nerve - visual. The types of violations depend on the dislocation of the source.
Tubular vision manifests itself in neuritis of the second pair of cranial nerves, hysteria, glaucoma, arachnoiditis. Complete blindness - as a result of injury, pathology of the chiasm. The condition is assessed based on the results of an examination of the visual components (acuity, visual field, etc.) and the fundus.
Polychromatic tables allow you to assess the level of color perception. Visual defects (so-called scotomas) detected by an ophthalmologist signal a pathology affecting the optic nerve. Patients themselves rarely consult a doctor when the severity decreases. Amblyopia can result in amaurosis. Sometimes complete loss of vision is the result of advanced pathology, when the pathological process is irreversible.
First symptoms
Clinical signs of damage to the mandibular nerve are expressed in discomfort in the area of innervation: the area of the mental foramen, the lower lip, the membrane of the gums and cheeks to the borders of the second molar.
Pathology is expressed:
- Paresthesia – change in sensitivity (no painful sensations during injection, etc.).
- Dysesthesia is a change in sensitivity that brings discomfort (pain, “pins and needles”).
- Anesthesia – complete loss of sensitivity.
When extracting wisdom teeth, the lingual nerve is most often damaged (up to 2.1%). During implantation, damage to this nerve is less common and manifests itself with the following symptoms:
- increased salivation;
- speech defects;
- involuntary tongue biting;
- problems with swallowing;
- loss or change in taste;
- burning sensation of the tongue;
- numbness of the mucous membrane of the tongue and gums.
Up to 90% of lingual nerve injuries heal on their own within 7-10 weeks of onset.
Classification of manifestations
According to Seddon's classification, injuries to the trigeminal nerve are of several types:
- Neuropraxia. The damage is reversible. The sheath of the nerve fibers is not affected. There is no degeneration. Sensitivity returns a few weeks after treatment.
- Axonotmesis. Requires long-term therapy for up to six months. Fiber damage occurs and degeneration develops. The damage is reversible.
- Neurotmesis. Nerve structures, fibers and connective membranes are affected. Scars form. The pathological process is irreversible. Surgery is required.
According to the WHO classification, there are five categories of NAS lesions:
- compression or traumatic injury;
- edema;
- gap;
- final break;
- post-traumatic fibrosis.
Assessing the complexity of a clinical situation
To diagnose neurological pathologies, two research methods are used:
- Mechanoceptive. The tissue response to mechanical action and stimulation is recorded.
- Two-point irritation.
- Brush test.
- Nociceptive. Determine the perception of pain.
- Using a pin.
- Temperature test.
You can determine a taste deficiency by using a cotton pad with sugar or salt.
Research is carried out simultaneously on the affected and healthy sides of the maxillofacial apparatus.
Symptoms are documented. Areas of neurosensory deficit are measured with an accuracy of 1 mm.
Therapy concept
Medical tactics for pain and discomfort:
- Monitoring the patient and tracking the dynamics of the condition over a certain period of time.
- Drug therapy. The use of painkillers, hydrogen pump blockers, glucocorticosteroids and other drugs.
- Removing or unscrewing the rod several turns. It is carried out within 24 hours after implantation. The critical period of treatment is three months. It is during this period that improvement should occur.
- Carrying out a microsurgical operation.
There are no strict treatment protocols. The doctor selects the best option based on practical experience and knowledge.
It is generally accepted that the clinical result of the operation is achieved only if it is performed within a year after implantation.
Surgery
Indications for the operation:
- Confirmed nerve damage.
- Persistent sensory impairment for three months.
- Pain due to a pinched nerve.
The result of surgery depends on certain factors:
- Time elapsed from injury to surgery.
- Type and severity of manifestations.
- Features of blood supply in the pathological zone.
- Proper selection and preparation of the rod.
- The general health of the patient.
- Age.
- Presence of tension zones.
- Experience and practical skills of the surgeon.
Speed of diagnosis is key. Especially with minor damage. Late diagnosis threatens the formation of carpal tunnel syndrome.
Diagnostics
Diagnosis is based on symptoms, medical history, and research:
- The doctor talks with the patient, finds out the symptoms. Finds out what the pain is and where it is located. Are there any infectious diseases in the head area? For example, otitis media, sinusitis, tooth extraction, adenoiditis.
- Then he examines and palpates the damaged area. The presence of swelling and redness is detected.
- When the doctor roughly presents the diagnosis, he examines for the presence of diseases with similar symptoms. That is, differential diagnosis is carried out. Refers for examination to a dentist and otolaryngologist.
- To determine the diagnosis, there is a method of applying a solution of cocaine hydroxide to the mucous membrane of the front of the nose. If the patient stops feeling pain, then this is inflammation of the nasociliary nerve.
- Next, instrumental studies should be carried out. Ophthalmoscopy, MRI of the head, biomicroscopy, anterior rhinoscopy.
- Once the diagnosis is made, treatment is prescribed.
With the help of additional examination, neuralgia of the nasociliary nerve is differentiated from other diseases. And they establish an accurate diagnosis.
Biomicroscopy of the eye
This is done using a slit lamp, the main part of which looks like a large slit. The device examines the structure of the eye, the back and front walls. This method allows you to see any damage, foreign body, and detect the disease at an early stage. Biomicroscopy allows you to see the condition of the retina and optic nerve.
Ophthalmoscopy
The fundus of the eye is examined using an ophthalmoscope. With the help of an eye mirror you can see blood vessels and nerves. Identify changes, redness, swelling.
Anterior rhinoscopy
This is done using a nasal speculum.
The anterior part of the nasal cavity is examined by inserting the device into the nostrils. The most suitable for this procedure is the Hartmann mirror. The doctor holds the device in his left hand, slightly dilating the nostril. In this case, the nasal septum and passages are visible. This is how redness, curvature, atrophy and hypertrophy are noticed. Sometimes it is possible to examine the nasal cavity using reflector lighting. It is used to examine children, as they may be frightened by an unknown object.
MRI of the head
To accurately confirm the diagnosis, an MRI of the head is performed. X-ray radiation is not used here. The examination is carried out using magnetic fields, which create an energy change in the examination area. This is how photographs are taken without the use of contrast. A cross-sectional image is displayed on the computer monitor.
Medical Internet conferences
The trunk of the facial nerve from the beginning of the cervical branch from it to its exit from the stylomastoid foramen in all the adult head-neck complexes we studied lay behind the external carotid artery and the external jugular vein. Of the 9 variants of the facial nerves, we encountered the main type of branching of the nerve in 7 cases, and the scattered type only in 1 person, where both sides of the head and neck area were prepared. With the main type of branching, all facial nerves were quite long and split into 2 trunks: upper and lower, which were subsequently divided into 3 and 2 groups of branches, respectively. During the dissection process in 2 people, where the branches of the facial nerve were isolated on the right and left sides, we found differences in the number of branches, especially from the upper trunk. It branched off in one version: 2 temporal on the left and 3 on the right, 3 zygomatic on the left and 2 on the right, and 2 buccal branches. In another case: also - 2 temporal - on the left and 3 on the right, and there were 2 zygomatic and buccal branches on both sides. In cases of unpaired preparations from 3 different people, among which there were 2 right halves and 1 left half of the head-neck complex, we found: right temporal branches 1 and 2, respectively, zygomatic - 2 and 3, buccal - 2. In the case of the left half: there were 3 temporal branches, 2 zygomatic branches on the left and 1 buccal branch. From the lower trunk, in all cases of main branching, single branches departed - the marginal mandible and the cervical branch. In one case, from the unpaired complex of the left side, the division of the marginal branch into 2, 1 cm before entering the muscle, was noticeable. In the case of loose branching, all 5 branches of the “large crow's foot” were clearly visible. They were short and almost identical in diameter, quickly breaking up into secondary branches. The temporal branch was divided into 3 branches, the zygomatic branch was also divided into 3 branches, the buccal branch was divided into 5 branches, and the marginal mandible and cervical branches were also single, as in the case of the main branching. It should be noted that all angles between the branches did not exceed 14°. With the exception of one option, where the buccal-marginal angle was 20°. The magnitude of the zygomaticotemporal angle ranged from 6 to 9°. The buccal-zygomatic angle ranged from 4 to 7°. The buccal-marginal angle turned out to be the largest – 12–14°. The neck-edge angle was 5–6°. Moreover, of the named values, the smaller value corresponded to the scattered branching of the facial nerve. Among the preparations where measurements were carried out on both sides, the measurement values coincided, which suggests the symmetry of the branching of the facial nerves. Between secondary branches, the angle sizes for all types of branching were 4–5°.
During the preparation process, we discovered 2 anastomoses of the facial nerves with the branches of the trigeminal nerve and the cervical plexus. In one case, we observed an anastomosis between the buccal branch of the facial nerve and the infraorbital nerve, which is a branch of the maxillary nerve (the second branch of the trigeminal nerve). The nerve arising from the pes anserine was an isolated connecting branch, among 5 found in this individual. In another case, the cervical branch of the facial nerve and the transverse nerve of the neck, the cutaneous branch of the cervical plexus, were anastomosed. In this case, the main distribution of nerve fibers to the skin of the neck from the transverse nerve and from it a thin anastomotic branch to the cervical branch of the facial nerve were clearly defined.
Cranial nerve examination
Motor fibers control the muscles of mastication and some muscles of the middle ear.
The trigeminal nerve has three sensory nuclei, two of which are located in the medulla oblongata and pons, and one in the midbrain. The only motor nucleus of this nerve is located in the pons.
The name “trigeminal” is due to the fact that it consists of three branches carrying information from three “floors” of the face - the forehead; nose, cheeks and upper jaw; lower jaw. Motor fibers pass in the inferior branch of the trigeminal nerve.
Facial nerve
(VII pair) contains three types of fibers:
1) afferent sensory fibers bring impulses from the taste buds of the anterior two-thirds of the tongue. These fibers end in the nucleus of the solitary tract, the common sensory nucleus of the facial, glossopharyngeal and vagus nerves. It extends from the medulla oblongata into the pons;
2) somatic motor fibers innervate the facial muscles, as well as the muscles of the eyelids, and some muscles of the ear. These fibers come from the motor nucleus located in the pons;
3) autonomic parasympathetic fibers of the facial nerve innervate the submandibular and sublingual salivary glands, lacrimal glands, and glands of the nasal mucosa. They begin from the parasympathetic superior salivary nucleus, also located in the pons
Glossopharyngeal nerve
(IX pair) is similar in composition to the facial nerve, i.e. also contains three types of fibers:
1) afferent fibers bring information from the receptors of the posterior third of the tongue and end on the neurons of the nucleus of the solitary tract;
2) efferent somatic motor fibers innervate some muscles of the pharynx and larynx. The fibers begin in the nucleus ambiguus, the common motor nucleus for the glossopharyngeal and vagus nerves, located in the medulla oblongata;
3) efferent parasympathetic fibers begin in the inferior salivary nucleus and innervate the near-ear salivary gland.
Nervus vagus
(X pair) is so called because of the extensive distribution of its fibers.
It is the longest of the cranial nerves; with its branches it innervates the respiratory organs, a significant part of the digestive tract, and the heart. The Latin name for this nerve is p. vagus,
which is why it is often called the vagus.
Just like the VII and IX nerves, the vagus contains three types of fibers:
1) afferents carry information from the receptors of the previously mentioned internal organs and vessels of the chest and abdominal cavities, as well as from the dura mater of the brain and the external auditory canal with the auricle. These fibers carry information about the depth of breathing, pressure in blood vessels, stretching of organ walls, etc. They end in the nucleus of the solitary tract;
2) efferent somatic motor innervates the muscles of the pharynx, soft palate, and larynx (including those that control the tension of the vocal cords). The fibers begin in the double core;
Important Functions of the occipital lobe of the brain
3) efferent parasympathetic fibers begin from the parasympathetic nucleus of the vagus nerve in the medulla oblongata. The parasympathetic part of the vagus nerve is very large, so it is predominantly an autonomic nerve.
From sensory cranial nerves
Only the vestibulo-auditory nerve (VIII pair) departs from the brain stem. It brings impulses from the auditory and vestibular receptors of the inner ear to the central nervous system. The sensory nuclei of this nerve - two auditory (ventral and dorsal) and four vestibular (lateral, medial, superior and inferior) - are located on the border of the medulla oblongata and the pons in the area of the vestibular field (see 7.2.2).
The VIII nerve originates in the inner ear and consists of two separate nerves - the cochlear (auditory) nerve and the vestibular (vestibular) nerve.
***
In conclusion, it should be noted that the nuclei of the cranial nerves have many afferents and efferents. Thus, all sensory nuclei send efferents to the thalamus (diencephalon), and from there information enters the cerebral cortex. In addition, sensory nuclei transmit signals to the reticular formation of the brain stem (see 7.2.6). All motor nuclei receive afferents from the cerebral cortex as part of the corticonuclear tract (see 6.4). Finally, there are numerous connections between the cranial nerve nuclei themselves, which facilitates the coordinated activity of various organs. In particular, thanks to the connections between the sensory and motor nuclei, the arcs of the stem unconditioned reflexes (for example, gag, blinking, salivation, etc.), similar to the spinal unconditioned reflexes, are closed.
Date added: 2015-10-01; | Copyright infringement
Related information:
Search on the site:
Innervation of the eyeball
All nerves involved in the functioning of the eye originate in groups of nerve cells localized in the brain and nerve ganglia. The task of the nervous system of the eye is to regulate muscle function, ensure sensitivity of the eyeball, and the auxiliary apparatus of the eye. In addition, it regulates metabolic reactions and blood vessel tone.
The innervation of the eye involves 5 pairs of 12 available cranial nerves: oculomotor, facial, trigeminal, as well as abducens and trochlear.
The oculomotor nerve originates from nerve cells in the brain and has a close connection with the nerve cells of the abducens and trochlear nerves, as well as the auditory and facial nerves. In addition, there is its connection with the spinal cord, providing a coordinated reaction of the eyes, torso and head in response to auditory and visual stimuli or changes in the position of the torso.
The oculomotor nerve enters the orbit through the opening of the superior orbital fissure. Its role is to raise the upper eyelid, ensuring the work of the internal, superior, inferior rectus muscles, as well as the inferior oblique muscle. Also, the oculomotor nerve includes branches that regulate the activity of the ciliary muscle and the work of the pupillary sphincter.
Together with the oculomotor nerve, 2 more nerves enter the orbit through the opening of the superior orbital fissure: the trochlear nerve and the abducens nerve. Their task is to innervate, respectively, the superior oblique and external rectus muscles.
The facial nerve contains motor nerve fibers, as well as branches that regulate the activity of the lacrimal gland. It regulates the facial movements of the facial muscles and the work of the orbicularis oculi muscle.
The function of the trigeminal nerve is mixed; it regulates muscle function, is responsible for sensitivity and includes autonomic nerve fibers. In accordance with its name, the trigeminal nerve splits into three large branches.
The first main branch of the trigeminal nerve is the ophthalmic nerve. Passing into the orbit through the opening of the superior orbital fissure, the optic nerve gives rise to three main nerves: nasociliary, frontal and lacrimal.
The nasolacrimal nerve passes through the muscular funnel, in turn dividing into ethmoidal (anterior and posterior), long ciliary, and nasal branches. It also gives off a connecting branch to the ciliary ganglion.
The ethmoidal nerves are involved in providing sensitivity to cells in the ethmoidal labyrinth, the nasal cavity, and the skin of the tip of the nose and its wings.
The long ciliary nerves lie in the sclera in the area of the optic nerve. Then their path continues in the supravascular space in the direction of the anterior segment of the eye, where they and the short ciliary nerves extending from the ciliary ganglion create a nerve plexus around the circumference of the cornea and the ciliary body. This nerve plexus regulates metabolic processes and provides sensitivity to the anterior segment of the eye. Also, the long ciliary nerves include sympathetic nerve fibers that branch from the nerve plexus belonging to the internal carotid artery. They regulate the activity of the pupillary dilator.
The short ciliary nerves begin in the region of the ciliary ganglion; they run through the sclera, surrounding the optic nerve. Their role is to ensure nervous regulation of the choroid. The ciliary ganglion, also called the ciliary ganglion, is a union of nerve cells that take part in the sensory (via the nasociliary root), motor (via the oculomotor root), and also the autonomic (via sympathetic nerve fibers) direct innervation of the eye. The ciliary ganglion is localized at a distance of 7 mm posterior to the eyeball below the external rectus muscle, in contact with the optic nerve. At the same time, the ciliary nerves jointly regulate the activity of the pupillary sphincter and dilator, providing special sensitivity to the cornea, iris, and ciliary body. They maintain the tone of blood vessels and regulate metabolic processes. The subtrochlear nerve is considered the last branch of the nasociliary nerve; it is involved in the sensitive innervation of the skin of the root of the nose, as well as the inner corner of the eyelids, part of the conjunctiva of the eye.
Entering the orbit, the frontal nerve splits into two branches: the supraorbital nerve and the supratrochlear nerve. These nerves provide sensitivity to the skin of the forehead and the middle zone of the upper eyelid.
The lacrimal nerve, at the entrance to the orbit, splits into two branches - upper and lower. At the same time, the upper branch is responsible for the nervous regulation of the lacrimal gland, as well as the sensitivity of the conjunctiva. At the same time, it provides innervation to the skin of the outer corner of the eye, covering the area of the upper eyelid. The inferior branch unites with the zygomaticotemporal nerve, a branch of the zygomatic nerve, and provides sensation to the skin of the cheekbone.
The second branch becomes the maxillary nerve and is divided into two main lines - the infraorbital and zygomatic. They innervate the auxiliary organs of the eye: the middle of the lower eyelid, the lower half of the lacrimal sac, the upper half of the lacrimal duct, the skin of the forehead and zygomatic region.
The last, third branch, having separated from the trigeminal nerve, does not take part in the innervation of the eye.
Spinal cord, medulla spinalis. Development of the spinal cord.
As already noted, phylogenetically the spinal cord (trunk brain of the lancelet)
appears at stage III of nervous system development (tubular nervous system).
At this time, there is no brain yet, so the trunk brain has centers for controlling all processes of the body, both vegetative and animal (visceral and somatic centers)
. According to the segmental structure of the body, the trunk brain has a segmental structure; it consists of interconnected neuromeres, within which the simplest reflex arc is closed. The metameric structure of the spinal cord is preserved in humans, which determines the presence of short reflex arcs in humans.
With the appearance of the brain (cephalization stage)
Higher control centers for the entire body arise in it, and the spinal cord falls into a subordinate position. The spinal cord does not remain only a segmental apparatus, but also becomes a conductor of impulses from the periphery to the brain and back, and bilateral connections with the brain develop in it. Thus, in the process of evolution of the spinal cord, two apparatuses are formed: the older segmental apparatus of the spinal cord’s own connections and the newer suprasegmental apparatus of the bilateral pathways to the brain. This structural principle is also observed in humans.
Decisive factor in the formation of the trunk brain
is adaptation to the environment through movement. Therefore, the structure of the spinal cord reflects the way the animal moves. So, for example, in reptiles that do not have limbs and move with the help of the body (for example, a snake), the spinal cord is developed evenly along its entire length and has no thickenings. In animals that use limbs, two thickenings occur, and if the forelimbs are more developed (for example, the wings of birds), then the anterior (cervical) thickening of the spinal cord predominates; if the hind limbs are more developed (for example, the legs of an ostrich), then the posterior (lumbar) thickening is increased; if both forelimbs and hindlimbs (four-legged mammals) are involved in walking, then both thickenings are equally developed. In humans, due to the more complex activity of the hand as a labor organ, the cervical thickening of the spinal cord was differentiated more strongly than the lumbar one.
The noted phylogenetic factors play a role in the development of the spinal cord and ontogenesis
.
The spinal cord develops from the neural tube,
from its posterior segment (the brain arises from the anterior segment). From the ventral section of the tube, the anterior columns of the gray matter of the spinal cord (cell bodies of motor neurons), adjacent bundles of nerve fibers and processes of these neurons (motor roots) are formed. From the dorsal section arise the posterior columns of gray matter (cell bodies of interneurons), posterior funiculi (processes of sensory neurons).
Thus, the ventral part of the brain tube is primarily motor
, and the dorsal one is
primarily sensitive
.
The division into motor (motor)
and
sensory (sensitive)
areas extends throughout the neural tube and is maintained in the brain stem.
Due to the reduction of the caudal part of the spinal cord, a thin cord of nervous tissue is obtained, the future filum terminale.
Initially, in the 3rd month of uterine life, the spinal cord occupies the entire spinal canal, then the spine begins to grow faster than the brain, as a result of which the end of the latter gradually moves upward (cranially). At birth, the end of the spinal cord is already at the level of the third lumbar vertebra, and in an adult it reaches the height of the first - second lumbar vertebra. Thanks to this “ascent” of the spinal cord, the nerve roots extending from it take an oblique direction.
Optic neuritis - symptoms and treatment
neuritis is an inflammation of the optic nerve. With the disease, vision sharply decreases, its field narrows and color perception is impaired. Spots and flickering appear before the eyes, pain occurs in the orbital area, which intensifies with eye movements [2].
Among all eye diseases, lesions of the optic nerve occur in 3.2% of cases [6].
The optic nerve is an atypical cranial nerve that contains approximately 1 million nerve fibers. It is the white matter of the brain located in the periphery. Its length is 35–55 mm [1]. Through it, visual information perceived by retinal cells is transmitted to the brain.
Nerve cell processes gather from throughout the retina to form the optic disc. Then they go to the brain, cross with the nerve fibers of the second eye and form the optic chiasm. The visual tract begins from it, which ends in the primary subcortical visual centers.
The optic nerve is divided into several parts:
- intraocular part and head of the optic nerve;
- retrobulbar part (behind the eye), or orbital;
- intratubular;
- intracranial.
The length of the intraocular part of the optic nerve is 25–35 mm. In the horizontal plane, the nerve bends in an S-shape, so that it is not stretched when the eyeball moves.
The intraocular part includes the optic disc. The optical fibers of the retina are connected in it, and vessels emerge from the center: narrow light red arteries and darker thick veins.
The retrobulbar or orbital part is a section of the optic nerve 25–35 mm long. It starts from the area where the nerve exits the eyeball and continues until it enters the optic canal.
The intracanalicular part of the optic nerve is enclosed in the optic canal. Its length is about 6 mm, the nerve here is fixed to the wall of the canal.
The intracranial part of the optic nerve passes into the optic chiasm. The length of this section is on average 10 mm. The intracranial region is particularly vulnerable to pathologies of adjacent structures, such as pituitary adenoma or aneurysm. With such disorders, the optic chiasm can be compressed, causing the visual field to narrow and the optic nerve to atrophy. If the optic nerve vessel is damaged, the patient ceases to see in one eye [2]. Hemianopsia, which is blindness in both eyes in half the visual field, also occurs.
With neuritis, the trunk and sheaths of the optic nerve in its various parts become inflamed. If the process extends to the optic nerve head, then such inflammation is called intraocular neuritis or papillitis . When the process occurs behind the eye, it is retrobulbar optic neuritis [3].
Causes of optic neuritis
It is not always possible to find out the exact cause of the disease, but most often inflammation of the optic nerve is caused by:
- multiple sclerosis is the most common cause of optic neuritis;
- other autoimmune diseases such as Sjogren's syndrome, systemic lupus erythematosus;
- Neuromyelitis optica is a demyelinating disease that primarily affects the eyes and spinal cord;
- demyelinating diseases associated with serum immunoglobulin G to myelin-oligodendrocyte glycoprotein (MOG-IgG) - for example, acute disseminated encephalomyelitis;
- granulomatous diseases - sarcoidosis, granulomatosis with polyangiitis[13];
- inflammatory diseases of the brain - encephalitis, arachnoiditis, meningitis, brain abscess, etc.;
- acute and chronic general infections - tuberculosis, Lyme disease, syphilis, brucellosis, typhus, erysipelas, influenza, smallpox, etc.;
- inflammatory diseases of the eyes and orbit;
- intoxication with lead or methyl alcohol; in children, helminthic intoxication is possible;
- penetrating wounds of the eye and orbit;
- traumatic brain injuries.
Neurology of motor nerves
If cranial nerves are affected, neurological manifestations depend on their functional purpose. The group of motor ones emanating from the parasympathetic nuclei of the trunk includes:
- oculomotor (III);
- block (IV);
- abducent (VI);
- additional (XI);
- sublingual (XII).
Oculomotor pair
from the orbit it controls the oblique muscle, which ensures the elevation of the eyelid. The oculomotor provides neurons to the muscle that controls the pupil and eyelash movements. If it is affected, weakness and even paralysis of the above muscles appear. Then the eye opens only partially or does not open at all, accommodation is disrupted, the light reaction of the pupil disappears, and strabismus may develop.
Block
from the skull it runs into the eye socket and controls the rotation of the eyeball with the help of the oblique muscle. Its defeat is accompanied by deviations of the apple of the affected eye and double vision. The fibers of the trigeminal nerve branch into processes and perform many functions. They control and provide sensitivity to various parts of the face.
Neuronal bundle diverting
directs contractions on one side of the lateral muscle, and on the opposite side, the medial muscle. The symptoms that appear depend on the degree of damage to the nuclei or neurons. Various visual disturbances may occur: strabismus, double vision, hemiplegia. The greater length of the nerve increases the risk of damage.
Additional
consists of 2 (spinal and vagus) parts. Through a conductive (two-neuron pathway) it carries out motor functions. When the nerve is irritated, tonic muscle spasms develop in the sternoclavicular area (nodding movements of the head, its unnatural rotation). A one-sided lesion leads to difficulties in moving the head and shoulders; a bilateral lesion leads to the inability to make these movements, often the head tilts back.
Hyoid nucleus
located in the rhomboid fossa, its motor filaments innervate the lingual muscles. Damage to the 12th nerve leads to their paresis and decreased tongue mobility. Bilateral damage is fraught with the development of paralysis of the innervated organ (glossoplegia).
Important Soothing aromatherapy
Vagus nerve (X pair, 10 pair of cranial nerves), n. vagus
N. vagus, vagus nerve
, which developed from the 4th and subsequent gill arches, is so called due to the vastness of its distribution.
It is the longest of the cranial nerves. With its branches, the vagus nerve supplies the respiratory organs, a significant part of the digestive tract (up to the colon sigmoideum)
, and also gives branches to the heart, which receives fibers from it that slow down the heartbeat.
N. vagus
contains three types of fibers:
1. Afferent (sensory) fibers
, coming from the receptors of the named viscera and vessels, as well as from some part of the dura mater of the brain and the external auditory canal with the auricle to the
sensitive nucleus (nucleus solitarius)
.
2. Efferent (motor) fibers
for the voluntary muscles of the pharynx, soft palate and larynx and the efferent (proprioceptive) fibers emanating from the receptors of these muscles.
These muscles receive fibers from the motor nucleus (nucleus ambiguus)
.
3. Efferent (parasympathetic) fibers
emanating from
the vegetative nucleus (nucleus dorsalis n. vagi)
.
They go to the myocardium of the heart (slow down the heartbeat) and the muscular lining of the blood vessels (dilate the blood vessels). In addition, the cardiac branches of the vagus nerve include the so-called n. depressor, which serves as a sensory nerve for the heart itself and the initial part of the aorta and is in charge of the reflex regulation of blood pressure. Parasympathetic fibers also innervate the trachea and lungs (narrow the bronchi), esophagus, stomach and intestines to the colon sigmoideum
(increase peristalsis), embedded in the named organs of the gland and glands of the abdominal cavity - liver, pancreas (secretory fibers), kidneys.
Parasympathetic part of the vagus nerve
is very large, as a result of which it is primarily an autonomic nerve, important for the vital functions of the body. The vagus nerve is a complex system consisting not only of nerve conductors of heterogeneous origin, but also containing intra-trunk nerve nodes.
Fibers of all types associated with the three main nuclei of the vagus nerve
, leave the medulla oblongata in its sulcus lateralis posterior, below the lingual tray nerve, with 10-15 roots, which form a thick nerve trunk, leaving the cranial cavity together with the lingual tray and accessory nerves through the foramen jugulare.
In the jugular foramen, the sensitive part of the nerve forms a small node - ganglion superius
, and at the exit from the foramen - another fusiform ganglion thickening -
ganglion inferius
.
Both nodes contain pseudounipolar cells, the peripheral processes of which are part of the sensory branches going to the named nodes or receptors of the viscera and blood vessels ( ganglion inferius
) and the external auditory canal (
ganglion superius
), and the central ones are grouped into a single bundle, which ends in
the sensitive nucleus, nucleus solitarius.
Upon exiting the cranial cavity, the trunk of the vagus nerve
goes down to the neck behind the vessels in the groove, first between v.
jugularis interna and a. carotis interna, and below - between the same vein and a. carotis communis, and it lies in the same vagina with the named vessels. Next, the vagus nerve penetrates through the upper thoracic aperture into the chest cavity, where its right trunk is located in front of a. subclavia, and the left one is on the anterior side of the aortic arch. Going down, both vagus nerves go around the root of the lung from behind on both sides and accompany the esophagus, forming plexuses on its walls, with the left nerve passing along the front side, and the right one along the back. Together with the esophagus, both vagus nerves penetrate through the hiatus esophageus of the diaphragm into the abdominal cavity, where they form plexuses on the walls of the stomach. The trunks of the vagus nerves
in the uterine period are located symmetrically on the sides of the esophagus.
After the stomach turns from left to right, the left vagus moves forward, and the right one moves back, as a result of which the left vagus
, and the right one on the posterior surface.
Optic nerve, nervus ophthalmicus
First branch of the trigeminal nerve. Provides sensitive innervation to the eyeball, lacrimal gland, lacrimal sac, mucous membrane of the ethmoidal labyrinth, frontal and sphenoid sinuses, skin and conjunctiva of the upper eyelid, glabella, dorsum of the nose, and forehead. Consequently, its innervation zone is located above the palpebral fissure.
Sensory nerve. Starts from the Gasserian node, enters the cavernous sinus, sinus cavernosus
.
When leaving the cavernous sinus, it gives off the nerve of the tentorium of the cerebellum, n.
tentorii , after which through the superior orbital fissure,
fissura orbitalis superior
, it goes into the orbit and here it divides into 3 nerves:
1. Nasociliary nerve, n. nasociliaris.
2. Frontal nerve, n. frontalis.
3. Lacrimal nerve, n. lacrimalis.
1. Nasociliary nerve, n. nasociliaris
, runs along the medial wall of the orbit to the medial corner of the eye along the way, giving off 5 branches:
– long root of the ciliary node, radix longus g. ciliare
- goes to the eyelash node;
– long ciliary nerves, nn. cliares longi —
innervate the membranes of the eyeball;
– posterior ethmoidal nerve, n. ethmoidalis posterior
,
–
through the opening of the same name it enters the nasal cavity and innervates the mucous membrane of the nasal cavity and sphenoid sinus;
– anterior ethmoidal nerve, n. ethmoidalis anterior
, - through the hole of the same name it enters the cranial cavity, and then through the perforated plate,
lamina cribrosa
, penetrates the nasal cavity, sends a branch to the frontal sinus and innervates the anterior sections of the lateral wall and septum of the nasal cavity, up to the tip of the nose;
– subtrochlear nerve, n. infratrochlearis
, is the terminal branch of the nasociliary nerve. It goes to the medial corner of the eye, where it anastomoses with the supratrochlear nerve.
2. Frontal nerve, n.frontalis
, runs along the upper wall of the orbit and is divided into three nerves:
– supratrochlear nerve, n. supratrochlearis
, – anastomoses with the subtrochlear and together they innervate the skin and conjunctiva of the medial corner of the eye, the lacrimal sac, the skin of the dorsum of the nose, and forehead;
– supraorbital nerve, n. supraorbitalis, –
innervates the skin of the forehead and scalp;
– frontal branch, gamus frontalis –
goes to the glabella and innervates the skin of this area.
3. Lacrimal nerve, n.1acrimalis
, runs along the lateral wall of the orbit, where an anastomosis from the zygomatic nerve approaches it,
ramus communicans cum nervo zygomatico
.
This anastomosis consists of autonomic fibers coming from the pterygopalatine ganglion. The nerve becomes mixed (contains sensory, sympathetic and parasympathetic fibers). Lacrimal branches extend from the lacrimal nerve, rr.
1acrimalae , in which all the autonomic fibers and some of the sensory fibers go to innervate the lacrimal gland, and the lacrimal nerve itself, in which only sensory fibers remain, innervates the skin and conjunctiva of the lateral corner of the eye.
Along the first branch of the trigeminal nerve in the orbit there is a ciliary ganglion ciliare
.
Ciliary node, ganaglion ciliare
The parasympathetic autonomic ganglion is located in the orbit lateral to the optic nerve. Three types of fibers are suitable for it:
1. Short spine, gadix brevis
, parasympathetic fibers that come from the Yakubovich nucleus as part of the oculomotor nerve.
2. Long spine, adix longus
, - sensory fibers coming from the nasociliary nerve.
3. Sympathetic root, radix sympathicus
, - sympathetic fibers coming from the cavernous plexus,
plexus cavernosus
.
Since the node is parasympathetic and contains only parasympathetic cells, the parasympathetic fibers are interrupted in it (i.e., the transmission of a nerve impulse occurs through synaptic connections to the nerve cells of the node), and the sensitive and sympathetic fibers pass through in transit. Three types of fibers depart from the node in the form of 3-6 short ciliary nerves, nn ciliares breves
:
– parasympathetic – innervate the constrictor pupillary muscle, m. sphincter pupillae
;
– sympathetic – muscle that dilates the pupil, m. dilatator pupillae
;
– sensitive – innervate the nucleus of the eyeball.
Maxillary nerve, nervus maxillaris
The second branch of the trigeminal nerve innervates the gums and teeth of the upper jaw, skin of the nose, lower eyelid, upper lip, cheek and temporal region, mucous membrane of the palate, upper lip, nasal cavity, maxillary sinus, cheek. Consequently, it innervates the midface between the palpebral fissure and the angle of the mouth.
The nerve is sensitive and begins in the Gasserian ganglion. Exits from the skull through the round opening, foramen rotundum
.
Before leaving the skull, the middle branch of the meninges departs from it, ramus meningeus medius
, which innervates the dura mater of the middle cranial fossa.
Coming out of the skull, the nerve enters the pterygopalatine fossa, fossa pterygopalatina
, where it divides into three branches:
1. Zygomatic nerve, n. zygomaticus.
2. Infraorbital nerve, n. infraorbitalis.
3. Nodal nerves, rr. ganglionares.
1. Zygomatic nerve, n. zygomaticus
, from the pterygopalatine fossa through the lower orbital fissure,
fissura orbitalis inferior
, enters the orbit, runs along its lateral wall, where it gives off a connecting branch to the lacrimal nerve ramus
communicans cum nervo lacrimali
.
Then, through the zygomaticoorbital foramen, foramen zygomaticoorbitale
, it enters the zygomatic bone, where it divides into two branches:
– zygomaticofacial, r. zygomaticofacialis
, which exits the zygomatic bone through the hole of the same name and innervates the skin of the lateral surface of the face;
– zygomaticotemporal, r. zygomaticotemporalis
, which exits through the opening of the same name and innervates the skin of the temporal region.
2. Infraorbital nerve, n. infraorbitalis
, through the lower orbital fissure enters the cavity of the orbit, runs along its lower wall, enters the infraorbital groove and canal, and through the infraorbital foramen,
foramen infraorbitalis
, enters the face, where it divides into its terminal branches.
Even in the pterygopalatine fossa, the posterior superior alveolar branches, rr, depart from it.
alveolares superiores posteriores , which enter the upper jaw through the openings of the same name and in the area of the alveolar process participate in the formation of the upper dental plexus,
plexus dentalis superior
, from which the dental branches innervate the large molars.
In the region of the infraorbital groove and canal, the upper middle and anterior alveolar branches, rr, respectively, depart.
alveolares superiores medius et anteriores , which also form the upper dental plexus,
plexus dentalis superior
, giving off dental branches,
rr.
dentales superiores respectively to the small molars, incisors and canines and the upper gingival branches,
rr.
gingivales superius .
The plexuses located in the alveolar process of the upper jaw exchange fibers, which explains the irradiation of pain in dental diseases. When entering the face through the infraorbital foramen in the canine fossa, the nerve forms a “lesser crow’s foot”, pes anserinus minor
, consisting of branches that innervate:
– skin of the lower eyelid , rami palpebrales inferiores;
– skin of the lateral surface of the nose, rami nasales externi
;
– skin and mucous membrane of the upper lip and gums, rami labiales superiores
;
– mucous membrane of the anterior parts of the nasal cavity, rr. nasales inferiores
.
3. Nodal nerves, rr. ganglionares
, in the pterygopalatine fossa they come from the maxillary nerve,
n.
maxillaris , to the pterygopalatine ganglion,
ganglion pterygopalatinum
.
Pterygopalatine ganglion
This is a parasympathetic (periorgan, third-order) node located in the fatty tissue of the pterygopalatine fossa. Three types of fibers are suitable for it:
1. sensitive root, radix sensoria
, – nodal branches,
rr.
ganglionares , from the maxillary nerve.
2. parasympathetic root, radix parasympatica
, - great petrosal nerve,
petrosus major
, which runs from the intermediate nerve (VII pair) along the anterior surface of the pyramid of the temporal bone to the lacerated foramen,
foramen lacerum.
3. sympathetic root, radix sympatica
, – deep petrosal nerve,
n.
petrosus profundus , which starts from the internal carotid plexus,
plexus caroticus internus
, formed by the neurons of the superior cervical ganglion of the sympathetic trunk.
Sympathetic and parasympathetic roots i.e. The large and deep petrosal nerves in the area of the foramen lacerum unite to form the pterygoid or Vidian nerve, nervus pterygoideus
, which through the canal of the same name enters the pterygopalatine fossa and approaches the pterygopalatine node. Since the node is parasympathetic, only parasympathetic fibers are interrupted in it, while sensitive and sympathetic fibers pass through in transit.
Departing from the node:
– medial and lateral superior posterior nasal branches, rr. nasales posteriores superiores mediales et laterales
, penetrating through the sphenopalatine foramen to the mucous membrane of the posterior sections of the upper and middle nasal passages;
– inferior posterior nasal branches, rr. nasales posteriores inferiores
, heading through the greater palatine canal to the mucous membrane of the bottom of the nasal cavity;
– nasopalatine nerve, n. nasopalaninus
, (Scarpian nerve), passing first through the sphenopalatine foramen to the mucous membrane of the nasal septum, and then through the incisive canal,
canalis incisivus
, to the mucous membrane of the hard and soft palate;
– greater and lesser palatine nerves, n. palatinus major et nn. palatini minores
;
from the pterygopalatine fossa through the greater and lesser palatine canals, canalis palatinus major et minor
, penetrate into the oral cavity, where they innervate the mucous membrane of the hard and soft palate;
– zygomatic branches, rr. zygomatici
. From the node, autonomic fibers go to the maxillary nerve, then go to the zygomatic nerve, then in the form of a connecting branch they approach the lacrimal nerve, from which they depart to innervate the lacrimal gland.
Mandibular nerve, nervus mandibularis
The third branch of the trigeminal nerve innervates the gums and teeth of the lower jaw, the mucous membrane of the tongue, cheek and lower lip, the skin of the chin, the submandibular and sublingual salivary glands, the temporomandibular joint, the muscles of mastication, some muscles of the neck, palate and middle ear. Consequently, the sensory fibers of this nerve innervate the lower part of the face (below the corner of the mouth).
It is a mixed nerve that contains both sensory and motor fibers. Sensitive ones begin from the Gasserian ganglion, and motor ones - from the motor nucleus, nucleus motorius
.
It leaves the skull through the oval opening, foramen ovale
, and enters the infratemporal fossa,
fossa infratemporalis
.
Immediately after leaving the skull, the spinous nerve, n.
spinosus , which through
the foramen spinosum
returns to the cranial cavity and innervates the dura mater of the middle cranial fossa. In the infratemporal fossa, the nerve divides into two branches:
1. Anterior, ramus anterior
, mainly motor, to the masticatory muscles
2. Posterior, ramus posterior
, mostly sensitive.
From the anterior branch come:
1.1. Nerve of the same name to the masticatory muscle, nervus massetericus
.
1.2. Deep temporal nerves, nn. temporales profundi
, to the temporal muscle.
1.3. Lateral pterygoid nerve, n. pterygoideus lateralis
, to the muscle of the same name.
These three nerves are motor, and the fourth:
1.4. Buccal nerve, nervus buccalis
– sensitive, innervating the skin of the cheek and buccal mucosa.
From the posterior branch depart:
2.1. Medial pterygoid nerve, nervus pterygoideus medialis
, motor, to the muscle of the same name, branches extend from it to the muscle that strains the velum palatine and to the muscle that strains the tympanic membrane,
m.
tensor veli palatini et m. tensor tympani .
2.2. Lingual nerve, nervus lingualis
, sensitive, passes between the pterygoid muscles, then goes down and forward and runs along the inner surface of the lower jaw, enters the tongue and ends there.
The chorda tympani
, approaches it .
plexus caroticus externus
approach the lingual nerve (its continuation is the facial plexus,
plexus facialis
). Thus, the nerve becomes mixed and contains 4 types of fibers: general sensitivity, taste sensitivity, parasympathetic and sympathetic fibers.
From the lingual nerve depart:
– hypoglossal nerve, n. sublingualis
, contains three types of fibers, except for flavor.
It goes first to the sublingual ganglion, ganglion sublinguale
. After the node, all three types of fibers are directed to the sublingual salivary gland.
– submandibular branches, nn. submandibulare
, contain three types of fibers, in addition to taste.
They are directed first to the node of the same name, ganglion submandibulare
, and then to the submandibular salivary gland.
– lingual branches, rr. linguales
, contain all 4 types of fibers. Fibers of general sensitivity innervate the anterior two-thirds of the tongue, fibers of taste sensitivity innervate all papillae of the tongue except the valvate, and autonomic fibers innervate the small salivary glands of the tongue.
– branches of the isthmus of the pharynx, rr. isthmi faucimi
, to the mucous membrane of the palatoglossal arch and to the palatine tonsil.
Submandibular, g. submandibulare, and sublingual, g. sublingvale, nodes
Located next to the glands of the same name, parasympathetic in structure, containing peripheral parasympathetic neurons, the axons of which (postganglionic fibers) end in the salivary glands of the tongue, submandibular and sublingual glands. Preganglionic parasympathetic fibers arise from the superior salivary nucleus of the facial nerve. They pass in stages as part of the drum string, chorda tympani
, lingual and hypoglossal nerves of the mandibular branch of the V pair and are interrupted by the neurons of the nodes.
Generally sensitive fibers are called nodal branches, rami ganglionares
.
Passing through the nodes in transit, they provide general sensitivity to these glands. Sympathetic fibers enter the nodes from the plexus of the facial artery, pl.
sympathicus a. facialis , pass through the nodes in transit and bring trophic innervation.
2.3. Inferior alveolar nerve, n. alveolaris inferior
, this is a mixed nerve, contains sensory and motor fibers.
It runs along the inner surface of the lower jaw and in the area of the foramen mandibularis
is divided into sensitive and motor parts.
Sensory fibers enter and exit the mandibular canal through the foramen mentale
.
In the canal, the lower alveolar branches depart from the nerve, rr.
alveolares inferiores , which enter the alveolar process of the lower jaw, form a plexus,
plexus dentalis inferior
, from which the lower dental branches,
rr.
dentales inferiores , innervate all lower teeth, and the lower gingival branches,
rr.
gingivales inferiores , gum of the lower jaw.
The final branch of the sensitive part, n.
mentalis , innervates the skin of the chin and the mucous membrane of the lower lip.
Motor fibers form the maxillohyoid nerve, n. mylohyoideus
, which runs along the inner surface of the lower jaw in the groove of the same name and innervates the muscle of the same name,
m.
mylohyoideus , and the anterior belly of the digastric muscle,
m.
digastricus .
2.4. Auriculotemporal nerve, n. auriculotemporalis
, sensitive, goes in front of the external auditory canal up to the temporal region.
ganglion oticum,
approach it .
Functions of cranial nerves
There are 3 types of structures considered. Some are responsible for muscle contraction; these are the motor (activator) functions of the cranial nerves. Others transmit impulses and “knowledge” received from the senses to the cortex for analysis. There are also mixed cranial nerves that perform both tasks in parallel. Functionality is determined by the type of neuronal fiber transmission.
Motor cranial nerves
There are 4 pairs in this group, each performing separate tasks. Motor nerves:
- Trochlear (IV)
– associated with the upper muscle, facial (oblique). Provides the eyeball with the ability to rotate to the sides and rotate. - Abductor (VI)
– connected to the rectus lateralis muscle. Necessary for retracting the eyeball to the desired direction. - Accessory (XI)
- innervates the sternocleidomastoid muscle. Thanks to it, the neck bends, the head turns, tilts to the sides, leans back, and the shoulders move. - Hypoglossal (XII)
– the 12th pair of cranial nerves is connected to the oral cavity. The structure is primarily responsible for comfortable swallowing and precise movements of the tongue muscle.
Important Brain pons
Sensory cranial nerves
An alternative name is sensory pairs, due to their connections with the sensory organs. Sensory cranial nerves perform the following functions:
- Olfactory (I)
– the shortest fibers in length. Necessary for the perception of smells. - Visual (II)
– transports impulse data from the photoreceptors of the retina to the cortex. These cranial nerves are responsible for visualization. - Vestibulocochlear (VIII)
– vestibular functions. This pair is necessary to maintain a sense of balance and transmit auditory signals.
Mixed cranial nerves
The described group of neuron fibers is responsible for both motor activity and the sensitivity of certain structures. Cranial mixed nerves:
- Oculomotor (III)
– transmits signals to the middle section. The pair is responsible for the sensitivity of the pupils to changes in light (constriction and dilation). At the same time, nerves provide movement of the eyeballs. - Trigeminal (V)
is the largest neural formation. This pair transmits sensory information from facial tissues and mucous membranes. Additionally, the structures regulate the movements of the masticatory muscles. - Facial (VII)
– the main task is to “command” facial expressions, control the functioning of the salivary and lacrimal glands. In parallel, the nerves transmit information about taste from the tongue receptors to the brain. - Glossopharyngeal (IX)
– associated with structures of the same name. In the oral cavity, these human cranial nerves collect sensory information about taste. The pair also provides swallowing by transmitting commands to the cervical muscles and the salivary gland. - The vagus (X)
is the most “loaded” nerve. “Serves” the heart, respiratory tract, digestive and filtering organs. It affects the swallowing process, regulates the overall activity of a person, and adjusts the intensity of stress. The pair can interact with the sympathetic system and most internal organs.
Branches of the maxillary nerve
2. Branches of the maxillary nerve (n. maxillaris) (Fig. 524). The middle meningeal branch (r. meningeus medius) starts from the receptors of the dura mater of the middle cranial fossa and joins the maxillary nerve near the round foramen of the sphenoid bone.
524. Scheme of the second branch of the trigeminal nerve. 1 - pes anserinus minor; 2 - rr. labiales superiores; 3 - rr. nasales externi; 4 - rr. palpebrales inferiores: 5 - for. infraorbitales; 6 - n. infraorbitalis iv. 7 - n. zygomaticofacialis: 8 - for zygomaticofaciale; 9 - n. zygomaticotemporal; 10 - for. zygomaticotemporale; 11 - for zygomaticoorbitale; 12 - n. lacrimalis; 13 - r. communicans cum n. lacrimalis; 14 - fissura orbitalis inferior; 15 - n. zygomaticus; 16 - nn. pterygopalatine 17 - for. rotundum; 18 - r. meningeus medius; 19 - gangl. pterygopalatinum; 20 - nn. palatini; 21 - nn. nasales posteriores; 22 - rr. orbitales; 23 - rr. alveolares superiores posteriores; 24 - rr. alveolares superior medius et anteriores; 25 - pl. dentalis superior; 26 - rr. den tales superiores.
The orbital branches (rr. orbitales) have receptors in the mucous membrane of the posterior cells of the ethmoid bone and the sphenoid sinus. Their fibers penetrate through the openings in the sutura sphenoethmoidalis into the posterior part of the orbit, through the inferior orbital fissure into the pterygopalatine ganglion and further into the pterygopalatine nerves (nn. pterygopalatine, which enter the maxillary nerve within the pterygopalatine fossa. The orbital branches include parasympathetic fibers from the pterygopalatine ganglion and sympathetic fibers from n. petrosus profundus, passing through the pterygopalatine ganglion.
The posterior superior nasal branches (rr. nasales posteriores superiores) contain sensory receptors in the mucous membrane of the nasal cavity and are formed from 8-15 branches in the form of three nerves: 1) nasopalatine nerve (n. nasopalatxnus), the sensory fibers of which begin from receptors located in mucous membrane of the hard palate of the oral cavity. Its branches are through for. incisivum pass into the nasal cavity, being in the submucosal layer of the nasal septum, accompanying a. nasalis posterior septi; 2) in the nasal cavity, the medial branches of the posterior superior nasal nerve (rr. nasales posteriores superiores mediates), innervating the mucous membrane of the nasal septum in the upper nasal passage, join the nasopalatine nerve; 3) the lateral branches of the posterior superior nasal nerve (rr. nasales posteriores superiores laterales) contact receptors in the mucous membrane of the upper and middle nasal passages, the posterior cells of the ethmoid bone, the vault of the pharynx, the auditory tube, the choanae and the sinus of the sphenoid bone. Sensory fibers of these three nerves through for. sphenopalatinum penetrate the pterygopalatine fossa, pass by the pterygopalatine node and through the nn. pterygopalatini reach the maxillary nerve. In the pterygopalatine fossa, from its node, parasympathetic postganglionic and sympathetic fibers from n penetrate into the posterior superior nasal branches. petrosus profundus for the innervation of mucous glands located in the zone of sensitive innervation (Fig.
525).
525. Scheme of the structure of the pterygopalatine node. Red lines are parasympathetic fibers; blue - sensitive; blue (intermittent) - sympathetic. 1 - gangl trigeminale; 2—n. petrosus major; 3 - petrosus profundus; 4 - gangl. pterygopalatinum; 5 - nn. palatini minores; 6 - rr. nasales; 7 - nn. pterygopalatini; 8 - n. zygomaticus.
The palatine nerves (nn. palatini) are formed from three nerves: 1) the greater palatine nerve (n. palatinus major) starts from the receptors of the mucous membrane of the hard and soft palate. The axons of sensory cells form 3-4 trunks, which through the for., palatinum majus penetrate the canalis palatinus major, and then into the pterygopalatine fossa and then enter the maxillary nerve; 2) small palatine nerves (nn. palatini minores) contact the receptors of the mucous membrane of the soft palate, palatine tonsil. They contain motor fibers from n. facialis, penetrating into m. levator veli palatini as part of n. petrosus major. The fibers of the lesser palatine nerve enter through the lesser palatine foramina into the canalis palatinus minor and reach the maxillary nerve; 3) the lower posterior lateral nasal branches (rr. nasales posteriores inferiores laterales) contain sensory fibers starting from receptors in the mucous membrane of the walls of the lower and middle nasal passages, the maxillary sinus. Through small openings between the palatine bone and the pterygoid processes they penetrate the canalis palatinus major, reach the pterygopalatine fossa and through the nn. pterygopalatini reach the maxillary nerve; 4) pterygopalatine nerves (nn. pterygopalatini) are sensory fibers of the orbital branches, posterior superior nasal branches and palatine nerves, connecting above the pterygopalatine ganglion into the pterygopalatine nerves entering the maxillary nerve.
All branches of the palatine nerves contain parasympathetic fibers emerging from the pterygopalatine ganglion, and sympathetic fibers from n. petrosus profundus, which reach the mucous glands of the oral and nasal cavities. Thus, nn. palatini are mixed.
The zygomatic nerve (n. zygomaticus) is formed from two nerves: 1) the zygomaticofacial branch (r. zygomaticofacialis) contacts the skin receptors of the upper part of the cheek and the lateral canthus. Its fibers penetrate through for. zygomaticofaciale into the thickness of the zygomatic bone, where they connect with n. zygomaticotemporalis, which penetrates through for. zygomaticoorbitale into the orbit; 2) the zygomaticotemporal branch (r. zygomaticotemporalis) starts from receptors located in the skin of the temporal and frontal regions. The nerve enters through for. zygomaticotemporale into the thickness of the zygomatic bone, uniting with the zygomaticofacial nerve into the zygomatic nerve. The zygomatic nerve passes into the orbit through the for. zygomaticoorbitale, located outside the eyeball. The zygomatic nerve leaves the orbit through the inferior orbital fissure and, within the pterygopalatine fossa, enters the maxillary nerve. As part of the zygomatic nerve, and then the zygomaticotemporal branch, parasympathetic fibers pass from the pterygopalatine nerve. In the orbit they leave the zygomaticotemporal branch and go to n. lacrimalis, which reaches the lacrimal gland. This transition of parasympathetic fibers from one nerve to another is called the connective branch.
The branches of the infraorbital nerve (n. infraorbitalis) are divided into two groups: the first has receptors in the soft tissues of the upper jaw, the second - in the teeth and gums of the upper jaw.
Branches of the first group: a) upper labial branches (rr. labiales superiores) have their receptors in the skin and mucous membrane of the upper lip. The nerve fibers are united into 3 - 5 branches located under the quadratus muscle of the upper lip in the fossa canina. These branches reach for. infraorbitale and are part of the infraorbital nerve; b) internal nasal branches (rr. nasales interni) begin from receptors located in the mucous membrane of the vestibule of the nose. The branches emerge through the openings between the nasal cartilage and the nasal bone and connect with the external nasal branches; c) external nasal branches (rr. nasales externi) contact the skin receptors of the wings of the nose; d) the lower branches of the eyelids (rr. palpebrales inferiores) begin from the receptors located in the skin of the lower eyelid. The nerve descends, passing through the beginning of the quadratus superior labii muscle, and enters the infraorbital nerve.
Branches of the second group: a) anterior superior alveolar branches (rr. alveolares superiores anteriores) begin from receptors located in the pulp of the upper incisors and canines, gums, periodontium and the mucous membrane of the anterior nasal cavity. Then their fibers enter the alveolar process of the upper jaw, participating in the formation of the upper dental plexus (plexus dentalis superior). From the dental plexus, 1-2 branches of the anterior superior alveolar branches are formed, which pass along the canalis alveolaris in the upper jaw. Via for. alveolaria anteriora they exit into the orbit, where they unite with the infraorbital nerve in the inferoorbital canal; b) the middle upper alveolar branch (r. alveolaris superior medius) has receptors in the pulp of the upper small molars, gums, periodontal and periodontal tissues, then the fibers participate in the formation of the upper dental plexus (plexus dentalis superior). From this plexus, 1-2 branches emerge along the alveolar canal in the thickness of the body of the upper jaw and enter the terminal part of the infraorbital nerve in the region of the pterygopalatine fossa; c) the posterior superior alveolar branches (rr. alveolares superiores posteriores) contact the receptors of the mucous membrane of the maxillary sinus, the pulp of large molars, gums, periodontal and periodontal tissues. The nerve fibers of the receptors participate in the formation of the superior dental plexus, located at the apexes of the roots in the alveolar process. The posterior superior alveolar nerve is formed from the plexus, which reaches the posterior alveolar openings of the tubercle of the upper jaw through the canalis alveolaris. Having entered the infratemporal fossa, with up to 8 branches, the nerve enters the pterygopalatine fossa and unites with the infraorbital nerve.
Thus, from the fusion of many branches, the infraorbital nerve is formed, initially located in the sulcus infraorbitalis, in the space from the infraorbital foramen to the pterygopalatine fossa. In this fossa it participates in the formation of the maxillary nerve.
The maxillary nerve is formed by connecting the pterygopalatine, zygomatic, infraorbital nerves and the meningeal branch within the pterygopalatine fossa. The nerve has a diameter of 2.5-4 mm, a length of 12-15 mm and passes through the round foramen of the sphenoid bone into the cranial cavity, where it enters the ganglion. trigeminale.
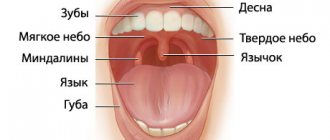
Taste nerves
Ellipsoidal-shaped cells located in the mouth are designed to detect taste (taste bud). Taste buds consist of basal cells and chemoreceptors (the taste receptors themselves). Taste buds of different types are located on the tongue, cheeks, soft palate, epiglottis in the initial part of the esophagus.
Sensations of sweet, salty, bitter are transmitted to a certain part of the GM cortex through the nerves: glossopharyngeal (IX), facial (YII), vagus (YIII). Taste bioimpulses travel through nerve fibers to the thalamus, then to the guardian region of the GM cortex.
Damage to these nerves and the central parts of the brain (tumors, injuries, operations) provokes neural taste disorders:
- total ageusia, loss of the ability to distinguish taste (salty, sweet, etc.);
- ageusia partial;
- specific ageusia;
- dysgeusia (perverted taste).
Treatment of the disease
Treatment of nasociliary nerve neurosis consists of eliminating the disease that affects it.
In case of inflammatory processes in the ENT organs, patients are prescribed a course of treatment with antibiotics and a set of drugs that affect the elimination of inflammation and restoration of the mucous membrane, or surgical intervention (for pathologies of the nasal septum).
For vascular diseases, patients are prescribed drugs with antihypertensive and nootropic effects. Treatment is also carried out using vasoactive drugs.
To relieve pain and other symptomatic and clinical manifestations of neuralgia, local anesthetic drugs are used in medical practice in combination with non-narcotic painkillers and vasodilators. Their use is determined by which part of the nasociliary nerve has undergone pathological effects:
- For neuralgia of the long ciliary nerve, dicaine (0.25% eye solution) mixed with adrenaline (4 drops per 10 ml of solution) is used.
- For neuralgia of the subtrochlear region of the nasociliary nerve, cocaine hydrochloride (2% solution) mixed with 0.1% adrenaline (4 drops per 5 ml of the drug) is used. A solution of lidocaine is also used in the form of a spray, which is injected into the nasal passages on the corresponding side or both at once (for bilateral neuralgia) up to 4 times a day.
- If any part of the nerve is damaged, use a powder mixture of papaverine, glucose, antispasmodic, diphenhydramine and aminazine 2 times a day.
As an additional therapy for patients diagnosed with Charlin's syndrome, a course of intramuscular vitamin B12 is indicated, as well as intravenous administration of sulfonamide drugs.
Unpleasant chest pain is often a sign of heart disease. But a similar symptom is also characteristic of neuralgia. A competent specialist should be able to distinguish the signs of neuralgia in the heart area from heart pain. Read the article about how to treat this disease.
We will consider the causes and symptoms of trigeminal neuralgia in this topic.
Anesthesia of the inferior alveolar nerve at the mandibular foramen
To perform anesthesia correctly, you need to know where the inferior socket opening is located. By the way, the location of the lower hole in adults and children, as well as citizens of retirement age, varies somewhat. In the former, it covers the inner part of the ramus of the lower jaw, comparable to the chewing region of the lower molars, and in the latter, it is slightly lower. The accessibility of the inferior alveolar nerve for drug anesthesia with solutions is due to its placement in front of the entrance to the bone canal, located in the bone groove. The area of the bone groove consists of loose fiber, which allows the injected anesthetic solution to be evenly distributed.
Anesthesia is carried out using two methods that differ from each other in the type of access to the anesthetized area - extraoral and intraoral. The anesthesia affects not only the area of the lower jaw where interventions are performed, but also its alveolar part, as well as the gums, mucous membrane and skin of the lower lip, the sublingual area, the skin of the sublingual part and most of the tongue.
The essence of the intraoral approach is as follows: first, a palpation determination of the injection site is carried out, located slightly further than the molar fossa and the temporal crest. The injection is given with the mouth wide open. In this case, the needle is located inside the temporal crest 0.7-1.0 cm higher than the chewing surface of the molars in order to cover their outer and posterior parts up to contact with the bone. The inferior alveolar nerve is blocked by moving the needle inward a couple of centimeters to the bony groove and injecting the rest of the anesthetic into it.
Anesthesia using the apodactyl method involves selecting the pterygomaxillary fold as a landmark, which is inward from the temporal crest. The injection is also carried out with the mouth wide open and the position of the needle identical to the one described above, which is inserted into the area of the outer slope of the pterygomaxillary fold approximately in the middle of the distance between the chewing surface of the upper and lower molars. Then it is advanced 1.5-2 cm deep, reaching the bone. An anesthetic is administered to block the inferior alveolar and lingual nerves.
Both methods of intraoral access to anesthesia have an analgesic effect after 3-5 minutes, maintaining the effect for up to an hour and a half.
Among the intraoral methods of anesthesia, there are two main ones - the Gow-Gates method and the Vazirani-Akinosi method. The most effective is the Gou-Gates method, in which it is possible to block the inferior alveolar nerve, and with it the lingual, auriculotemporal, mylohyoid, and buccal nerves. The sequence of manipulations with this method is as follows: a section of the lateral edge of the pterygomaxillary recess is selected as the injection site, and the injection itself is made with the mouth wide open into the mucous membrane under the medial palatal tubercle in the area of the second molar of the upper jaw. The trajectory of the needle movement is to the tragus of the ear or the neck of the condylar process to the bone stop at a depth of 2.5 cm. The patient’s mouth does not close for another 2-3 minutes. You can begin operational actions in 8-10 minutes.
The immobilized lower jaw prompts the specialist to use the Vazirani-Akinosi method, which is activated when the teeth are closed.
The anesthetic effect in both cases occurs within 5-10 minutes, but the Vazirani-Akinosi method requires special care to avoid deepening the needle into the mucous membrane along the medial surface of the mandibular ramus. The consequences of such an oversight can be disastrous - damage to the branches of the facial nerve must not be allowed.
Diagnosis of neuralgia
A neurologist is involved in differential diagnosis. Diagnosis of neuralgia begins with a neurological examination of a patient with typical complaints for this disease. The listed causes of neuralgia require a more complete examination to identify or exclude the underlying disease.
In some cases, additional instrumental examination (electroneurography) may be required if the cause of neuralgia was injury in the projection of the nerve. An MRI of the spine or any of the nerve plexuses may be required in the event of any volumetric impact on the nerve structures, as occurs with a herniated or protruded intervertebral disc or soft tissue tumors.