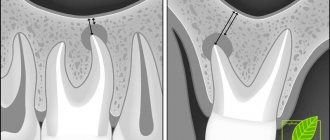
The maxillary (maxillary) sinus, despite its significant volume (up to 10 cubic centimeters), in a healthy person is hidden in the thickness of the bone of the upper jaw and does not betray its presence in any way. However, it is not so far from the mouth - the roots of an adult’s teeth sometimes reach it. In some cases, perforation of the bottom of the maxillary sinus is possible, meaning its direct connection with the oral cavity. This is possible due to some physiological characteristics of a particular patient:
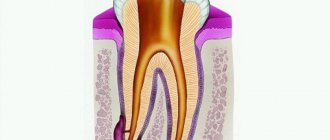
- the close arrangement of the roots of the teeth can thin the bone border between the oral cavity and the maxillary sinus, from normal 1 centimeter to a very dangerous 1 millimeter;
- with low bone thickness, the roots of the molars can reach the cavity, separated from it only by the mucous membrane;
- a cyst, periodontitis or periodontitis can contribute to the thinning of the bony septum between the sinus and the oral cavity.
Perforation occurs against the background of the listed factors after dental intervention, even if the surgical technique was not violated.
What causes perforation?
The most common causes of perforation are:
- removal or implantation of teeth;
- root resection;
- endodontic treatment.
When the tooth roots are located directly in the maxillary sinus, the doctor’s skill level or his accuracy do not affect the situation in any way - perforation simply cannot be avoided. But it must be recognized that with low professionalism of a specialist, a problem can appear even in cases where its occurrence could have been prevented.
Endodontic treatment leads to perforation in cases where the insertion of a pin or compaction of filling cement was carried out too aggressively, as well as in pathological expansion of the root canals. In such a situation, perforation occurs directly through the thickness of the tooth, and foreign objects in the form of fragments of dental roots and cement can get inside the maxillary sinus.
When implanting teeth, filling root canals and installing pins, the occurrence of a fistula is always considered a consequence of a medical error.
Installation of an artificial root requires maximum attention from the doctor, since it threatens to perforate the maxillary sinus. The patient’s bone tissue after the removal of a “native” tooth has a tendency to rapid degeneration - the body does not see the point in maintaining tissue that is not assigned any functions. If you delay the installation of the implant, choose its size incorrectly, or perform the operation without proper preparation, perforation will be a predictable result.
In the case of tooth root resection, there are no alternative treatment options - a cyst in the upper part of the root can only be removed this way. However, the doctor must first obtain a clear idea of the thickness of the alveolar process (the bony septum between the maxillary sinus and the oral cavity), and how far the root is from the maxillary sinus.
Consequences of perforation
Perforation of the maxillary sinus is a fairly serious pathology that often has to be treated in a hospital. Attempts to independently treat it with folk remedies at home without medical assistance can lead to the development of serious and dangerous consequences:
- The development of a pronounced inflammatory reaction in the sinus cavity with the spread of infection to the surrounding bone tissue and the formation of foci of osteomyelitis of the upper jaw.
- Spread of inflammation to other sinuses of the skull (frontal, sphenoid and ethmoid).
- Loss of healthy teeth located in the area of untreated perforation.
- Formation of purulent foci (abscesses, phlegmons).
Due to the close location of the maxillary sinus and the brain, after perforation, infection may spread to the meninges with the development of meningitis or meningoencephalitis, which threatens the patient’s life.
Symptoms
When a tooth is removed, sinus perforation can be diagnosed by characteristic and clearly visible signs:
- there are air bubbles in the blood released at the site of the extracted tooth, their number increases with targeted, accentuated exhalation through the nose;
- blood will also come from the nose - on the side where the tooth was removed and perforation occurred; it can be mixed into nasal secretions in small quantities, only slightly tinting them a light pink shade;
- The patient's voice changes, a previously uncharacteristic nasal tone appears in it.
A visitor to a dental office can sometimes feel that air is passing through the hole where the extracted tooth was located. This phenomenon is accompanied by unusual feelings of pressure or heaviness in the maxillary sinus.
Endodontic procedures and implantation, accompanied by perforation of the maxillary sinus, are distinguished by their own characteristics:
- the installed element or equipment seems to fall inward after applying additional force;
- there is a sharp change in the position of the tool in the hole made;
- the blood protruding from the hole is saturated with oxygen bubbles.
It is important to understand in time that there is a problem and promptly address it. If this is not done, an infection will get into the maxillary sinus. Symptoms will become more than obvious to the patient:
- the sinus area delivers extremely unpleasant sensations in the form of acute pain;
- the nasal mucosa on the corresponding side swells, breathing through the nostrils becomes difficult;
- Possible discharge of pus from the nose.
In addition to the specific symptoms, there are also general signs typical of intoxication: the temperature rises, weakness is felt, the patient has a headache, and the patient is shivering.
Treatment
To eliminate the resulting disease, surgical treatment is indicated. Surgery can be avoided if the complication arose in the dentist's chair after tooth extraction and was immediately diagnosed. In this case, the treatment tactics consist of carefully preserving the formed blood clot and preventing infection of the tooth socket for 5-7 days. At the same time, the doctor prescribes the patient a course of preventive measures to prevent inflammatory reactions. This usually involves taking anti-inflammatory and antibacterial drugs and vasoconstrictor drops. Outpatient or at home - depends on the patient’s condition.
Diagnosis
At the time of a dental operation that led to perforation of the maxillary sinus, the doctor draws a conclusion about a new problem based on the signs described above. If perforation is questionable, the dentist's findings are rechecked using the following methods:
- probing with a thin probe;
- radiography - shows dark accumulations of blood, tooth root fragments and filling cement located inside the maxillary sinus, can be done with the preliminary administration of a contrast agent;
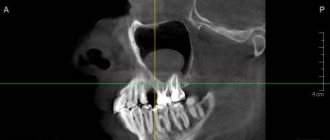
- CT scan;
- general clinical blood test - necessary when identifying an old problem to make sure there is an infection in the body.
Diagnostics
Diagnosis of perforation of the floor of the maxillary sinus during tooth extraction is based on a typical clinical picture. In doubtful cases, as well as when such a complication is suspected during implantation or endodontic manipulations, it is necessary to use instrumental diagnostic methods:
- Probing the socket of an extracted tooth or perforated canal with a thin probe . This allows us to determine that there is no bone bottom in the wound. In this case, the instrument passes freely through soft tissues and does not encounter obstacles along its path.
- X-ray of the sinus area . In this case, the pictures can reveal both darkening of the cavity due to the accumulation of blood in it, as well as fragments of dental roots, implants or filling material. Sometimes it is advisable to conduct radiography with contrast, when a contrast agent is introduced into the cavity through a perforation fistula.
- Computed tomography , which allows you to determine perforations and the presence of foreign bodies in the sinus with maximum accuracy.
- If old perforations are suspected, general clinical blood tests , the result of which may indicate the presence of an active source of infection in the body.
How to treat?
The tactics for eliminating the problem depend on exactly what causes led to the perforation and what the general clinical picture is. Almost always, repairing a perforation requires surgery, the only exception to this rule is when a hole was created during a tooth extraction, provided that the dentist found it immediately and no foreign objects or infection got inside. If the problem is identified immediately, it is important to keep the blood clot in the place where it formed and prevent it from becoming infected - it will become a natural barrier to the infection entering the sinus. Protecting a blood clot from infection is carried out using a tampon with an iodine solution, which will have to be kept for at least a week.
In some cases, the doctor chooses the tactic of suturing the gum tissue. Another alternative is to install a compact plastic plate that is attached to adjacent teeth and acts as a barrier between the oral cavity and the sinus until the septum is restored.
For obvious reasons, physical barriers cannot provide a 100% guarantee that infection will not penetrate the hole, so the doctor additionally prescribes vasoconstrictors and anti-inflammatory drugs. They can be taken at home, but sometimes require the patient’s outpatient presence.
Penetration of any foreign objects into the maxillary sinus is regarded as a serious complication, which automatically means the need for surgical intervention and hospital treatment. In such a situation, the sinus is opened, removing foreign objects and tissues that cannot be restored, after which the fistula is covered with the patient’s tissues.
Perforation of the maxillary sinus: treatment
Conservative treatment for perforation of the maxillary sinus is indicated only in cases of its rapid detection. If it happens during the process of tooth extraction, the surgeon and the patient need to make every effort to keep the blood clot in the socket. To do this, apply an antiseptic turunda or alveolar bandage and secure it with sutures. The hole can be covered with fibrinogen-based glue, film or protective sheets. The patient is prescribed antibacterial therapy and vasoconstrictor drops are prescribed for instillation into the nose. It is important that for seven days he minimizes coughing, sneezing and blowing his nose - in this case, a hole with a diameter of up to five millimeters will close on its own.
Surgical closure of maxillary sinus perforation is recommended for holes of five millimeters or more that exist for more than twenty days. If foreign objects have entered the cavity, an operation is performed to remove them (sinusrotomy) in combination with plastic surgery of the perforation of the maxillary sinus using:
- Native tissue in the form of a buccal, alveolar, vestibular or combined flap, which is sutured to the wound edges;
- Synthetic materials in the form of plates of collagen, dura mater, bone matrix;
- Autografts in the form of fragments of the patient’s native bone, taken from the rib/chin/jaw and secured with steel screws.
You can make an appointment with CELT dental surgeons to eliminate perforation online on our website or by contacting our information line operators: +7 (495) 788-33-88.
Make an appointment through the application or by calling +7 +7 We work every day:
- Monday—Friday: 8.00—20.00
- Saturday: 8.00–18.00
- Sunday is a day off
The nearest metro and MCC stations to the clinic:
- Highway of Enthusiasts or Perovo
- Partisan
- Enthusiast Highway
Driving directions
Perforation discovered after the fact
If the patient suffered discomfort in the first 2-4 weeks and did not contact the dentist, who, in turn, did not identify the problem at the time of its occurrence, the perforated wound turns into a permanent fistula that is not prone to healing.
Typical signs of chronic sinusitis appear:
- the nose on the side of the fistula is constantly stuffy;
- the parasinus area gives off a dull pain, its waves can roll to the nearest eye and temple;
- pus is discharged from the nostrils and in the mouth (from the fistula);
- possible swelling of the cheek on the side of the fistula with visible deformation of the face.
In most cases, a fistula is felt as air passing between the nose and mouth while talking or sneezing. Pronunciation of a number of sounds becomes more difficult. Liquid food may enter the nose from the mouth. Therapy for an old fistula shows rather weak results, and relapse with such a problem is not uncommon. There is no alternative to surgical intervention - it is necessary to open the maxillary sinus, remove foreign objects and non-viable tissue. The fistula requires excision throughout its entire thickness, the defect is closed with healthy tissues of the patient. After the operation, an antibiotic course lasting one and a half to two weeks is prescribed; in parallel, antihistamines and anti-inflammatory drugs must be used.
How is surgery to remove a cyst in the nose performed?
For a long time, surgery to remove a sinus cyst was carried out only by opening the wall of the maxillary sinus through the oral cavity or through the cheek. This manipulation is called maxillary sinusotomy; it is quite traumatic and requires a long recovery period.
Currently, classical surgery is rarely performed, with preference given to minimally invasive interventions. But for extensive purulent cases, just such a radical intervention is used. The dangerous formation is completely removed, the sinus is washed with an antiseptic and drained.
In other cases, surgery on the maxillary cyst is performed endoscopically, with minimal disruption of the integrity of the sinus walls.
If necessary, additional plastic surgery of the anastomosis is performed and adjacent polypous growths are removed.
Endoscopic surgery to remove a maxillary sinus cyst is performed on an outpatient basis and usually lasts 20–40 minutes. After its completion, the patient remains in the clinic for 1–2 hours under the supervision of a doctor, then returns to his normal life.
Using an endoscope allows you to remove the maxillary cyst in a gentle way. This operation does not disrupt the drainage and ventilation of the sinuses, reduces the risk of chronic rhinosinusitis and does not require long-term recovery for the patient.
Why shouldn’t you treat perforation of the maxillary sinus yourself?
To date, there are no effective treatments for perforation other than surgery. An attempt to cure yourself at home using “traditional medicine” means that time will be lost and the situation will become neglected. You can start the problem before complications arise:
- the sinus cavity becomes inflamed, the infection spreads to the bone tissue, the patient begins to suffer from osteomyelitis of the upper jaw;
- inflammation penetrates into other intracranial sinuses, and there are more foci of infection;
- next to the untreated perforation, the alveolar process is weakened, as a result of which healthy teeth may fall out;
- foci of suppuration develop.
The maxillary sinus is also located in close proximity to the brain. The lack of a timely response and the development of suppuration inside the sinus is fraught with meningitis and meningoencephalitis - these are diagnoses that directly threaten life.
GBOU "NIKIO im. L.I. Sverzhevsky" of the Moscow Department of Health
Oroantral fistula
The maxillary sinus is the largest of all the paranasal sinuses and is shaped like a four-sided pyramid. The lower wall of the maxillary sinus is formed by the alveolar process along the length from the first premolar to the tubercle of the upper jaw. An anatomical feature of the lower wall of the sinus is that in some cases the bone bridge between the apexes of the roots of the teeth adjacent to it and the lumen of the sinus itself can be up to 1 mm thick, and in some cases its role is played by the mucous membrane of the sinus. In our opinion, it would be advisable to distinguish between two concepts - “oroantral communication” and “oroantral fistula”. The oroantral communication is formed immediately after the violation of the seal of the maxillary sinus and in some cases, with the correct treatment tactics, does not lead to the development of traumatic sinusitis and oroantral fistula. We can talk about the presence of an oroantral fistula when the bone walls of the alveolus of the extracted tooth are epithelialized, but the seal of the sinus is not restored.
The diagnosis of chronic odontogenic maxillary sinusitis is established on the basis of clinical and radiological data. X-ray and CT examinations are the most important diagnostic methods for identifying various forms of chronic sinusitis.
The treatment tactics for chronic odontogenic maxillary sinusitis is determined by the clinical form of the disease. During exacerbation of chronic sinusitis, its exudative forms (catarrhal, serous, purulent) are treated, as a rule, conservatively. In this case, the same means and treatment methods are used that are used in the treatment of acute sinusitis. Productive forms of chronic odontogenic maxillary sinusitis (polypous, polypous-purulent) are treated surgically. Regardless of the form of chronic sinusitis in the presence of visual and intracranial complications, the main method should be surgical treatment.
The main goal of surgical treatment for chronic odontogenic maxillary sinusitis is to remove the affected teeth and create conditions for restoring the normal function of the affected maxillary sinus. To do this, regardless of the surgical approach, the damaged sinus anastomosis with the nasal cavity is created anew or restored, ensuring its free drainage and ventilation. Thus, we are talking about restoring the impaired function of the osteo-meat complex.
Treatment
There are a significant number of different options and modifications of surgical interventions on the maxillary sinuses, proposed for the treatment of sinusitis. All of them, depending on the approach, are divided into extranasal and endonasal. It should be noted that most surgeons in the surgical treatment of odontogenic maxillary sinusitis, especially in the presence of persistent oroantral communication, operate using the traditional technique of radical maxillotomy and communication plastics. Today, the technique of extra- or intranasal sinusotomy with plastic surgery of the bottom of the maxillary sinus with a trapezoidal mucoperiosteal flap cut from the vestibular surface of the alveolar process of the upper jaw is used. In some cases, sinusotomy was accompanied by the removal of a foreign body from the lumen of the sinus (most often a tooth root) or filling material.
Currently, surgical treatment of chronic odontogenic maxillary sinusitis with persistent oroantral communication in specialized clinics is carried out using a gentle endoscopic maxillotomy technique with simultaneous plastic surgery of the oroantral communication.
Endonasal operations of the paranasal sinuses were developed almost simultaneously with extranasal ones. However, only with the advent of modern endoscopes with fiber optics and long-focus operating microscopes, endonasal operations began to be introduced into clinical practice.
We fulfill
Extra- and intranasal maxillotomy with simultaneous plastic surgery of the oroantral fistula, if present.
Prevention
Perforation of the maxillary sinus is a problem that is easier to avoid than to fix it later. Since perforation is caused by dental intervention, preventing the problem falls on the shoulders of the dentist. He is obliged:
- responsibly examine the patient before performing procedures;
- clearly understand the anatomical features of the client before major intervention;
- strictly adhere to the intervention technology.
The dentist is also obliged to respond adequately to any signs of perforation that has just occurred due to his fault. If for some reason the doctor has not fulfilled his own duties, then it is up to the patient - he must refuse self-medication and put aside the fear of dentists, in no case try to “endure” the discomfort, but immediately seek help.
Why does a cyst appear in the nose?
The main reasons for the appearance of maxillary cysts include:
- Recurrent or chronic maxillary sinusitis (sinusitis). Inflammatory changes in the mucous membrane lead to blockage or scarring of the excretory glandular ducts. The produced secretion has no outflow, accumulates and stretches the gland. This is how true mucous and serous cysts are formed.
- Chronic non-infectious inflammation (usually of an allergic nature), accompanied by hyperplasia of the mucous membrane of the nose and paranasal sinuses.
- Dental pathology, the resulting cysts are called odontogenic. The most common reason for their appearance is inflammation around the root of a carious tooth or near the tooth germ of the upper jaw. The purulent process leads to atrophy and destruction of bone tissue, spreading to the walls of the maxillary sinus. More rare causes include abnormally deep tooth roots and excessively traumatic tooth extraction.
- Predisposing factors are injuries to the facial part of the skull, congenital anomalies with asymmetry of the hard palate and nasal bones, and immunodeficiency states. Occasionally, a cyst in the sinus is formed against the background of a congenital defect in mucus production, when the secretion of the glands has an excessively viscous consistency.
Removal of a maxillary sinus cyst at the ENT clinic of Dr. Korenchenko
See also Treatment of ENT diseases Cyst in the maxillary sinus Treatment of a cyst in the maxillary sinus Surgery to remove a cyst in the maxillary sinus
Endoscopic ENT surgeries are not performed in all clinics. After all, they require modern equipment, the doctor having the appropriate skills and certificates. Dr. Korenchenko’s ENT clinic is a modern, specialized and well-equipped medical center. Our specialists are highly qualified and have rich clinical experience, all the necessary certificates and skills. When treating patients, we use only modern, clinically proven and highly effective techniques.
Endoscopy at Dr. Korenchenko’s Clinic is an important and widely used therapeutic and diagnostic procedure. It is included in the basic examination of all patients who apply and are observed, which allows doctors to receive reliable and accurate information about the current condition of the ENT organs. Our specialists also perform removal of maxillary cysts and most other operations endoscopically, with high results and without long-term rehabilitation of patients.
Treatment at Dr. Korenchenko’s ENT clinic is a modern and competent approach, using effective technologies and effective therapeutic regimens.