The maxillary (maxillary) sinus, despite its significant volume (up to 10 cubic centimeters), in a healthy person is hidden in the thickness of the bone of the upper jaw and does not betray its presence in any way. However, it is not so far from the mouth - the roots of an adult’s teeth sometimes reach it. In some cases, perforation of the bottom of the maxillary sinus is possible, meaning its direct connection with the oral cavity. This is possible due to some physiological characteristics of a particular patient:
- the close arrangement of the roots of the teeth can thin the bone border between the oral cavity and the maxillary sinus, from normal 1 centimeter to a very dangerous 1 millimeter;
- with low bone thickness, the roots of the molars can reach the cavity, separated from it only by the mucous membrane;
- a cyst, periodontitis or periodontitis can contribute to the thinning of the bony septum between the sinus and the oral cavity.
Perforation occurs against the background of the listed factors after dental intervention, even if the surgical technique was not violated.
Features of the maxillary sinus
The maxillary sinus (its other name is the maxillary sinus) is located in the thickness of the bone tissue of the upper jaw. It is separated from the oral cavity by the alveolar process of the upper jaw, which forms its bottom. The volume of such a sinus is quite large, and in adults it can reach 10 cubic centimeters.
This sinus, or sinus, is not airtight. It communicates with the nasal cavity through a narrow slit.
Typically, perforation of the maxillary sinus occurs in the area of its bottom. Some of its features contribute to this:
- Close proximity of the roots of molars and premolars. In some cases, the thickness of the bone layer between the tooth roots and the bottom of the maxillary sinus can be relatively large - up to 1 cm, but in some people the bone border between these formations is very thin - no more than 1 mm.
- Sometimes the roots of the first and second molars are located in the sinus cavity itself, separated from it by just a layer of mucous membrane.
- Rapid thinning of the bone layer in the presence of acute or chronic inflammatory diseases: periodontitis, periodontitis, cysts.
- Relatively thin bony trabeculae in the tissue of the upper jaw.
All this predisposes to the occurrence of perforation during dental procedures, even if the treatment technique was not violated and the doctor did not apply significant traumatic force.
Therapeutic measures
In most cases, perforation cannot be treated without surgery. Such an operation can be avoided only if the pathology arose as a result of tooth extraction procedures and was immediately detected by a specialist.
At the same time, all necessary measures to prevent the defect were also taken in a timely manner. In such situations, most often the septum is sutured or a turunda is placed in the hole, which is pre-moistened with a special composition that has anti-inflammatory properties.
This helps prevent the entry and spread of infection. Also, when carrying out such procedures, the hole heals more quickly.
For several weeks, the patient is regularly observed by a specialist, who examines him every other day and changes the turunda.
However, not in all cases the wound is sutured immediately. Sometimes it is enough that there is no foreign body in the wound. After this, the attending physician makes sure that it does not start to bleed. To prevent recurrent bleeding, the wound is packed for seven days and sutures are placed on the gums.
If the damage to the wall of the maxillary sinus occurred long ago, then it is impossible to avoid surgical intervention. During the procedure, the maxillary sinus is opened and all dead tissue and foreign bodies are removed.
After such treatment, the doctor prescribes a course of antibiotics, which lasts for two weeks. In this case, it is also necessary to use anti-inflammatory and antihistamine medications.
Causes of perforations of the maxillary sinus floor
The etiology of perforations of the maxillary sinus is always associated with any dental procedures. Perforation can occur:
- when removing teeth;
- during endodontic treatment;
- during dental implantation;
- during root resection.
When teeth are removed, damage to the bottom of the maxillary sinus can be a consequence of either rough actions by the dentist or failure to comply with treatment tactics, or as a result of the anatomical characteristics of the patient himself (for example, when the tooth roots are located directly in the sinus cavity).
When endodontic treatment is carried out, one of the complications is perforation of the tooth root, which is often combined with damage and perforation of the bottom of the maxillary sinus. This happens when the root canals are excessively expanded, when brute force is used when inserting pin elements or compacting filling cement. With this type of perforation of the maxillary sinus, filling material or root fragments almost always penetrate into its cavity.
If perforation occurs at the time of insertion of a dental implant (it can be an implant of any brand, for example, Mis, Nobel, Xive, etc.) or during root canal filling or insertion of pins into the tooth root, then it is always a therapeutic error doctor's tactics.
Damage to the bottom of the maxillary sinus is a serious complication when implanting artificial roots into bone tissue during prosthetics. This is explained by the fact that after tooth extraction, bone tissue very quickly undergoes degeneration processes. As a result, the height of the alveolar process of the jaw decreases. If the doctor does not take this point into account and incorrectly carries out preparations before implantation, and also incorrectly selects the size of the implant, then the risk of sinus perforation is very high.
Tooth root resection is a treatment method for the presence of cysts in the area of its apex. If the patient is underexamined, when the doctor does not know the exact size of the bone plate separating the bottom of the sinus from the wall of the cyst, and also if it is necessary to remove a large volume of jaw bone, then perforation of the maxillary sinus is not a rare phenomenon.
What medical errors lead to perforation?
The presence of the problems described above does not guarantee that the tooth will independently enter the maxillary sinus. This usually occurs when there is a perforation - a break in the thin wall between the mouth and the nasal sinus. In the vast majority of cases, this occurs during dental procedures. And if monitoring the condition of teeth and preventing osteoporosis is the responsibility of the patient, then mechanical perforation is always the responsibility of the doctor. Of course, it is much more difficult for the latter to work if at least one of the factors described above is present. That is why good health (including teeth) is the result of cooperation between the doctor and the patient.
Patients often complain that the pain from sinusitis radiates to the teeth. A detailed examination reveals a radically opposite picture. Perforation of the bottom of the maxillary sinus is detected, which causes pain. The fact is that periodontitis may not make itself felt for a long time, but sinusitis debuts quickly. Therefore, it seems that the problem is in the nose, and not in the mouth.
Perforation in most cases appears as a result of a medical error made during the treatment or extraction of teeth.
Perforation of the maxillary sinus during tooth extraction
Removing a tooth if its root is located in the maxillary sinus or is separated from it by a thin layer of bone is always difficult. Especially when it comes to 2-3 molars with massive and intertwined roots. Since the dental surgeon applies physical force during the operation, there is a high probability of damaging the already thin layer of bone.
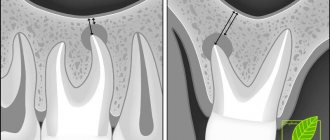
In this case, it is recommended to take a photo at the end of the procedure. Treatment of perforation of the maxillary sinus immediately after tooth extraction is simple. The doctor will be able to quickly restore the tightness of the sinus, avoiding complications. To exclude the possibility of a fistula forming in the nasal sinus after some more time, it is recommended to take a repeat photo after a month.
Perforation during implantation
A perforation of a sinus near a tooth during prosthetics is always a very serious complication that can cast doubt on the success of the entire operation. To prevent this, additional bone augmentation using various methods is performed before implantation.
Before implanting the implant, the doctor must take a panoramic photo. If the roots of a wisdom tooth or other molars and premolars are located in the maxillary sinus or in close proximity to it, then a sinus lift is prescribed, during which the bottom of the sinus is raised and strengthened.
If perforation does occur, then implantation is postponed until complete healing.
Perforation during endodontic treatment
Acute sinusitis can also develop after routine dental treatment. During canal treatment, it is easy to go beyond the apex with a metal instrument or filling material. To eliminate the possibility of complications and promptly eliminate perforation after each stage of endodontic treatment, it is important to take an image. Modern radiovisiographs have a very low radiation dose, so they cannot harm health in any way.
Perforation during removal of the apex or root of a tooth completely
From the point of view of perforation, tooth-saving operations can also pose a danger, for example, removing the root of a tooth with a cyst on it that has grown into the maxillary sinus. Such operations are relatively safe for teeth 4-5, while for teeth 6-7 they are no longer advisable. The risk of perforation is too great. It is worth clarifying that we are talking about cases with a pathologically thin bone septum between the nasal sinus and the oral cavity. If the bone thickness is within normal limits, then apectomy is performed for any tooth.
Symptoms of perforation
If perforation of the nasal sinus occurred at the time of tooth extraction, then its symptoms will be quite specific:
- The appearance of small air bubbles in the blood released from the tooth socket, the number of which increases with a sharp forced exhalation through the nose.
- The appearance of bloody discharge from the nose on the side of the perforated maxillary sinus.
- Changes in the timbre of the patient’s voice, the appearance of “nasality”.
Sometimes the patient begins to complain about the passage of air through the hole after tooth extraction, as well as a feeling of heaviness or pressure in the projection of the maxillary sinus.
If perforation of the maxillary sinus occurs during implantation or endodontic treatment, the doctor may suspect it by:
- characteristic failure of the instrument or implanted element after applying some force to advance it;
- changing the position of the instrument in the wound;
- the appearance of small air bubbles in the blood.
If perforation of the maxillary sinus for any reason was not diagnosed and treated immediately, then its cavity becomes infected with the development of acute sinusitis or sinusitis, which is characterized by symptoms such as:
- severe acute pain in the maxillary sinus area;
- swelling of the nasal mucosa on the corresponding side with difficulty breathing through the nose;
- the appearance of purulent nasal discharge.
The appearance of general symptoms of intoxication is also characteristic: headaches, chills, high fever, weakness.
Prevention
Perforation of the maxillary sinus is a problem that is easier to avoid than to fix it later. Since perforation is caused by dental intervention, preventing the problem falls on the shoulders of the dentist. He is obliged:
- responsibly examine the patient before performing procedures;
- clearly understand the anatomical features of the client before major intervention;
- strictly adhere to the intervention technology.
The dentist is also obliged to respond adequately to any signs of perforation that has just occurred due to his fault. If for some reason the doctor has not fulfilled his own duties, then it is up to the patient - he must refuse self-medication and put aside the fear of dentists, in no case try to “endure” the discomfort, but immediately seek help.
Diagnostics
Diagnosis of perforation of the floor of the maxillary sinus during tooth extraction is based on a typical clinical picture. In doubtful cases, as well as when such a complication is suspected during implantation or endodontic manipulations, it is necessary to use instrumental diagnostic methods:
- Probing the socket of an extracted tooth or perforated canal with a thin probe . This allows us to determine that there is no bone bottom in the wound. In this case, the instrument passes freely through soft tissues and does not encounter obstacles along its path.
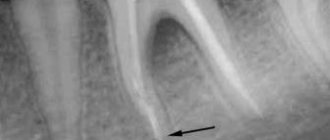
- X-ray of the sinus area . In this case, the pictures can reveal both darkening of the cavity due to the accumulation of blood in it, as well as fragments of dental roots, implants or filling material. Sometimes it is advisable to conduct radiography with contrast, when a contrast agent is introduced into the cavity through a perforation fistula.
- Computed tomography , which allows you to determine perforations and the presence of foreign bodies in the sinus with maximum accuracy.
- If old perforations are suspected, general clinical blood tests , the result of which may indicate the presence of an active source of infection in the body.
Diagnosis
At the time of a dental operation that led to perforation of the maxillary sinus, the doctor draws a conclusion about a new problem based on the signs described above. If perforation is questionable, the dentist's findings are rechecked using the following methods:
- probing with a thin probe;
- radiography - shows dark accumulations of blood, tooth root fragments and filling cement located inside the maxillary sinus, can be done with the preliminary administration of a contrast agent;
- CT scan;
- general clinical blood test - necessary when identifying an old problem to make sure there is an infection in the body.
Treatment
Treatment of perforations of the maxillary sinus floor depends on what changes are present in the sinus cavity itself.
Treatment without surgery is possible only in cases where perforation occurred during tooth extraction and was detected immediately, and according to radiography there are no signs of infection of the sinus cavity or the presence of even minor foreign bodies in it. With this option, the doctor’s tactics are to preserve the blood clot formed in the socket as carefully as possible, as well as to prevent its infection. To do this, a small gauze swab soaked in iodine solution is inserted into the lower part of the hole. Usually it is tightly fixed in the wound cavity on its own, but sometimes sutures are required on the gum. This treatment with iodine continues for at least 6-7 days until full granulations are formed and the defect is closed. In this case, the tampon is not removed from the hole so as not to damage the blood clot.
It is also possible to temporarily close the defect with a small plastic plate, which is fixed to adjacent teeth with clasps. It separates the oral cavity and sinuses, which promotes healing of the perforation.
At the same time, a course of preventive measures is prescribed, aimed at preventing the development of inflammatory complications. It includes taking antibiotics, anti-inflammatory drugs, drops with a vasoconstrictor effect. This course is carried out on an outpatient basis or at home.
If, during perforation, foreign bodies penetrate into the sinus (implant, filling material, fragment of a tooth root), then treatment is carried out only in a hospital setting. In this case, an operation is indicated to open the cavity of the maxillary sinus, remove the foreign body and non-viable tissue, followed by plastic closure of the perforated defect.
»
How to treat?
The tactics for eliminating the problem depend on exactly what causes led to the perforation and what the general clinical picture is. Almost always, repairing a perforation requires surgery, the only exception to this rule is when a hole was created during a tooth extraction, provided that the dentist found it immediately and no foreign objects or infection got inside. If the problem is identified immediately, it is important to keep the blood clot in the place where it formed and prevent it from becoming infected - it will become a natural barrier to the infection entering the sinus. Protecting a blood clot from infection is carried out using a tampon with an iodine solution, which will have to be kept for at least a week.
In some cases, the doctor chooses the tactic of suturing the gum tissue. Another alternative is to install a compact plastic plate that is attached to adjacent teeth and acts as a barrier between the oral cavity and the sinus until the septum is restored.
For obvious reasons, physical barriers cannot provide a 100% guarantee that infection will not penetrate the hole, so the doctor additionally prescribes vasoconstrictors and anti-inflammatory drugs. They can be taken at home, but sometimes require the patient’s outpatient presence.
Penetration of any foreign objects into the maxillary sinus is regarded as a serious complication, which automatically means the need for surgical intervention and hospital treatment. In such a situation, the sinus is opened, removing foreign objects and tissues that cannot be restored, after which the fistula is covered with the patient’s tissues.
Old perforations
If the perforation of the maxillary sinus was not promptly identified and eliminated, then after 2-4 weeks the stage of acute manifestations will subside, and a fistula will form in the area of the defect, connecting the sinus cavity with the surface of the gum.
This process is simultaneously accompanied by symptoms of chronic sinusitis:
- constant dull pain in the sinus area radiating to the orbit and temple;
- nasal congestion on the affected side;
- purulent discharge from the nasal cavity, as well as from the fistula;
- Sometimes patients have swelling of the cheek on the side of the damaged sinus.
Most patients also complain of a sensation of air moving through the fistula when talking or sneezing, difficulty pronouncing certain sounds, and liquid food entering the nasal cavity from the mouth.
Treatment of such chronic perforations with fistulas presents some difficulties, since the presence of a chronic focus of inflammation in the maxillary sinus significantly reduces the effectiveness of therapy and quite often leads to relapse and re-formation of the fistula canal.
Such patients are indicated for surgical intervention, which includes opening the maxillary sinus with removal of all non-viable tissues and foreign bodies from its cavity, excision of the fistula and plastic closure of the defect. Antibiotics after removal of the fistula are prescribed for a course lasting 10-14 days with the simultaneous use of anti-inflammatory and antihistamine drugs, and the use of physiotherapeutic methods of treatment.
Symptoms
It is important to understand that the maxillary sinus is not isolated. Air circulates constantly in it. Therefore, if there is this pathological condition, then the flowing blood will contain air bubbles. In addition, part of the blood mass will penetrate into the sinus.
To make a correct diagnosis, you need to contact a highly qualified specialist who, based on the test results, prescribes the most effective therapeutic measures.
If a person has any doubts about the presence of pathology, he should immediately visit a dental surgeon or ENT doctor.
Among the most common signs that may indicate that there is damage to the maxillary sinus are:
- Bleeding of the tooth socket, which occurs after the procedure for removing a dental unit. In this case, a large number of air bubbles are observed in the blood. Their number, as a rule, increases when the patient takes a deep breath.
- Bleeding from the nostril closest to the injury site. As a rule, with high-quality removal, blood flows only from the hole.
- Voice change. The man begins to nasal. This condition is not immediately noticed after removal of a dental unit, since a tampon is placed in the oral cavity, which prevents conversation.
- The sensation of air flow passing through the hole formed after tooth removal. In this case, the patient notes pressure in the upper jaw.
When perforation of the sinus occurs during the implantation procedure, it is as if the surgical instrument sinks deeper than the distance at which it should be located. If such a situation arises, a competent specialist will immediately determine that the bone membrane has been perforated.
For minor injuries that were not noticed by either the specialist or the patient, more dangerous symptoms begin to appear:
- severe inflammatory process;
- formation of extensive purulent contents;
- frequent migraines;
- constant pain in the upper jaw.
When inflammation begins, the patient has difficulty breathing. There is swelling on one side of the nose. In addition, this process is accompanied by general weakness and increased body temperature.
If these symptoms occur, you should notify your doctor about a recently pulled tooth or implant placement.
Consequences of perforation
Perforation of the maxillary sinus is a fairly serious pathology that often has to be treated in a hospital. Attempts to independently treat it with folk remedies at home without medical assistance can lead to the development of serious and dangerous consequences:
- The development of a pronounced inflammatory reaction in the sinus cavity with the spread of infection to the surrounding bone tissue and the formation of foci of osteomyelitis of the upper jaw.
- Spread of inflammation to other sinuses of the skull (frontal, sphenoid and ethmoid).
- Loss of healthy teeth located in the area of untreated perforation.
- Formation of purulent foci (abscesses, phlegmons).
Due to the close location of the maxillary sinus and the brain, after perforation, infection may spread to the meninges with the development of meningitis or meningoencephalitis, which threatens the patient’s life.
Why shouldn’t you treat perforation of the maxillary sinus yourself?
To date, there are no effective treatments for perforation other than surgery. An attempt to cure yourself at home using “traditional medicine” means that time will be lost and the situation will become neglected. You can start the problem before complications arise:
- the sinus cavity becomes inflamed, the infection spreads to the bone tissue, the patient begins to suffer from osteomyelitis of the upper jaw;
- inflammation penetrates into other intracranial sinuses, and there are more foci of infection;
- next to the untreated perforation, the alveolar process is weakened, as a result of which healthy teeth may fall out;
- foci of suppuration develop.
The maxillary sinus is also located in close proximity to the brain. The lack of a timely response and the development of suppuration inside the sinus is fraught with meningitis and meningoencephalitis - these are diagnoses that directly threaten life.
Preventive actions
Prevention of perforations of the floor of the maxillary sinus consists of:
- in a full examination of the patient before complex dental procedures;
- in the correct assessment of the anatomical and topographical characteristics of each person;
- in strict adherence to the technology of therapeutic manipulations.
Timely detection of signs of perforation and its adequate treatment is the key to a favorable outcome for the patient. Incorrect therapeutic tactics or self-medication can aggravate the course of such a complication and cause the development of severe negative consequences.
Signs if perforation was left without the attention of a doctor
Symptoms of inflammation after unsuccessful treatment occur in different ways - after a few days, weeks or even years. Depends on the sterility of the foreign body in the sinus, its ability to cause inflammatory processes, and the characteristics of the patient’s immune system. The following manifestations are possible:
- feeling of heaviness;
- pain when chewing;
- purulent and serous discharge from one nostril;
- elevated temperature;
- impaired sense of smell;
- pain when lightly tapped under the eye and in the nose area.
These are typical signs of odontogenic sinusitis caused by poor quality dental treatment. The key difference from rhinogenic sinusitis (when sinus infection occurs from the side of the nasal passages as a result of ARVI or influenza) is that signs of the inflammatory process are detected only on one side, where treatment was carried out.
What to do if perforation does occur?
Unfortunately, this happens from time to time. And further tactics depend, to a greater extent, on the size of the perforation.
First , and most importantly, DO NOT PANIC!
The second thing to do, regardless of the size and location of the defect, is to bring the perforations to the center of the aperture. To do this, the aperture will have to be expanded:
Third , mobilization of the edges of the perforation. It should be surrounded on all sides by normal mobilized mucous membrane of the maxillary sinus.
As a rule, this is enough for a small defect to close on its own. This happens according to the same principles as reducing the spot on a deflating balloon:
If this does not happen, there are different options for closing the perforation of the maxillary sinus mucosa during surgery. In any case, this is not a reason to stop the operation.
Option 1. Excessive mobilization of the mucous membrane of the maxillary sinus
This only works with small defects and with good mobility of the sinus mucosa.
The bottom line is this: the mucous membrane of the maxillary sinus is mobilized much more than necessary, this makes it possible to “tighten” the defect. Some surgeons suggest putting sutures in this case, but, firstly, this is not so simple, and secondly, this is not necessary, since the mucous membrane quite quickly restores its tightness due to its own elasticity and the formation of a blood clot:
The photograph shows how the mucosal defect in the right corner collapses and decreases in size. With further mobilization of the Schneiderian membrane, it disappears altogether.
Option #2. Using an autogenous bone fragment and/or a free de-epithelialized flap.
At RegenerationDay, I have repeatedly talked about the fact that any osteoplastic surgery, including sinus lifting, can be performed without the use of biomaterials at all. Another thing is that it is somewhat more difficult, longer and more traumatic.
However, with the “osteoplastic” creation of access to the maxillary cavity, we are left with an autobone fragment that could be used to close an accidental perforation of the mucous membrane of the maxillary sinus. It's very easy to do this:
This option has one disadvantage: it only works in cases of “osteoplastic” creation of an aperture, when we have an “extra” fragment of autologous bone. If access to the maxillary cavity was created in another way, then obtaining a de-epithelialized flap will require a donor site, which, in turn, increases the time and morbidity of the operation.
Option #3. Use of barrier membranes
In fact, this is the “classic” option for closing Schneiderian membrane perforations. The idea is simple - we use a barrier membrane such as Bio-Gide or Jason, covering the defect by an average of 30%. Thus, we can close even very large perforations with a fairly predictable result:
First, we detect and highlight the mucosal defect so that it is reduced as much as possible:
select a barrier membrane and adjust it to size:
glue the resulting “patch” and fill the subantral space with graft:
There is only one nuance in the use of barrier membranes when closing defects in the mucous membrane of the maxillary sinus. And it is directly related to the properties of barrier membranes.
Microbes live in the nasal cavity and maxillary sinus. This is, in fact, the same open environment; like the oral cavity, it has its own microflora. And barrier membranes are permeable not only to body cells, but also to bacteria. Therefore, if the barrier membrane opens into the lumen of the maxillary sinus, there is a risk of infection of the underlying graft (see “Success Factors for Osteoplastic Surgery. Factor #2 and Factor #3”). Therefore, before “sealing” the resulting hole in the mucous membrane with a patch of barrier membrane, you need to bring the edges of this hole together as much as possible. Ideally, pull it off completely. So that the membrane does not open into the nasal cavity. Thus, you will significantly reduce the likelihood of graft infection and make the result of the operation more predictable.
This option has another significant disadvantage, namely the cost of the barrier membrane. If you did not initially intend to use it, then it will be very difficult for you to explain to the patient why his operation began to cost more than he originally expected.
Option #4. Use of collagen matrices
I would like to dwell on this option in more detail.
In case of perforations, until recently we used barrier membranes in 100% of cases. However, barrier membranes have one significant drawback - they are permeable not only to cells, but also to bacteria. This means that the microflora, which is always present in the maxillary sinus (this is the same open environment as the oral or nasal cavity), may well infect the graft through the barrier membrane and worsen the results of the operation (see “Option #3” above).
Is there a biomaterial that is not afraid of an open environment? At the same time, is it as easy to use as a barrier membrane?
Yes, it exists. This is a collagen matrix.
not necessarily Geistlich Mucograft, but with similar properties.
Unlike the barrier membrane, the collagen matrix is designed to be “open”, and its structure prevents the penetration of microflora into the underlying graft. This is why we use them to augment tooth sockets after extractions.
Let me give you a simple example.
During the sinus lift operation, we developed a small perforation of the Schneiderian membrane:
We start by bringing it to the center of the aperture, and mobilize the edges along the way. As a result, it decreased somewhat in size:
What should I use to seal it?
In this case I used Geistlich Mucograft Seal 8mm. Biomaterial in this form factor is cheaper than a barrier membrane, and its diameter allows you to easily cover the resulting mucosal defect:
It is better to wet Mucograft before positioning. It will become more elastic (without loss of strength) and soft:
After which, it easily sticks and covers the defect:
All we have to do is fill the resulting subantral space with a graft (Bio-Oss) and complete the sinus lift and osteoplasty operation as we planned:
The disadvantage of this option is that the Mucograft collagen matrix of comparable dimensions to the barrier membrane, for example, 15x20 mm, is more expensive. In addition, Geistlich itself does not approve of this approach, citing established protocols and instructions for the use of biomaterials. However, I find it very convenient and affordable, because the largest number of perforations are less than 5-6 mm in size, which makes it easy and relatively inexpensive to cover them with Mucograft Seal 8 mm. Well, in my opinion, the collagen matrix, due to its properties, will relatively calmly survive contact with the microflora of the maxillary sinus and will not allow it to infect the underlying graft.
Actually, the result of this approach, despite the objections of Geistlich Pharma AG, was very good:
So, this option deserves, if not active implementation, then at least attention from both the manufacturer and implantologists.
Option #5. Refusal to continue the operation
As you can see, perforation of the mucosa during sinus lift is not a problem at all. One way or another, we can cover the defect and calmly continue the operation. However, a reasonable question arises: “To what extent and to what size can we close the perforation?
In the article about sinus lifting, I write that perforation with a diameter of more than 1 cm is a reason to complete the surgical operation and postpone sinus lifting until complete rehabilitation. However, this was before this incident happened in my practice. I won’t repeat myself, anyone interested can read it here>>
This case clearly showed that even large defects of the mucous membrane, significantly larger than 1 cm in diameter, are completely closed and make sinus lifting possible. Therefore, we have no unfinished operations for a long time.
How is the treatment carried out?
We respect the patient’s personal time and strive to carry out all activities comprehensively, in one day :
- Professional hygiene Preparation of the oral cavity to ensure sterility during surgery to avoid secondary sinus infection
- Surgery to eliminate inflammation Performed while you sleep; the method of access to the sinus is selected depending on the location of the foreign body and the presence of tumors
- Temporary prosthetics If the causative tooth had to be removed, a temporary crown or immediate prosthesis is installed to mask the defect
Surgical operations in our Center are performed under sedation. The patient does not feel anything, fears and worries are excluded. Sedatives put you into a controlled drug-induced sleep without falling into unconsciousness - this is not general anesthesia! They do not contain toxic components, act gently, preserving reflexes. The artificial lung ventilation device is not connected, hospitalization is not required.
The surgical intervention is completed by a mandatory CT examination , which is necessary to assess the quality of the work performed.
After 10-14 days, the patient is invited to the clinic for suture removal and a control CT image. A schedule of professional inspections is drawn up.