How is nitrous oxide used in dentistry?
Nitrous oxide, or laughing gas, as it is popularly called, was invented at the end of the 18th century by physicist John Priestley. For a long time, the invention could not be used: the gas with a pronounced sweetish taste was absolutely useless at first glance, but had a number of interesting properties. After inhalation, the person became cheerful, relaxed and experienced a feeling similar to intoxication. As usually happens, fans of this gas, or rather, its effects, quickly appeared. Nitrous oxide was used by clowns and circus performers to further excite and make the audience laugh. Over time, another interesting property was discovered: while under the influence of laughing gas, people did not seem to feel pain and treated it quite calmly. Dentist Horace Wells was the first to use nitrous oxide in dental treatment. Despite the fact that the first experiments gave positive results, public experiments were unsuccessful, and in one case the patient almost died. His colleague Wells Morton was more successful in using nitrous oxide, so he is considered a pioneer in this field. Of course, in the past, the gas formula and dosage were far from perfect, so treatment with nitrous oxide was not so predictable. In its modern version, sedation with nitrous oxide has been carried out since the late 40s. It was then that doctors began adding oxygen to the mixture and using special devices, including cylinders, a rotameter and a mask.
Nitrous oxide sedation: new views on an effective method
A mixture of nitrous oxide and oxygen (N2O/O2) is completely safe and has been successfully used for over 160 years to relieve pain and anxiety. In the early 1800s, dentist Horace Wells dedicated his life to promoting nitrous oxide in both general medical and dental practice. Because he promoted the use of nitrous oxide for pain control, he was posthumously given the title of "Discoverer of Anesthesia." Since that time, the method of sedation with nitrous oxide has become one of the most common in dental practice, in addition, it began to be used as a premedication at the beginning of the general anesthesia procedure.
Very often, dental patients seek help already with certain signs of pain or anxiety. Moreover, the feeling of anxiety can be associated directly with the visit to the dentist itself. Consequently, the doctor has to relieve these two sensations at once, since they are interrelated. The use of a mixture of nitrous oxide and oxygen at minimal cost allows you to effectively and safely deal with emotionally difficult clinical situations in dental practice. In this article, we will describe the main characteristics of nitrous oxide, indications for the use of the N2O / O2 mixture, and also analyze the main facts and myths associated with the long-term effects of nitrous oxide on the body, the biological effects of this gas, and approaches to minimizing the risk of contamination of the dental office space through N2O.
Advantages
Nitrous oxide/oxygen (N2O/O2) sedation offers a number of advantages over other sedation methods or alternative pharmacological agents. The properties of nitrous oxide allow this gas to not only relieve pain, but at the same time reduce anxiety. However, this effect is limited and observed over a short period of time. Nitrogen sedation can also be used in the treatment of patients with bronchial asthma, in which case the role of the gas is limited to the fact that it allows minimizing the effect of provoking stress factors. Nitrous oxide can be titrated, meaning that additional doses can be given to the patient over time until the desired level of sedation is achieved. Gas is eliminated from the body at almost the same rate as its accumulation. Most of the injected gas is eliminated through the lungs within a few minutes after stopping its supply and starting to breathe pure oxygen. You can also help remove nitrous oxide from the body by breathing regular air, but this manipulation will take a little longer. N2O/O2 mixture can be safely used among patients of all age groups. In addition to its main actions, it also allows you to somewhat suppress the gag reflex, thus creating conditions for conducting x-ray examinations and taking impressions. There are only a few contraindications to the use of nitrous oxide in dental practice, since its effect on the human body in general is neutral rather than negative.
Contraindications
In some situations, the use of N2O/O2 sedation should be delayed or avoided. When planning to undergo sedation, you should always seek the advice of your physician. The following are conditions under which it is imperative that the patient consult with a physician prior to undergoing sedation, and if consultation is not possible, the procedure should be postponed until the conditions described below have been completely relieved.
The use of medications during the first trimester of pregnancy is not recommended, therefore, exposure to nitrous oxide should be avoided. It is recommended to carry out any dental interventions in the second trimester. Similarly, with complete safety, a mixture of nitrous oxide and oxygen can be used in the second and third trimester of pregnancy, but, of course, after consultation with your doctor.
An upper respiratory tract infection (such as sinusitis) often causes nasal congestion, which may prevent gas from entering the respiratory system. In such cases, it is better to start sedation after the underlying disease has resolved. The use of a N2O/O2 mixture in cases of emphysema and chronic bronchitis is problematic; in these disorders, the use of sedation is prohibited due to the impossibility of ensuring proper airway patency. If you have chronic obstructive pulmonary disease, the use of sedation is possible only after consulting your doctor. Given that nitrous oxide has expanding properties, its use is limited in cases of active cystic fibrosis. Likewise, it is not advisable to use nitrous oxide after ophthalmic surgery. Certain complications after sedation can develop in patients after repair of the eardrum. As a result of the gas expansion phenomenon, complications with nitrous oxide use are predicted to occur in patients with pneumothorax or constipation.
On the other hand, patients with such pathological conditions rarely seek dental care until treatment for the above-mentioned disorders is completed. Patients taking bleomycin sulfate as a drug to treat certain types of cancer have an increased risk of developing pulmonary fibrosis. This outcome is associated less with the influence of nitrous oxide than with the influence of oxygen itself (at a concentration of more than 30%). But such situations (using bleomycin and performing sedation at the same time) are rather exceptions. According to the literature, after performing pneumoencephalography, there is an increase in intracranial pressure due to the fact that nitrous oxide replaces nitrogen molecules. Therefore, after pneumoencephalography, nitrous oxide sedation should be postponed for at least a week. One should be extremely careful when using sedation for psychological illnesses, and exclude the possibility of performing this manipulation when the patient is under the influence of drugs. It is also undesirable to perform sedation among patients who do not fully understand the essence of the manipulation due to impaired consciousness (for example, with Alzheimer's disease), as well as among patients taking psychotropic drugs. But it should be remembered that in addition to nitrous oxide sedation, there are other options that can be used in the above situations.
Based on our experience, we also recommend avoiding nitrous oxide sedation in patients with whom you cannot communicate well due to a language barrier, as well as in patients who suffer from claustrophobia and who have difficulty putting on and maintaining a mask in position. It is extremely important that the physician performing sedation is familiar with all evidence-based information regarding aspects of the implementation of this manipulation.
Evidence-Based Research
An evidence base is a necessary component for the implementation of effective dental treatment. There are several reports in the literature of the effects of nitrous oxide as an occupational risk factor. Historically, nitrous oxide has been associated with many disorders, ranging from birth defects to neoplasmic lesions. However, recent research indicates that low concentrations of nitrous oxide, such as those reported in dental office settings, are completely safe for dentists to use. It is also necessary to note the effectiveness and safety of new types of devices used for nitrous oxide sedation procedures. Of the 800 dental publications discussing the effects of nitric oxide that were published before 1995, only about 25 met the required parameters for reliability and validity. Many of the above-mentioned studies were conducted using retrospective designs, which in themselves are not very statistically reliable unless all methodological criteria are adhered to to the required extent. The first study of nitrous oxide as an occupational risk factor was published in 1967: a Russian researcher pointed out reproductive problems that were noted among anesthesiologists working in direct contact with the gas. Similar publications were presented in the United States in the late 1970s and early 1980s. But since then, methods for storing, supplying, dosing and using nitrous oxide have improved significantly. Nowadays, all such systems for working with gases are also equipped with special units for intake and purification of the surrounding air from traces of nitrous oxide. In addition, completely new systems for supplying nitrous oxide as a sedative agent continue to appear on the market, which are conceptually different from older analogues.
In one influential study from 1985, Sweeney and colleagues used an extremely sensitive deoxyuridine inhibition technique to identify critical levels of nitrous oxide concentrations. So, based on the results obtained, the visible biological effect of nitrous oxide is observed only at a concentration of 1800 parts per million (ppm). To date, there has not been a single clinically confirmed case of negative biological effects of nitric oxide in dental working conditions at the low levels of gas that are observed in the air during and after the sedation procedure.
Biological effects
The most significant biological effect associated with nitrous oxide exposure is its ability to inactivate vitamin B12. This mechanism affects an enzyme called methionine synthetase. Methionine synthetase, in turn, is essential for DNA production. Impaired fetal development was found in animals that were exposed to 60% nitrous oxide 24 hours a day for 12 days. The negative chronic effect of nitrous oxide on human reproductive function was discovered only in the conditions of incorrectly conducted studies, the subjects of which were exposed to high concentrations of the gas in the complete absence of cleaning of work areas. As for DNA synthesis disorders, such a risk is associated only with women during pregnancy, or with women planning to become pregnant. However, it is best to know the exact levels of nitrous oxide in a room before doing any work in it. The toxic effect of nitric oxide on the human body is the subject of debate in modern scientific literature. Despite this, available data indicate that the gas is completely safe when used in limited therapeutic doses. Neurological symptoms associated with nitrous oxide include numbness, tingling, and in some cases paraesthesia of the extremities, clumsiness, slow gait, altered reflexes, and muscle weakness. It is logical that the severity of these disorders is associated with the duration and dose of exposure to nitrous oxide. Cases of nitric oxide overdose reported in the literature have involved exposure to the gas for several hours a day for two weeks straight. However, some people exposed to chronic nitrous oxide indicate resolution of symptoms after the gas stops, and some indicate their permanent nature.
Concentration control
The National Institute for Occupational Safety and Health (NIOSH) and the American Conference of Industrial Hygienists (ACGIH) have been instrumental in developing recommendations regarding threshold levels of nitric oxide during human work activities during an 8-hour workday. In 1977, these organizations established nitric oxide concentration limits for health care workers. It has been determined that in operating rooms and dental offices, nitrous oxide concentrations should not exceed 25 and 50 parts per million, respectively. These levels were established based on the results of preliminary studies by Bruce, Bach, and Arbit, as well as the characteristics of the equipment used. These critical concentration levels are still relevant today. The Occupational Safety and Health Administration (OSHA) is the organization that has the authority to enforce these recommended levels; however, because of controversy regarding their appropriateness, OSHA recognizes that it would be desirable to revalidate such concentration limits.
To address several pressing issues regarding nitrous oxide, a meeting was convened in October 1995 by the Council on Scientific Affairs of the American Dental Association. It brought together several stakeholders, including respected experts in the field, educators, manufacturers and government officials. It was concluded that the true recommended exposure limit for nitrous oxide cannot be clearly established. Sweeney et al proposed a concentration level of 400 ppm as a cutoff. In their opinion, this level is the most commonly achieved, and is much lower than the 1800 ppm level at which the biological effects of nitrous oxide were first recorded. Other countries have adopted the following nitrogen oxide exposure limits: from 25 ppm in France and Denmark to 100 ppm in Sweden and Germany.
Estimation of nitrous oxide concentration levels
To determine whether traces of nitrogen oxide are present in a room, levels must be objectively measured in parts per million. To do this, they use a device - an infrared spectrometer, which allows you to determine the concentration of not only nitrogen oxide, but also other gases in terms of parts per billion (ppb). Of course, there is no point in buying it purposefully, but you can rent it either directly from the manufacturer or at a local hospital. In addition, the spectrometer allows you to detect areas of gas leakage from containers containing it. Another approach to estimating nitric oxide concentrations is to determine the amount of nitric oxide a person is exposed to over a period of time. To do this, the measuring device is simply put on, like a dosimeter, and carried with you for several hours. Thus, the time-weighted average (TWA) of nitrous oxide absorption is determined by its amount in the collecting tank of the measuring device.
Minimizing the risk of contamination
It is extremely important to pay due attention to measures to reduce the risk of nitrous oxide contamination. Disposal of trace gases can be ensured before, during and after use for dental purposes. Leakage of small amounts of nitrous oxide can occur in the area of all equipment connections, regardless of the specific use of portable or stationary equipment. To avoid this, manufacturers recommend periodic monitoring of the equipment used. Each manufacturer provides the necessary information regarding the frequency with which control measurements should be carried out, on average twice a year. Using ordinary soap and water, you can easily identify problem areas in terms of gas leaks in the system you are using. In addition, it is extremely important to ensure the reliable functioning of systems for the extraction of gas residues that form outside the nasal tube during its supply.
It must also be remembered that nitrous oxide can enter the doctor’s body not only due to system problems, but also directly from the patient. To minimize this effect, it is extremely important to limit conversation with the patient during the manipulation, because the gas that he inhales easily exits through the oral cavity. In addition, it is necessary to ensure that the mask fits snugly, taking into account its proper size. Sometimes all that is required for a tight fit of the mask is simply to form the necessary bend in the conductive tube. Despite the fact that nitrous oxide is much heavier than air, and even when it spreads outside the mask and tube, it immediately “falls” to the floor, this gas is also extremely expansive in nature. In other words, it spreads very quickly and easily over the entire surface area. On the other hand, the partial pressure of nitrous oxide is 31 times that of air, increasing the chance of it entering the physician's airway before it reaches the floor surface in cases of leakage.
Recommendations for monitoring nitrous oxide impurities in workroom air
Below is a list of recommendations and preventive measures aimed at minimizing the level of nitrous oxide contamination in the dental office environment.
- It is necessary to first establish the baseline concentrations of nitrous oxide in the clinic and in the surrounding air using an infrared spectrophotometer.
- To assess personnel exposure to gas, it is recommended that time-weighted instruments be used.
- Every 2 years, send equipment to the manufacturer for routine maintenance and evaluation.
- Provide visual monitoring of the integrity of conductive tubes and reservoirs.
- Use the "soap suds" principle to check the tightness of connections for possible gas leaks. To do this, add a few drops of detergent to a small amount of water, and wipe the areas of connections, reservoirs and conductive pipes with this solution. If there are gas leaks, bubbles will form.
- Ensuring effective evacuation of gas traces.
- It is necessary to assess the effectiveness of room ventilation and air exchange. In certain cases, measures may be required to improve the existing ventilation system to reduce the level of gas residues in the indoor air. Some air conditioning systems do not provide air exchange at all, but operate on the principle of recirculating existing air.
- Provide full information support to operating personnel regarding the possible risks of complications associated with chronic exposure to nitrous oxide.
Summary
The sedative effect of nitrous oxide allows you to optimize the treatment process for patients with existing fear of dental interventions. The use of this gas is justified by a number of advantages and only a small number of disadvantages. Understanding the principles of reducing the effects of nitric oxide on clinical staff is also an important factor in its effective use. Dentists should be fully aware of the new facts and basic concepts of the use of laughing gas in their daily practice, while paying special attention to monitoring the concentration of this gas in the air of the working environment. If you would like to know more about local restrictions regarding critical values for nitrous oxide that are relevant for your country or region, we recommend that you contact the appropriate quality control authorities for the provision of dental and medical care for information.
Authors: Ann Brunick, RDH, MS Morris S. Clark, DDS, FACD
Indications for treatment under ZAX
One of the main advantages of nitrous oxide is its safety: the gas is eliminated from the body in the shortest possible time and in an unchanged state. To recover from the state of sedation, no special antidotes are required, which is very important when treating children’s teeth. After 10–15 minutes, the little patient returns to his normal life and does not feel any side effects. Dental treatment with nitrous oxide for children is carried out very often and has a number of indications.
- Fear of the dentist. Any treatment under sedation can reduce fear of the doctor. Few children are not nervous before the appointment, so sedation is an ideal procedure for relieving stress.
- Preschool age. At a very young age, the use of potent drugs and tranquilizers is prohibited or not recommended. In this regard, nitrous oxide is a better solution.
- Pronounced gag reflex. Laughing gas not only does not provoke, but even suppresses the gag reflex.
Experts recommend using nitrous oxide in dentistry for children for no more than 1 hour. During this time, a fairly large number of manipulations can be performed, including treating pulpitis or periodontitis. If longer or complex treatment is required, then it is better to split it into several stages.
When will nitrous oxide treatment be effective?
1. Age over 3 years. Children are not psychologically ready for this type of manipulation and may be scared.
2. The child sits in the dental chair by himself - without panic fear or hysteria, but at the same time experiences slight discomfort. In this case, the oxygen mixture will help you relax and take your mind off unpleasant sensations.
3. Nasal breathing. The mask should remain on the face throughout the entire procedure, tightly covering the nose. This is due to the fact that the effect of the gas occurs gradually. First, the patient breathes pure oxygen, then the anesthesiologist gradually changes the gas ratio, increasing the nitrogen concentration. If you periodically remove or adjust the mask, the desired effect will not be achieved.
Contraindications
Today, nitrous oxide is used almost everywhere, and reviews of the procedure are mostly positive. This was largely because the use of this gas does not require a special license, which is required for other types of sedation using psychotropic substances. Because of this, ZAKS is sometimes taken quite lightly. Meanwhile, this procedure has an impressive number of contraindications and restrictions that must be kept in mind to avoid complications and side effects:
- the age of the patients is too young—ZAKS is not recommended for children under three years of age;
- upper respiratory tract diseases (colds, runny nose, rhinitis, sinusitis);
- adenoids;
- otitis in the acute stage;
- traumatic brain injuries (3 months or earlier before the start of treatment);
- seizures and epilepsy;
- lack of possibility of contact with a doctor - when performing ZAKS, the doctor must understand the child’s condition and reaction;
- individual manifestations of the reaction (convulsions, allergies, reverse reactions).
Side effects of ZAX are usually associated with the individual reaction of the child’s body to the components of the mixture. It happens that instead of a relaxed and calm state, we get the opposite reaction: hyperactivity, sudden movements, panic states. In this case, the gas supply should be stopped immediately, as there is a high risk of harming the child and only increasing his fear of dental treatment. If allergic reactions occur (shortness of breath, cough, redness), the doctor should also interrupt the procedure and give the patient antihistamines.
Technology of low-flow gas anesthesia
Aspects of low-flow anesthesia have been actively discussed by specialists over the past decades. Interest in this problem has resurfaced due to the development of new technologies. The attention of researchers is also attracted by such factors of low-flow anesthesia as cost-effectiveness, physiology and environmental friendliness.
Recently, very effective vapor anesthetics have begun to be used in medicine: desflurane, isoflurane, sevoflurane, ethrane. Xenon (medical) also appeared, a gaseous anesthetic of the latest generation. In this regard, the use of high-flow anesthesia, which has traditionally been used in medical practice, has become impractical.
Nevertheless, the widespread introduction of low-flow anesthesia in Russian clinics is complicated by the lack of modern anesthesia and respiratory equipment. As it turned out, our country does not produce anesthesia machines that could ensure the implementation of anesthesiological procedures with a minimum gas flow. To be fair, it is worth noting that imported anesthesia equipment cannot provide anesthesia using xenon.
According to statistics, more than 3 million anesthesia procedures are performed in Russian medical institutions per year, most of which are performed using high-flow technologies, which is extremely wasteful both economically and environmentally inappropriate. Moreover, this method inherently contradicts human physiology. In addition, most Russian anesthesiologists do not know the basics of low-flow anesthesia.
Rice. 1 Anesthetic workstation Aisуs CS2
A little history
Attempts to use a completely closed circuit during anesthesia were made by doctors a long time ago, when anesthesia machines were far from perfect. But doctors were able to fully appreciate the advantages of the low-flow method only in the 70s of the last century, with the advent of more advanced anesthesia equipment and technical means that allowed intraoperative monitoring of the concentration of vapor and gas anesthetics.
In our country, closed-circuit gas anesthesia was first used by T. M. Darbinyan, performing heart surgery on children, but the method became more widely used years later, in the late 90s, and only in those clinics that had anesthesia-respiratory facilities systems of foreign production.
Minimum flow xenon anesthesia first entered domestic practice in 1992. It was used in the S.P. Botkin City Clinical Hospital by doctors N.E. Burov and D.A. Dzhabarov. The use of xenon has shown the inadequacy of domestic anesthesia units, adapted exclusively to high-flow anesthesia. Until 2003, there were no certified anesthesia machines suitable for using xenon in Russia at all. And only towards the end of 2003 such equipment began to be used.
With the advent of isoflurane, snevoflurane, desflurane and other halogen-containing anesthetics, low-flow anesthesia using devices, usually foreign-made, began to be introduced in Russia, although not very actively. But there was still no certified xenon equipment among them. Recently, anesthesia machines designed for closed-circuit anesthesia based on 4 liquid and 2 gas anesthetics have appeared in domestic medicine and are being successfully used.
Serial production of such anesthesia-respiratory units in Russia will significantly reduce the technical gap with developed foreign countries in the field of anesthesia.
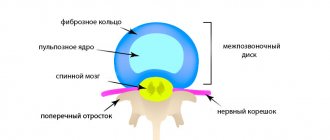
Types of breathing circuit
Based on the decision of the International Commission for Standardization, the breathing circuit can be reversible or non-reversible. Based on its functional features, it can be:
- open;
- half open;
- half-closed;
- closed.
Experts classify the reversible circuit as: semi-closed, pendulum and completely closed, and the non-reversible circuit as open and half-open.
The circulation system is considered the most optimal for low-flow anesthesia in children and adults. Its variety is determined by the amount of fresh gas flow. If the gas flow is higher than the metabolic demand for oxygen and the absorption rate of other gas anesthetics, then the anesthesia system operates in a closed circuit. If the flow of the fresh gas mixture is more than 1.5 times higher than the MBL value, then the circulation system operates in a semi-open circuit, which prevents the accumulation of carbon dioxide even in the absence of an adsorber.
The amount of gas flow determines the following types of anesthesia:
- high-flow, with a gas flow of more than 6 liters per minute;
- medium-flow, with a gas flow of more than 3 liters per minute;
- low-flow, with a gas flow of more than 1 liter per minute;
- minimal, with a gas flow of less than 1 liter per minute.
Anesthesia can be performed in a closed circuit if the fresh gas flow and gas uptake are equal.
Pharmacokinetics of gases
Nitrous oxide is not metabolized in the human body. From the moment it enters the circuit, it is absorbed by tissues within 20 minutes. As the tissues become saturated with nitrous oxide, its further absorption decreases and stops at the level of a flat curve. The absorption of nitrous oxide by tissues is calculated using a special formula.
Xenon has a lower solubility coefficient than nitrous oxide, so it is absorbed by tissues three times less. The human body consists of heterogeneous tissues, and their solubility coefficients are different, so it is quite difficult to accurately calculate the volume of soluble xenon. For example, a patient has 10 kg of adipose tissue. Up to 1700 ml of xenon can additionally dissolve in it, the total volume of gas in this case will be 8400 ml. It is estimated that to achieve a xenon concentration of up to 70%, an 80 kg patient would require approximately 8400 ml of xenon. Then the level of anesthesia will dynamically stabilize. This volume of anesthetic will be sufficient to maintain the surgical stage of anesthesia in a closed circuit for 2–3 hours. In this case, the tightness of the circuit should not be compromised. The absence of an open wound surface is also important. A situation is created that is unique in its essence, when the anesthetic that enters the patient’s body is retained in it at a stable narcotic concentration and participates in repeated recirculation in a closed circuit.
Xenon elimination occurs quite quickly. After just 5 minutes, up to 95% of all xenon dissolved in the body is released through the patient’s lungs. The patient awakens 2–3 minutes after the supply of gas anesthetic is stopped.
It is important to note that the pharmacokinetics of xenon during low-flow anesthesia requires further study and clarification, based on the characteristics of organs and tissues. Their pronounced, medium and low perfusion, different degrees of gas solubility in tissues, the speed of elimination of the anesthetic and the period of its post-anesthesia action should be taken into account.
Features of low-flow gas anesthesia
At the end of the usual premedication and intubation, denitrogenation is performed with pure oxygen, the total volume of which is 50–60 l, the concentration of alveolar nitrogen is reduced to 0.5%. After denitrogenation, the oxygen gas flow is set at the rate of 4 ml per kilogram of the patient’s body weight. The anesthetic gas flow (nitrous oxide or xenon) is calculated at a fourfold increase in relation to the oxygen gas flow.
After 15 minutes, the nitrous oxide level will be 65–70%, and a persistent narcotic concentration of this anesthetic will occur. With xenon anesthesia, a stable narcotic concentration of this substance is achieved much faster. This will take about 5 minutes.
Having reached a stable narcotic concentration of the anesthetic, the gas flow is adjusted to minimum flows under the control of the fractional concentration of oxygen in the inhaled gas mixture. Its level should not be lower than 30%. The minimum gas current is maintained throughout the entire period of anesthesia. 15–30 minutes before the end of the surgical intervention, the xenon supply is stopped, but a ventilator is connected via a closed circuit. After the operation, xenon is removed from the patient’s body using pure oxygen, which is supplied by a gas flow of 3–4 liters per minute. Exhaled xenon enters a special adsorbing unit, where it is utilized. After 2–3 minutes have passed after completion of the xenon supply, the patient regains consciousness. Low-flow xenon anesthesia is tens of times cheaper than medium-flow anesthesia.
Technical requirements for anesthesia equipment
Based on the design features, there are two types of respirators that are part of inhalation-type anesthesia devices:
- with continuous gas supply;
- with intermittent gas supply.
It is worth noting that many models of imported anesthesia equipment are not able to provide low-flow anesthesia if the total flow decreases to the level of 500 ml per minute. This is due to the fact that during the expiration period, if there is a lack of gas-narcotic mixture, ambient air is sucked into the breathing circuit. This creates a threat of dangerous gas anesthesia.
The requirements of the International Standards Commission reflect that when using respirators, it is necessary to adjust the total gas flow. Anesthesia using xenon becomes more expensive, since a large volume of gas is used. For this reason, an anesthesia-respiratory unit that provides for the supply of gas to the breathing circuit during the expiratory phase of the respiratory cycle will be more economically profitable.
Dental treatment in children with nitrous oxide: how does it work?
As already mentioned, the use of nitrous oxide occurs almost everywhere. Although the procedure is relatively simple, it should only be performed by a licensed anesthesiologist. In addition, if the clinic offers sedation services, there should also be a resuscitator on duty who can provide first aid if the need arises. The procedure begins with preparation. 10 hours before sedation you need to stop eating and come to the clinic on an empty stomach. If the child is small, then preparation for sedation is done in a playful way so as not to frighten or embarrass him. The process of sedation with nitrous oxide begins by first delivering 100% oxygen at a certain rate. Then nitrous oxide is added: its concentration ranges from 30 to 50%. Then the doctor administers local anesthesia, since the ZAX is designed to calm the child and remove stress, and pain relief is carried out separately. During the treatment process, the doctor communicates with the child, monitors his condition and, if necessary, asks him to take certain actions. After the manipulations are completed, the supply of nitrous oxide stops, and after 10–15 minutes the gas completely leaves the body.
A few recommendations before using nitrous oxide-oxygen
If you or your child is undergoing sedation, you must:
- firstly, you need to limit your food intake before the visit (a light snack is enough), because a full stomach can cause dizziness or mild nausea;
- secondly, the dentist should be warned about respiratory diseases, if any, as they may interfere with the achievement of the effect of sedation.
The doctors of our clinic will carefully and professionally perform sedation using nitrous oxide-oxygen so that visiting the dentist will be a pleasant and desirable procedure for you!
Low-flow anesthesia is a technique for performing inhalation anesthesia (usually as part of a combination), in which the fraction of the gas mixture returning to the reverse circuit is at least 50% of the initially inhaled volume. In this regard, definitions in which low-flow anesthesia is considered as inhalation anesthesia with a fresh gas flow of less than 2 l/min (according to others - less than 1 l/min) seem incorrect, since for patients with low body weight (young children) such a flow will not lead to recirculation of the respiratory mixture; therefore, such anesthesia cannot be considered low-flow.
Along with the above, for adult patients, the concept of minimal flow anesthesia (fresh gas flow 0.5 l/min) and closed circuit anesthesia (oxygen flow 250 ml/min) are distinguished.
The main prerequisite for the spread of low-flow anesthesia was the emergence of modern expensive inhalational anesthetics, in particular sevoflurane. It is obvious that the use of low or minimal carrier gas flows makes it possible to reduce the use of an inhalation agent by tens of times. Moreover, this technique has a pharmacoeconomic effect only if the duration of anesthesia is at least twenty minutes.
All anesthesia and respiratory devices offered by our company (models Ather 6, Ather 6D, Ather 7 and Ather 7D/C) allow for low-flow and minimal-flow inhalation anesthesia.
One of the prerequisites for low-flow anesthesia is the availability of full gas monitoring. Inhaled and exhaled concentrations of oxygen, carbon dioxide, inhalational anesthetic and nitrous oxide (if used) must be monitored. The second condition for low-flow anesthesia is the tightness of the breathing circuit, since if there is a discharge of the respiratory mixture (usually at the circuit-patient level), anesthesia with low flows of fresh gas will be impossible. Due to the latter requirement, it is possible to use only sealed devices to ensure airway patency (endotracheal tube or laryngeal mask).
The technique of low-flow anesthesia without the use of nitrous oxide includes the following steps. First there is a high flow phase (4-5 L/min), which may take about 10 minutes, depending on the anesthetic used and the patient's data. The ratio of oxygen and air concentrations is usually 1:3. In this case, the evaporator is set to high (but not maximum) concentrations of anesthetic until the target MAC value is reached. Upon reaching them, the fresh gas flow is reduced to 0.5–1 l/min, while increasing the concentration of anesthetic on the evaporator (for isoflurane to 6 vol.%, for sevoflurane - up to 5 vol.%). In the future, they focus on indicators of the concentration of anesthetic on exhalation. After the end of the main stage of the intervention, approximately 10 minutes before the end of the operation, the evaporator is turned off and the same flow of fresh gas is maintained. The patient is transferred to spontaneous breathing using the light-brown method or using the pressure support mode (PSV). 5 minutes before extubation, the remainder of the inhalational anesthetic is washed away with a high flow of fresh gas (5 l/min or more), after which the patient awakens.
If nitrous oxide is used, the technique changes somewhat. The initial high flow phase is produced using oxygen and nitrous oxide in a 1:2 ratio. In this case, the evaporator is set to the average concentration of the inhalation agent (1.5–2 vol.% for isoflurane and 2–3 vol.% for sevoflurane). The duration of this phase can be about 10 minutes. Upon reaching the required MAC value (or focusing directly on the concentration of the inhalation agent on exhalation), the fresh gas flow is reduced to 0.5–1 l/min, while the ratio of nitrous oxide and oxygen changes to 1:1. Subsequently, anesthesia is administered based on the concentration of the inhalation agent and nitrous oxide during exhalation. It should be remembered that the inspiratory oxygen concentration should not fall below 50% with a fresh gas flow of 0.5 l/min. 20-30 minutes before the end of the operation, turn off the evaporator, leaving the fresh gas flow low. The patient is allowed to breathe spontaneously, and then the remaining anesthetic gases are flushed out using high flow (5 L/min or more) 5–10 minutes before extubation.
When the fresh gas flow is 0.5 l/min or less, it is necessary to take into account the volume of gas that is taken from the circuit for the purpose of subsequent analysis, since its average intake rate can reach 200 ml/min when using a bypass gas analyzer. Therefore, to carry out minimal flow anesthesia, it is advisable to use devices that have the function of returning the analyzed gas to the circuit. Some models of anesthesia-respiratory apparatus independently return the test gas, while others require the connection of an additional line to the circuit for return.
Medical Internet conferences
Goal: to study the possibilities of new methods of anesthesia in dentistry
Objectives: 1. Study the history of the emergence of dentistry as an independent branch of medicine 2. Study the problems of the need to treat primary teeth 3. Study modern methods of sedation 4. Study the indications for the use of nitrous oxide in pediatric dentistry 5. Study the contraindications for the use of nitrous oxide in pediatric dentistry.
As a separate independent discipline, dentistry was formed not so long ago - at the beginning of the 20th century. This happened due to the merger of such areas of medicine as dental and maxillofacial surgery. However, the history of dentistry goes back to the Ancient World, when the first attempts were made to treat dental diseases. In Russia, dentistry developed in the era of Peter the Great, who gained a lot of new knowledge while traveling through European countries and brought from abroad a variety of devices for dental treatment. Although the first school of dentists in St. Petersburg opened only in 1881. And just a few years later, several hundred qualified dentists graduated from it.
In the 20th century, dentistry, having formed into a separate science, began to develop by leaps and bounds. As a result, today there are many durable and aesthetic materials, and doctors are able to restore almost any defect in hard tissues or dentition. Orthodontics today can correct almost any malocclusion. The development of local anesthesia and the introduction of new strong anesthetics have made almost all manipulations painless, which greatly facilitates treatment. Bad teeth occur not only in adults, but also in children. Therefore, pediatric dentistry is one of the most relevant areas of modern dentistry.
Some parents believe that there is no need to worry about diseases of children's baby teeth. After all, baby teeth will fall out anyway and be replaced by permanent teeth, and you shouldn’t bother with them. It's a delusion. Bad baby teeth will certainly lead to problems with permanent teeth. If the question arises - to treat a diseased tooth or remove it, the answer is clear - treat. Early removal of baby teeth should be carried out only in extreme cases, as this leads to a number of serious problems. First of all, it causes difficulty in the eruption of the main tooth. There is a violation of the development of bite, diction, and facial skeleton, and cosmetic defects are formed. It is very important to prevent destructive processes and, if necessary, remove foci of infection from the oral cavity. The presence of a huge amount of putrefactive and other pathogenic bacteria in a child’s mouth reduces immunity and increases the risk of many diseases. And vice versa, if a child has healthy teeth, he is less likely to catch all kinds of acute respiratory infections, and the risk of gastrointestinal diseases is reduced. Therefore, it is so important to monitor the condition of your child’s teeth. But it is not so easy to bring a child to an appointment with a dentist and persuade him to allow the doctor to do all the necessary manipulations, especially if the child has already had a negative experience, and in such cases modern methods widely used in dentistry come to the rescue.
With the advent of modern sedation technology, dentists can provide their patients with truly stress-free treatment.
In the West, nitrous oxide is most often used in pediatric dentistry - oxygen sedation (NAS). Nitrous oxide is an inert gas with a subtle sweetish odor; when mixed with oxygen, it provides the safest and most harmless sedation for the patient. ZAX has been regularly used in dentistry since 1948, and currently, in 80% of cases in children, this type of sedation is used.
Nitrous oxide is supplied using special equipment. The device is a rotameter that allows you to adjust the ratio of gases in the mixture, a reserve bag, a breathing circuit with a nasal mask and a source of gases (cylinders or a centralized system). The gases exhaled by the patient are evacuated by high-speed suction.
Indications for the use of ZAX in pediatric practice are:
· The need to relieve moderate fear of dental surgery in a child who is capable of cooperation. Usually these are children over 3 years old.
· First treatment at the dentist, which allows you to form a stereotype of a non-scary treatment.
· Increased gag reflex.
· Traumatic interventions (local anesthesia, removal, preparation of carious cavity).
· Long-term treatment.
Contraindications to ZAX are:
· The child has a strong fear after a negative experience of treatment at the dentist and reluctance to contact the doctor.
· The child is too young when he is not ready to cooperate.
· Mental illnesses and intellectual disabilities that impede the ability to come to an agreement with the child.
· Impaired nasal breathing (adenoids, ARVI). The child will breathe through the mouth and will not be able to use the nasal mask.
· Full stomach, as nausea and vomiting may occur. The last meal should be taken 2 hours before the start of sedation.
· Hyperexcitability, since there is a possibility of a paradoxical reaction to sedation.
Having some experience, the doctor, analyzing the child’s behavior during the consultation, can predict what impact the ZAX will have on the patient. It is important to remember that successful use of ZAX is only possible in combination with the use of behavior management techniques. Trying on a mask takes place in a playful way. The doctor explains to the child in an accessible form what will happen to him. It is important to obtain the patient’s voluntary consent to wear a mask: this is the first component of success. In children's practice, scented masks and masks of various colors are used, which makes the choice and the procedure itself more pleasant.
Introduction to a state of sedation begins with the supply of 100% oxygen at a rate of 4-6 l/min, with the gradual addition of nitrous oxide. The permissible concentration of nitrous oxide is 50%. The most optimal ratio at which the planned treatment can be carried out is 30% nitrous oxide and 70% oxygen. However, adjusting the concentration of nitrous oxide depends on the effect, and in each case this is an individual indicator that is recorded in the map. After the start of inhalation, the blood is saturated with gas within 5-7 minutes. The difference between ZAX and other sedative drugs is the rapid onset of sedation and the absence of a trace effect; nitrous oxide is completely eliminated from the body within 5-10 minutes of inhalation.
For the most unpleasant and painful procedures, such as tooth extraction, with a diagnosis of periodontitis, it is possible to temporarily increase the concentration of nitrous oxide up to 50%. Nitrous oxide has an analgesic effect and potentiates the action of local anesthetics. Even if the child is scared or feels discomfort, after the end of the manipulation he quickly calms down and gives the opportunity to calmly continue the treatment. The use of ZAXS allows for complex and fairly long-term treatment. For example, treatment of pulpitis followed by restoration with composite materials or standard crowns in one visit. Completion of work must be carried out on traces of nitrous oxide. The exit from the state of sedation should be smooth and ends with inhalation of 100% oxygen for 5-10 minutes. At this time, the doctor can communicate with the child, reinforcing his positive impressions of visiting the clinic. The effect of ZAX is due to nonspecific depression of the central nervous system.
Comfortable, relaxed state; pleasant mood; soft, relaxed, inhibited body movements; lack of resistance; deep breathing; decreased motor activity of the eyes, easily fixed gaze; decreased perception of sound are all symptoms of sedation. The patient may be disoriented and easily suggestible. The use of ZAX significantly facilitates the treatment process for both the child and the dentist. Children develop a positive attitude towards dental visits, which instills in them a culture of dental health. New prospects open up for the pediatric dentist to provide higher-quality, more extensive, smoother treatment!
Today, 103 dental clinics are registered in Saratov, 12 of them provide children's services. The Praktik dental clinic uses nitrous oxide.
Conclusion: nitrous oxide is one of the most current methods of sedation, helping to make the procedure easier for both the doctor and the patient. This method of anesthesia is common in the USA, Canada, in the West, in the Central cities of Russia, and in Saratov, unfortunately, it is used only in one clinic.